Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
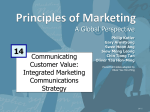
Bruyere_Case09_001-008.qxd 6/26/08 6:10 PM Page DS9-1 CAS E STU DY 9 PULMONARY THROMBOEMBOLISM For the Patient Case for this case study, see the printed book. DISEASE SUMMARY Definition Pulmonary thromboembolism (PTE), also known as pulmonary venous thromboembolism, is not a disease but a common, serious, and potentially fatal complication of deep vein thrombosis (DVT). With PTE, venous thrombi (i.e., blood clots) detach from their sites of origin on blood vessel walls, travel through the blood to the lungs, obstruct blood vessels, and reduce blood flow. Most pulmonary thromboemboli (⬎95%) arise in the deep veins of the lower extremities. Clinical manifestations depend on the size of the embolus and its site of impact. Large emboli can be fatal. Most emboli are multiple and the lower lobes of the lungs are more commonly involved due to a more extensive circulation. Prevalence Venous thrombosis affects as many as 2 million people in the United States every year. Approximately 650,000 patients develop PTE annually, resulting in a quarter-million hospitalizations. Pulmonary thromboembolism occurs in 60–80% of patients with DVT, even though more than half the patients are asymptomatic. Sixty percent of patients who die in the hospital have experienced PTE. Because patients with PTE present with non-specific clinical manifestations, the diagnosis is missed in approximately 400,000 individuals in the United States each year. Virtually every primary healthcare provider encounters patients who are at risk for PTE. Subtle population differences exist in the incidence of PTE, but the frequency is high in all racial groups. PTE is common in all trimesters of pregnancy and in the immediate postpartum period. A 30-year, population-based study revealed that PTE occurred in 160/100,000 women in the postpartum period and in 11/100,000 women during pregnancy. The incidence of PTE is also increased in women receiving oral contraceptive or hormone replacement therapy, but gender alone is not an independent risk factor. Although the frequency of PTE increases with age, age is not an independent risk factor. Rather, the accumulation of other risk factors, such as underlying illness and decreased mobility, causes the increased frequency of PTE in older patients. DS9-1 Case Study 9 ■ Pulmonary Thromboembolism Bruyere_Case09_001-008.qxd 6/26/08 6:10 PM Page DS9-2 Significance Massive PTE is second only to sudden cardiac death from coronary artery disease as a cause of unexpected death. Furthermore, PTE is currently the third most common cause of death in hospitalized patients and the sole or a major contributing cause of death in approximately 10% of adults who die acutely in hospitals. The highest incidence of PTE occurs among hospitalized patients. An estimated number of 50,000–100,000 deaths occur annually as a result of PTE, and the overall mortality rate continues to be significant (15–17.5%). Undiagnosed and untreated PTE carries an even higher mortality rate of 30%. The development of pulmonary arterial hypertension that often leads to right heart failure (cor pulmonale) is a serious complication of PTE. In addition, the patient who has had one episode of PTE is at high risk for having more and also has a high probability for developing recurrent, non-healing skin ulcers of the lower extremities from DVT. PTE is also the most frequent cause of maternal death associated with childbirth. Causes and Risk Factors The causes of PTE are multifactorial and, in many patients, are not readily apparent. Persons at risk for developing DVT are also at risk for developing PTE. Back in the 19th century, a pathologist named Virchow identified three major factors that predispose patients to thrombus formation and increase their risk for PTE. The three factors, collectively known as the Virchow triad, are venous stasis (i.e., sluggish blood flow), hypercoagulability of the blood, and injury to the endothelial lining cells of veins. Specific examples of conditions that promote venous stasis are: prolonged bedrest, heart failure, cardiac dysrhythmias, and dehydration. Conditions that predispose to a hypercoagulable state of the blood include the following: • use of estrogens in oral contraceptives and hormone replacement therapy • pregnancy • polycythemia (i.e., elevated hematocrit from increased erythropoiesis, often the result of living at high altitude) • cancer • cigarette smoking • deficiency of protein S or antithrombin III, both of which have antithrombotic properties Factor V Leiden mutation is present in approximately 5% of the population and is the most common cause of familial PTE. The risk of PTE among users of oral contraceptives is approximately three times the risk of that of non-users. The combination of oral contraceptive use and cigarette smoking poses an especially high risk for both DVT and PTE. Specific examples of conditions that injure the linings of veins are inflammation of the veins (i.e., phlebitis), blunt trauma, bone fractures that cause significant soft tissue injury, certain surgical procedures, and burns. The most common risk factors for PTE are long periods of inactivity, trauma, pregnancy, cancer, heart failure, estrogen use, and a strongly positive family history for DVT or PTE. Pathophysiology A thrombus is an intravascular blood clot composed of platelets and red blood cells enmeshed in a network of fibrin. The process of thrombus formation is known as thrombosis and is considered the pathophysiologic counterpart of normal hemostasis, which occurs with laceration or rupture of a blood vessel. Thrombosis is the ultimate result of a complex series of events that occurs without hemorrhage and often without significant injury. With even slight denudation of the inner lining of a vein, platelets can attach at the site of injury, secrete chemical factors that attract more platelets, and convert fibrinogen to fibrin. Slowly moving red blood cells become enmeshed in the network of the developing thrombus and the clot increases in size (i.e., propagation). DS9-2 Case Study 9 ■ Pulmonary Thromboembolism Bruyere_Case09_001-008.qxd 6/26/08 6:10 PM Page DS9-3 Most venous thrombi form as a result of long periods of inactivity, increased concentrations of clotting factors in the blood, certain medical conditions, and injuries to veins. Muscular activity promotes blood flow. Inactivity caused by prolonged bedrest and long plane rides or automobile trips decreases the flow of blood in the legs, making thrombi more common. People who are immobilized for long periods of time after surgery, a heart attack, or a serious injury are more likely to develop thrombi and PTE than are patients who are bedridden for only short periods. In recent years, attention has focused on increased rates of DVT and PTE among otherwise healthy travelers on long plane trips. Cramped seats with minimal legroom have contributed to the problem—so much so that DVT is sometimes referred to as “economy class syndrome.” Some types of cancer (especially pancreatic, lung, and ovarian) cause increased blood levels of procoagulants (substances that promote clotting) when cancer cells secrete chemicals that activate coagulation factors. Estrogens contained in birth control pills and hormone replacement medications also increase the concentrations of clotting factors in the blood. People who have cardiovascular disease associated with thrombosis (i.e., heart attacks and strokes) are also more likely to develop PTE. Injury to veins often occurs during certain surgical procedures (especially hip or knee replacements), from direct injury to the legs, or from leg or pelvic fractures. Once venous thrombi form they have several fates: 1. they can be lysed by natural fibrinolytic enzymes released by endothelial cells 2. they can remain stationary for many years and even become incorporated into the blood vessel wall where they developed 3. they can fragment, and migrate through the blood to the right side of the heart and into pulmonary arteries, eventually obstructing blood flow Thrombi can be dislodged from their point of origin by trauma, the effect of exercise and muscle action, and changes in blood flow. However, it is impossible to accurately predict which clot will dislodge or when it will dislodge. PTE can arise from DVT anywhere in the body. Fatal PTE occasionally results from a thrombus that originates in the axillary or subclavian veins (deep veins of the arm and shoulder) or in the veins of the pelvis. A thrombus that forms around indwelling central venous catheters is also a potential cause of fatal PTE. Thrombi that develop in superficial (i.e., near the skin) veins, such as the saphenous vein, tend to remain stationary. However, thrombi that form in deep leg veins, especially within the calves, tend to embolize easily. A thrombus in the popliteal segment of the femoral vein (behind the knee) is the cause of PTE in more than 60% of cases. Large emboli may impact at the bifurcation of the main pulmonary artery, resulting in obstruction to blood flow in both the right and left pulmonary arteries. This type of PTE is known as a saddle embolus, will cause severe and immediate strain on the right ventricle, and is a cause of sudden and unexpected death. A large saddle embolus located at the bifurcation of the main pulmonary artery is shown in Disease Summary Figure 9.1. Smaller thrombi continue traveling into smaller arteries in the lung, impacting and causing either a small hemorrhagic lung infarct (i.e., cell death due to insufficient blood flow) or, if the embolus is extremely small, resulting in no clinical manifestations whatsoever. The effects of PTE on the pulmonary circulation are related to obstruction of blood flow by the embolus and neurohumoral reflexes causing vasoconstriction, which further compromises pulmonary blood flow. Pulmonary thromboemboli result in two major pathophysiologic consequences: respiratory compromise owing to the non-perfused, although perhaps well-ventilated, segment of lung in which obstruction has occurred and hemodynamic compromise from increased resistance to pulmonary blood flow. Acute respiratory consequences include increased alveolar dead space, hypoxemia, and hyperventilation. Obstruction to pulmonary blood flow also causes reflex bronchoconstriction in the affected area of lung, wasted ventilation, reduced gaseous exchange, and loss of alveolar surfactant. Arterial hypoxemia is a frequent but not universal finding in patients with acute PTE. Pathophysiologic mechanisms that cause hypoxemia include ventilation-perfusion mismatch and reduced cardiac output. PTE, and especially multiple emboli, reduce the cross-sectional area occupied by functional pulmonary vasculature. This results in an increase in both pulmonary vascular resistance and right ventricular workload (so-called pulmonary hypertension). Increased right ventricular workload may lead to right heart failure (RHF). Pulmonary infarction is a potential but also uncommon consequence of decreased pulmonary blood flow because bronchial arterial blood flow provides a second circulation to the lungs. DS9-3 Case Study 9 ■ Pulmonary Thromboembolism Bruyere_Case09_001-008.qxd 6/26/08 6:10 PM Page DS9-4 DISEASE SUMMARY FIGURE 9.1 The main pulmonary artery and its bifurcation have been opened to reveal a large saddle embolus. (Reprinted with permission from Rubin E, Farber JL. Pathology. 3rd Ed. Philadelphia: Lippincott Williams & Wilkins, 1999.) DS9-4 Case Study 9 ■ Pulmonary Thromboembolism Bruyere_Case09_001-008.qxd 6/26/08 6:10 PM Page DS9-5 Diagnosis: Clinical Manifestations and Laboratory Tests The clinical diagnosis of PTE is notoriously difficult to make and often missed for several reasons: 1. Most patients with PTE have no obvious symptoms at presentation. 2. Common signs and symptoms of PTE are not specific. 3. Patients with PTE may present with a variety of atypical symptoms (e.g., fever ⬍102°F, abdominal pain, and a productive cough). A thorough medical history is important and the clinician should be highly suspicious when certain clinical manifestations combined with risk factors for PTE are noted. Based on the suddenness of onset and severity of pulmonary arterial obstruction, the presentation of patients with PTE can be categorized into four groups: 1. With massive pulmonary embolism, large emboli compromise pulmonary blood flow and produce circulatory collapse and shock. The patient presents with systemic hypotension (i.e., systolic blood pressure ⬍90 mm Hg), weakness, pallor, diaphoresis, oliguria (i.e., urine output ⬍400 mL/24 hours), tachycardia, tachypnea, cold extremities, and impaired mentation. 2. With acute pulmonary infarction (i.e., cell death from insufficient blood flow) caused by obstruction of a peripheral pulmonary artery, patients present with sudden onset of chest pain that is more severe with deep inspirations, dyspnea (i.e., breathlessness), decreased excursion (i.e., movements of the diaphragm), audible pleural friction rub, dullness with percussion due to pleural effusion, and hemoptysis (i.e., coughing up blood-stained sputum). Although the pain may be sharp, stabbing, and indistinguishable from angina pectoris due to myocardial ischemia, it is associated with a normal electrocardiogram and negative response to nitroglycerin. 3. With acute PTE in which there is no infarction, patients present with non-specific symptoms of dyspnea, substernal discomfort, tachypnea, and/or tachycardia. 4. Patients with multiple pulmonary emboli present in one of two manners: (a) Patients who have had repeated, documented episodes of PTE present with features of pulmonary hypertension and RHF, i.e., elevated jugular venous pressure, right ventricular S3 gallop, ascites, hepatomegaly, and dependent pitting edema. (b) Patients who have not had previously documented PTE but have widespread obstruction of the pulmonary vasculature by emboli present with gradually progressive dyspnea, intermittent chest pain with exertion, and, eventually, features of pulmonary hypertension and RHF. The most common symptoms of PTE are dyspnea (72–84% of all patients) and pleuritic chest pain (59–74%). The most common sign is tachypnea (68–92%). At least one of these clinical manifestations is present in 97% of patients with angiographically confirmed PTE. Other common clinical manifestations associated with PTE are shown in Disease Summary Table 9.1. Although they may provide information that suggests a differential diagnosis, routine laboratory blood test results are non-specific and not helpful to diagnose PTE. Arterial blood gases characteristically reveal hypoxemia, hypocapnia, and respiratory alkalosis. Initially, chest x-rays are normal. However, as the course of PTE advances, chest radiography may reveal dilation of pulmonary vessels, atelectasis, slight pleural effusion, and an elevated diaphragm. Profound hypoxia with a normal chest x-ray in the absence of pre-existing lung disease strongly suggests PTE. Ventilation/perfusion (V/Q) scanning of the lungs is an important procedure for establishing diagnosis. A perfusion scan is performed by injecting radiolabeled microaggregates of albumin into the venous circulation and allowing the particles to embolize to pulmonary capillary beds. With ventilation scanning, the patient breathes a radioactive gas or aerosol while the distribution of radioactivity in the lungs is monitored. Abnormalities in the perfusion scan are interpreted in conjunction with the ventilation scan to determine a probability that PTE is the cause of abnormal findings. In 96% of cases, a normal V/Q scan indicates an absence of PTE. Patients with two or more segmental defects or one large perfusion defect in the presence of a normal x-ray and normal ventilation scan have an 88% probability for PTE. Among patients with a high clinical pretest probability, the likelihood for PTE increases to 95%. DS9-5 Case Study 9 ■ Pulmonary Thromboembolism Bruyere_Case09_001-008.qxd 6/26/08 6:10 PM Page DS9-6 Disease Summary Table 9.1 Frequencies of Common Clinical Manifestations Associated With Pulmonary Thromboembolism Common Clinical Finding in PTE Frequency (%) Sinus tachycardia 70 Crackles in the lungs 40–58 Cough 36–53 Heart rate ⱖ100/min 24–44 Leg pain 24–26 Accentuated pulmonary component of second heart sound 13–53 Fourth heart sound (S4) 13–24 Palpitations 10–18 Wheezing 9–11 Hemoptysis 8–30 Elevated body temperature 7–43 Adapted with permission from Chesnutt MS, Prendergast TJ. Pulmonary venous thromboembolism. In: McPhee SJ, Papadakis MA, Tierney LM, Jr., eds. 2007 Current Medical Diagnosis and Treatment. 46th Ed. New York: McGrawHill, 2007;Table 9-20:286.) Non-invasive tests for lower extremity DVT may be helpful in the evaluation of patients who cannot be diagnosed with V/Q scans. Color-flow Doppler imaging and compression ultrasonography have a high sensitivity (89–100%) and specificity (89–100%) for detection of DVT in symptomatic patients. Inability to compress the common femoral or popliteal veins in symptomatic patients is diagnostic of first-episode DVT. Full compressibility at both sites excludes DVT. The role of spiral CT (i.e., computed tomography) scanning in diagnosing PTE has evolved significantly during the past decade and is rapidly replacing V/Q scanning as the initial diagnostic procedure for suspected PTE. Spiral CT can visualize central, lobar, and segmental emboli with a sensitivity ⬎90% and detect emboli as small as 2 mm. A combined CT scan for PTE/DVT enhances the utility of spiral CT scans by further identifying obstructions in the deep venous system of the lower extremities or pelvic veins. Pulmonary angiography remains the reference standard for the diagnosis of PTE, and a definitive diagnosis is established 97% of the time. Following injection of an iodinated contrast dye, anteroposterior, lateral, and oblique images are obtained from each lung. Positive results consist of an abrupt arterial cutoff of an affected artery. Non-occlusive emboli produce a so-called “tram-track” appearance. Angiography is generally a safe procedure, with a mortality rate ⬍0.5% and a morbidity rate ⬍5%. Major complications of the procedure include allergic reactions to the dye and adverse effects from catheter insertion. Magnetic resonance imaging (MRI) has a sensitivity of 85% and a specificity of 96% for central, lobar, and segmental emboli but is inadequate for the diagnosis of subsegmental emboli. Furthermore, MRI is expensive, not widely available, and may create artifacts that limit its use in diagnosing PTE. The integrated approach to diagnosis employs the clinical likelihood of PTE in conjunction with results of non-invasive testing to arrive at one of three decision points: to establish PTE or DVT as the diagnosis, to exclude PTE and DVT with sufficient evidence, or to refer the patient for pulmonary angiography. Appropriate Therapy Patients with suspected or confirmed PTE are given supplemental oxygen or ventilator support with immediate activity limitations to reduce oxygen demand. Immediate full anticoagulation is mandatory. Diagnostic studies should not delay empirical anticoagulant therapy. Initial anticoagulation is performed with intravenous heparin, which activates antithrombin III to prevent the propagation of DVT and pulmonary emboli. The efficacy of heparin therapy depends on achieving a critical therapeutic level of heparin within the initial 24 hours of treatment. The critical therapeutic level is 1.5 times the baseline control value or the upper limit of normal range of the activated partial thromboplastin time (aPTT). Lower molecular weight heparins (LMWHs) have many advantages over unfractionated heparin: DS9-6 Case Study 9 ■ Pulmonary Thromboembolism Bruyere_Case09_001-008.qxd 6/26/08 6:10 PM Page DS9-7 • • • • • • significant bioavailability can be administered by subcutaneous injection have a longer duration of action fixed doses can be given monitoring of aPTT is unnecessary are equally effective and as safe as unfractionated heparin In some cases, anticoagulation therapy may reduce mortality rate from 30% to less than 10%. Patients should be started simultaneously on oral anticoagulation with warfarin. The anticoagulant effect of warfarin is mediated by the inhibition of vitamin K-dependent coagulation factors (i.e., II, VII, IX, and X). The recommended therapeutic range for PTE is an international normalized ratio (INR) of 2–3. A therapeutic dose of warfarin is usually established within 4–5 days. Heparin is then discontinued and warfarin therapy is maintained. Patients with an initial episode of PTE and reversible risk factors (e.g., immobilization, surgery, or trauma) should receive warfarin for 3–6 months. In the absence of an identifiable risk factor, patients should be treated for at least 6 months. Long-term anticoagulation is required for patients with recurrent PTE or persistent risk factors, such as a factor V Leiden mutation. Until randomized clinical trials demonstrate a clear morbidity or mortality benefit, the role of thrombolytic therapy in the management of acute PTE remains controversial. Currently accepted indications for thrombolytic therapy include hemodynamic instability (e.g., shock) or right ventricular dysfunction demonstrated with echocardiography. Currently available thrombolytic regimens include alteplase, reteplase, urokinase, and streptokinase. The safety of these thrombolytics is comparable. However, comparative trials have demonstrated that administration of a 1-hour infusion of alteplase is more rapidly effective than 12-hour infusions with urokinase or streptokinase. Inferior vena cava (IVC) interruption by the insertion of an IVC filter is indicated in patients with acute PTE who have an absolute contraindication to anticoagulant therapy and in those with recurrent PTE despite anticoagulant therapy. If hemodynamic consequences are life-threatening and the patient has refractory hypotension, an embolectomy (i.e., surgical removal of the embolus) may be performed on an emergency basis. However, the mortality rate is very high and this is a procedure of last resort. Prevention is critical for patients who are at risk for DVT and PTE. Walking and activity as soon as possible after surgery or during a long illness can reduce risk. If the patient is bedridden for a prolonged time, range-of-motion exercises and low-dose subcutaneous heparin sodium or LMWHs may be used. Compression stockings are a safe and effective prophylactic in patients who are high risk when heparin therapy is not desirable or is contraindicated. These devices provide a gradient of compression that is highest at the toes and gradually decreases up to the thigh. Compression stockings increase blood flow velocity at least five-fold in lower extremity veins. Serious Complications and Prognosis Prognosis of PTE depends on the patient’s underlying disease state and appropriate diagnosis and treatment. Most patients treated with anticoagulants do not develop long-term complications. At 5 days of anticoagulant therapy, 36% of lung scans are resolved; this percentage doubles at 3 months. In a small proportion of patients, PTE does not resolve and pulmonary hypertension develops. The mortality rate ranges from 14 to 25% and depends on the size of the embolus and the site of impact and obstruction. Death from recurrent PTE occurs in ⬍3% of all cases. Major complications include sudden cardiac death, shock, pulmonary hypertension, RHF, recurrent DVT and PTE, and severe hypoxemia. Suggested Readings Brashers VL. Pulmonary embolism. In: McCance KL, Huether SE, eds. Pathophysiology: The Biologic Basis for Disease in Adults and Children. 5th Ed. St. Louis: Elsevier Mosby, 2006:1232–1234. DS9-7 Case Study 9 ■ Pulmonary Thromboembolism Bruyere_Case09_001-008.qxd 6/26/08 6:10 PM Page DS9-8 Chesnutt MS, Prendergast TJ. Pulmonary venous thromboembolism. In: McPhee SJ, Papadakis MA, Tierney LM Jr., eds. 2007 Current Medical Diagnosis and Treatment. 46th Ed. New York: McGraw-Hill, 2007:284–294. Feied C, Handler JA. Pulmonary embolism. eMedicine website. Available at: www.emedicine. com/EMERG/topic490.htm. Date accessed: June 2006. Husain AN, Kumar V. Pulmonary embolism, hemorrhage and infarction. In: Kumar V, Abbas AK, Fausto N, eds. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia: Elsevier Saunders, 2005:742–743. Kaufman DA. Pulmonary embolus. MedlinePlus Medical Encyclopedia website, National Library of Medicine and National Institutes of Health. Available at: www.nlm.nih.gov/ medlineplus/ency/article/000132.htm. Date accessed: March 2007. Mayo Clinic staff. Pulmonary embolism. Mayo Clinic website. Available at: www.mayoclinic. com/health/pulmonary-embolism/DS00429. Date accessed: September 2005. Mitchell RN. Pulmonary thromboembolism. In: Kumar V, Abbas AK, Fausto N, eds. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia: Elsevier Saunders, 2005:136. Pace B. Pulmonary embolism. J Amer Med Assoc 2001;285:836. Porth CM. Pulmonary embolism. In: Porth CM, ed. Pathophysiology—Concepts of Altered Disease States. 7th Ed. Philadelphia: Lippincott Williams & Wilkins, 2005:712–713. Schumann L. Pulmonary embolism. In: Copstead LEC, Banasik JL, eds. Pathophysiology. 3rd Ed. St. Louis: Elsevier Saunders, 2005:577–579. Sharma S. Pulmonary embolism. eMedicine website. Available at: www.emedicine.com/med/ topic1958.htm. Date accessed: June 2006. DS9-8 Case Study 9 ■ Pulmonary Thromboembolism