Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
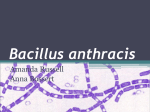
ANTHRAX Typical cutaneous anthrax ulcer on the face of a seventeen year old girl. The patient was from a northern Iranian village where exposure to contaminated soil and livestock products is common; no bioterrorism was suspected. She was cured with intravenous penicillin G (from Mohsen Esfandbod, and Mahdi Malekpour, Clinical Images in Medicine, NEJM, July 9, 2009). Introduction Anthrax is primarily a disease of herbivores. Humans usually become infected when they come into contact with infected animals or their products. Anthrax is primarily an occupational hazard for handlers of processed hides, goat hair, bone products, wool and infected wildlife. It can also be contracted by contact with infected meat, for example in abattoir workers. Anthrax as a biological warfare agent: Anthrax may also be used as a possible biological warfare or biological terrorism agent, most likely spread as an aerosol. Any new case should be assessed with this possibility in mind, particularly but not exclusively in cases of pulmonary anthrax. The deliberate release of anthrax spores through contaminated letters in the USA in October 2001 resulted in 22 cases of anthrax, of which half were cutaneous and half were pulmonary anthrax. There were 5 deaths. Epidemiology ● According to the WHO, anthrax is endemic to animals in much of sub-Saharan Africa and Asia, as well as in some southern European countries, parts of the Americas, and some regions in Australia. ● Epidemics in animals also occur sporadically in other countries around the world. ● Human infection with anthrax occurs less frequently Organism ● Bacillus anthracis, a gram-positive, aerobic rod-shaped bacterium. ● It is encapsulated, spore-forming and non-motile. Spores may lay dormant in the environment for decades. Reservoir ● Spores may remain viable in contaminated soil for many years. ● Dried or processed skins and hides of infected animals may also harbor spores for years. Mode of transmission Anthrax can be transmitted by 3 means: 1. Cutaneous anthrax: This is anthrax introduced through a skin injury. It can occur by contact with: ● Tissues of infected animals such as cattle, horses, and pigs via contaminated hair, wool, hides or products made from them (Hide-porter’s disease). ● Soil associated with infected animals and contaminated bone meal used in some gardening products. ● 2. 3. Possibly by biting flies that have fed on infected animals in some parts of the world but not seen in Australia. Pulmonary anthrax (“woolsorter’s disease”): ● This is anthrax caused by inhalation of aerosolised spores. ● Anthrax has a very low infectious dose: based on animal data, estimates of infectivity via the respiratory route suggest that as few as 1 to 3 spores may cause infection. Intestinal or oropharyngeal anthrax: ● This is anthrax caused by ingestion of contaminated undercooked meat. ● There is no evidence of transmission through the milk of an infected animal. Incubation period ● Cutaneous anthrax: is very short, typically 1 day only, though it may be up to 6 days. ● Pulmonary anthrax: typcially this is 1-7 days although evidence from mass exposures indicates incubation periods of up to 60 days are possible. This is thought to be related to delayed activation of the inhaled spores. ● Gastrointestinal: 3-7 days. Period of Communicability ● There is no evidence of direct spread of anthrax from person to person. ● Articles and soil contaminated with spores may remain infective for years. Susceptibility and Resistance ● Recovery is usually followed by prolonged immunity. Clinical features Anthrax most commonly affects the skin. Less commonly it may affect the lungs or GIT. Cutaneous anthrax Typical cutaneous anthrax lesion. This form accounts for over 95% of anthrax cases. Lesions usually occur on exposed skin and often commence with itchiness. They then pass through several stages: 1. Papular stage. 2. Vesicular stage: ● 3. Blisters form that often become haemorrhagic Eschar stage: ● This appears two to six days after the haemorrhagic vesicle dries to become a depressed ulcer with a black necrotic base, (malignant pustule or “black eschar”) which may have surrounding redness and extensive edema, (see above). Anthrax lesions are usually painless but pain may result due to surrounding oedema. Untreated lesions can progress to involve regional lymph nodes. An overwhelming septicaemia can occur in severe cases. Untreated cutaneous anthrax has a case fatality rate of 5–20% but death is rare with early appropriate treatment. Pulmonary (inhalational) anthrax: This is uncommon. Clinical features include: 1. Fever 2. Non specific consitutional symptoms, (lethargy, malaise, anorexia) 3. Respiratory symptoms: Initial mild cough or chest pain. Followed within 3-6 days by increasing respiratory distress, with hypoxia and high fevers. 4. Meningitis may also complicate this form. The mortality rate approaches 100% with delayed or no treatment. Commencement of appropriate antibiotics during the prodrome significantly decreases the mortality rate. Intestinal/ oropharyngeal anthrax: These are very rare forms of anthrax in developed countries but may occur in large outbreaks in developing countries following ingestion of meat from infected animals. In intestinal anthrax, gastro-intestinal symptoms may be followed by fever, septicaemia and death. Case fatality rates in the range of 25–75% have been reported. In oropharyngeal anthrax, fever, neck swelling due to lymphadenopathy, throat pain, oral ulcers and dysphagia may be followed by severe local ulcers and swelling, septicaemia and death. Case fatality rates are similar to the intestinal form. Investigations 1. Microscopy and Culture: ● Isolation of Bacillus anthracis from blood, skin lesions or sputum. 2. PCR testing. 3. CXR ● For suspected pulmonary anthrax Others as clinically indicated. Management Antibiotics: For cutaneous anthrax, use oral: ● Ciprofloxacin Or ● Doxycycline These can also be used initially for post inhalational exposure prophylaxis. Pulmonary and GIT anthrax will require far more intensive combination chemotherapy, and specialist advice will need to be sought. Immunization: ● High risk persons, include laboratory workers who are liable to handle B. anthracis. ● These may be immunized with the cell-free vaccine giving annual boosters as recommended. ● Protection is likely to be greater against cutaneous exposures than pulmonary exposures. ● The vaccine is not currently licensed for use in the general community. Notification ● Anthrax infection (Group A disease) must be notified immediately by telephone or fax and followed by written notification within five days. School exclusion ● School exclusion is not required.