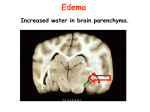
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
INDEX www.yassermetwally.com
INTRODUCTION
NORMAL ANATOMY
TYPES OF ACQUIRED HERNIATIONS
IMAGING OF ACQUIRED CEREBRAL HERNIATIONS
The cranium provides protection for the brain against external forces, The brain is suspended in the cerebrospinal fluid (CSF) and
supported by the skull and dural septa, which divide the cranial cavity into compartments and prevent excessive movement of the brain
[1]. The unyielding cranium is a closed system and hence there is a fixed volume for the brain, CSF, and blood vessels and very little
room for expansion in the face of increased intracranial volume and pressure. The brain is essentially incompressible (its shape can be
altered, but its volume is basically constant); therefore, the vascular and CSF spaces must compensate for alterations in intracranial
volume because of mass lesions or cerebral edema [2,3]. Unfortunately, this capacity is very limited, and when it is exceeded, cerebral
displacement and herniation result. Cerebral herniation is the displacement of brain tissue from one compartment to the other. Of
course, there are numerous variables that influence the degree of herniation and its untoward neurologic effects, such as the location of
the mass, the volume of the mass, the intracranial pressure, the rate at which alterations in pressure and volume develop, brain atrophy,
and individual anatomical variations.
There are several different types of cerebral herniation and these are defined by the anatomic boundary through which the herniating
tissue traverses [1,4]. Subfalcine, transtentorial, and tonsillar herniation are well known. Transtentorial herniation can be further
classified as central (ascending and descending) and lateral (anterior and posterior).
Transphenoidal and external hernias are less well- known patterns of herniation. A thorough understanding of the anatomy of the brain,
skull, and total septa is imperative to understanding cerebral displacement and herniation (5]. Recognition of cerebral displacement and
herniation is critical, because the clinical consequences are devastating. Cerebral herniation causes compression of the brain, cranial
nerves, and blood vessels and results in serious neurologic morbidity and even death.
ANATOMY
The cranial cavity is incompletely divided into fossae by bony ridges and further divided by dural septa. The base of the skull provides
support for the brain and consists of three fossae: anterior, middle and posterior, which are separated by bony ridges. The foramen
magnum is a large orifice in the floor of the posterior fossa that allows passage of the spinal cord, nerves and blood vessels. Although
there are numerous skull base foramina, the foramen magnum is the only opening of any significant size.
The dural septa represent reflections of the dura mater that further divide the intracranial cavity. Dura is the Latin word for hard, an
accurate description of this tough, fibrous membrane. The two main dural reflections are the falx cerebri, which separates the cerebral
hemispheres, and the tentorium cerebelli, which separates the posterior fossa from the cerebral hemispheres defining the supratentorial
and infratentorial compartments. The falx cerebella is a smaller dural reflection, which partially separates the cerebellar hemispheres.
Figure 1. Patterns of cerebral herniation. (A) Coronal, (B) axial, and (C) sagittal diagrams demonstrate the different types of cerebral
herniation: (1) Subfalcine, (2) uncal, (3) descending transtentorial, (4) tonsillar, (5) ascending transtentorial, and (6) external herniation.
Figure 2. Patterns of cerebral herniation.
The falx cerebri is a sickle-shaped septum that attaches anteriorly to the crista galli, and posteriorly to the internal occipital
protuberance and tentorium cerebella. The anterior part of the falx cerebri has a relatively narrow sagittal width, whereas the posterior
part of the falx cerebri has a broad sagittal width where it attaches to the tentorium cerebella and contains the straight sinus [6,7].
Superiorly, the falx cerebri attaches to the inner table of the skull in the midline and contains the superior sagittal sinus, whereas the
inferior free edge of the falx cerebrei contains the inferior sagittal sinus [6]. The corpus callosum is located immediately inferior to the
free edge of the falx and the distance between the two decreases posteriorly. The cingulate gyros is just lateral to the inferior aspect of
the falx. The pericallosal artery, a branch of the anterior cerebral artery, runs in the pericallosal sulcus between the corpus callosum
and cingulate gyrus [6].
Figure 3. Dural reflections. Diagram of the cranial dural reflections and tentorial incisura.
The tentorium cerebella is a transverse dural septum that separates the posterior fossa from the cerebral hemispheres. The tentorium, as
its name suggests, is shaped like a tent, with its apex suspended in the midline by the posterior inferior falx cerebrei, and the base
attached to the inner surface of the occipital bone and upper border of the petrous temporal bone [7]. The transverse sinuses and
superior petrosal sinuses are contained within these basal dural attachments. The opening of the tentorium is the tentorial incisor, also
known as the hiatus or notch. The incisor has a semioval shape and is attached at its base to the clinoid processes and at its apex to the
falx cerebrei [6,7]. Otherwise, the margins of the incisura are free, though quite rigid. The midbrain and cerebral peduncles pass
through the incisura.
Figure 4. Normal anatomy. (A) Coronal T2-weighted MR image demonstrates the falx cerebrei (large black arrow), the cingulate gyros
(outlined arrow), corpus callosum (circle) and tentorium cerebri (small black arrows). (B) Axial T1-weighted MR image demonstrates
the uncus (outlined arrow) and hippocampal gyrus (black arrow).
The anatomy of the tentorial incisor and adjacent structures is complex. The uncus and hippocampus of the medial temporal lobe
slightly overhang the incisura. The posterior cerebral arteries, anterior choroidal arteries, and internal cerebral veins pass around the
midbrain in the ambient cistern in close proximity to the free edge of the tentorium. The oculomotor nerve exits the midbrain and
crosses the interpeduncular cistern between the posterior cerebral and superior cerebellar arteries, and courses just medial to the uncus
on its way to the cavernous sinus. Both computed tomography (CT) and magnetic resonance (MR) imaging demonstrate the anatomy of
the cranial cavity and enable diagnosis of cerebral herniation, although MR imaging provides superior anatomic detail.
TYPES OF ACQUIRED HERNIATIONS
Subfalcine herniation
Subfalcine herniation, also known as midline shift or cingulate herniation, is the most common type of cerebral herniation and is easily
recognized on CT and MR imaging. It is caused by unilateral frontal, parietal, or temporal lobe mass effect or edema [I]. When
subfalcine herniation occurs, the anterior falx, although rigid, will tilt away from the mass effect. The posterior falx is wider, more rigid,
and more resistant to displacement. This explains why subfalcine herniations occur anteriorly. As the mass effect increases, the
ipsilateral cingulate gyros will be displaced beneath the free edge of the falx cerebrei, pushing down the ipsilateral corpus callosum.
With further progression, the contralateral cingulate gyrus and contralateral corpus callosum are compressed [2]. These findings are
best demonstrated on coronal MR imaging. When subfalcine herniation becomes severe, both foramina of Monro become compressed
and obstructed. This results in dilatation of the contralateral lateral ventricle, but the ipsilateral ventricle usually remains compressed
because of mass effect. A wedge of pressure necrosis may occur where the cingulate gyros is squeezed against the falx [2]. Also, the
pericallosal artery may be pressed against the unyielding falx, resulting in occlusion and brain infarction [8,9].
Figure 5. Subfalcine herniation (arrows). Subfalcial herniation is displacement of the cingulate gyrus from one hemisphere to the other,
under the falx cerebri. Subfalcial herniation can compress the pericallosal arteries, causing an infarct in their distribution.
Figure 6. Subfalcine herniation. Coronal enhanced Tl- weighted MR image demonstrates a large enhancing mass (large arrow) within
the left frontal lobe causing subfalcine herniation. The cingulate gyrus (outline arrow) is displaced beneath the falx cerebrei (small black
arrow) and there is downward displacement of the corpus callosum (circle).
Quantification of the degree of midline shift is most easily done by measuring the degree of displacement of the septum pellucidum from
the midline, on axial images with either CT or MRI. The midline is usually determined by halving the distance between the inner tables
at the level of the septum pellucidum. The degree of septal shift, not surprisingly, is predictive of patient prognosis [10-12]. Ross et al
[12] reported that greater midline shift on CT scans correlated with a significantly lower likelihood of recovery in patients with acute
intracranial hematomas. All patients in their series with a septal shift over 15 mm had a poor outcome. Conversely, no patient with
septal shift less than 5 nun shift had a poor outcome. Pineal shift and aqueductal shift appear to have less predictive value [12].
Figure 7. Subfalcine herniation. Axial CT scan reveals a large acute subdural hematoma (large arrow) causing subfalcine herniation.
Note the displacement of the anterior falx cerebrei (small arrow) and extensive midline shift. The ipsilateral ventricle is compressed due
to mass effect, but the atrium of the contralateral lateral ventricle (outlined arrow) is dilated due to obstruction of the foramen of
monro.
Figure 8. This is a trauma case where a contusion of the inferior temporal lobe (blue arrow) has resulted in diffuse hemispheric edema.
Note the compressed and flattened gyri on the right. This has resulted in subfalcine herniation of the cingulate gyrus, with a secondary
hemorrhagic infarction above that (black arrow). A midline shift from right to left is also present, as is uncal herniation.
Transtentorial herniation
Transtentorial herniation occurs when brain tissue is displaced into the tentorial notch, and is perhaps the most important herniation
phenomenon in terms of frequency and clinical consequences. Transtentorial herniation is a complex process that can be loosely
classified into overlapping pattens. Lateral transtentorial herniation can be anterior (uncal) or posterior (parahippocampal); whereas
central transtentorial herniation can be either ascending or descending. Only a few millimeters of space are present between the
midbrain and rigid tentorial edge, and the oculomotor nerve and posterior cerebral artery are in close proximity [5,13]. Consequently,
very little displacement can be tolerated, and a shift of a few millimeters will result in compromise of these vital structures, with serious
neurologic sequelae.
Uncal herniation
Figure 9. Uncal herniation. (A) Axial and (B) coronal Tl- weighted MR images after the administration of gadolinium demonstrate a
large enhancing temporal lobe mass causing herniation of the uncus (arrow) into the suprasellar cistern.
Uncal herniation represents anterior lateral transtentorial herniation. It is perhaps the best-known type of transtentorial herniation and
is readily identified on both CT and MR. Uncal herniation typically occurs from a unilateral, expanding supratentorial lesion, especially
in the middle cranial fossa. In this patten of herniation, the uncus is displaced over the free edge of the tentorium [14]. Consequently, the
midbrain is displaced and the opposite cerebral peduncle is squeezed against the contralateral tentorial edge. This damages the
descending corticospinal and corticobulbar tracts, resulting in paralysis on the same side of the supratentorial mass. This "falselocalizing" sign occasionally resulted in surgery on the wrong side of the brain in the days before CT [15]. The groove where the
midbrain is compressed against the contralateral tentorial edge is known as Kemohan's notch after the author who first described it
[16]. Mass effect on the ipsilateral cerebral peduncle can also lead to a contralateral hemiparesis. As herniation progresses, the midbrain
is further compressed, narrowing it in the transverse dimension, which can affect the ascending reticular activating system and result in
progressive loss of consciousness. Compression of the oculomotor nerve results in ipsilateral third nerve palsy ("blown pupil"). If the
posterior cerebral artery is compressed, infarction of the occipital lobe ensues and produces homonymous hemianopsia, though by this
time the patient is usually unconscious (2,17]. Rarely, the anterior choroidal and superior cerebellar arteries may be compromised,
resulting in infarction [5].
Figure 10. This photo was taken looking at the inferior side of the brain with the brainstem removed at the level of the midbrain. The
herniated uncus is bulging over the position of the tentorium (black arrows) and compressing the midbrain. The two mammillary bodies
(blue arrows) have been shifted to the patients right due to the pressure.
Figure 11. A, This figure represents a view of the ventral part of both cerebral hemispheres. The brain stem has been removed at the
mid brain level. The occipital lobes shows the dura representing the tentorium of the cerebellum. There is bilateral herniation of the
hippocampal gyri (arrows). B, The right hippocampus (seen on the left side of the photograph) shows the larger herniation. Uncal
(transtentorial) herniation is herniation of the medial temporal lobe from the middle into the posterior fossa, across the tentorial notch.
The uncus of the temporal lobe is forced into the gap between the midbrain and the tentorium.
Uncal herniation is well demonstrated on both CT and MRI [18-20]. Early on there is displacement of the uncus, resulting in effacement
of the lateral suprasellar cistern. As herniation progresses, there is widening of the ipsilateral ambient and lateral Pontine cistern, with
displacement and rotation of the brainstem. With more advanced herniation, there is obliteration of the cisternal spaces, and the
midbrain becomes compressed and elongated in the anteroposterior dimension.
Posterior (parahippocampal) tentorial herniation
In patients with occipital and posterior temporal masses, the herniation of the medial temporal lobe occurs more posteriorly.
Consequently, the herniating hippocampus impinges less upon the cerebral peduncle, but more on the tectum at the level of the superior
colliculus [21]. This may result in Parinaud's syndrome, with paralysis of upward conjugate gaze. There is also relatively less
compression of the oculomotor nerve and posterior cerebral artery. However, as herniation becomes more severe, these structures will
be compromised. Early on, MR and CT will demonstrate effacement of the ipsilateral quadrigeminal plate and ambient cisterns, while
there is usually no effacement of the lateral suprasellar cistern. Compression of the tectum and rotation of the midbrain can be seen as
herniation progresses, and finally the cisternal spaces will be obliterated and the midbrain displaced and deformed. Compared with
uncal herniation, this patten of herniation appears to be much less commonly recognized as an isolated clinical presentation. In many
cases there is overlap of uncal and hippocampal herniation.
Figure 12. Uncal and hippocampal herniation. Axial T2- weighted MR image of the brain demonstrates uncal and hippocampal
herniation due to multiple abscesses in the right temporal and occipital lobes. The largest abscess is in the occipital lobe resulting in
parahippocampal herniation (black arrow) and compression of the right midbrain tegmentum (outlined arrow).
Descending transtentorial herniation
Descending transtentorial herniation consists of caudal descent of brain tissue through the tentorial incisura, and occurs mainly in
response to mass effect in the frontal, parietal, and occipital lobes [1]. Since intracranial masses are rarely in the midline, there is
considerable overlap of horizontal and vertical shifts during transtentorial herniation; such that descent of the diencephalon, midbrain,
and pons tends to occur simultaneously with uncal and hippocampal herniation. Furthermore, with unilateral lesions, subfalcine
herniation commonly precedes transtentorial herniation; whereas midline masses, bilateral supratentorial masses, or supratentorial
hydrocephalus cause transtentorial descent without midline shift [1].
As descending transtentorial herniation progresses, there is further downward displacement of brain tissue, with disastrous
consequences. Damage is caused by local pressure from crowding of tissue within the incisura, which can lead to compromise of the
third cranial nerve, posterior cerebral artery, and midbrain, and there are also traction forces wreaking havoc. The lower brainstem is
less mobile because of the upper cervical dentate ligaments. The longitudinal compression of the upper brain stem against the unyielding
medulla leads to buckling of the brainstem and further compression of the midbrain tegmentum [22]. Downward displacement of the
brainstem also produces traction on the oculomotor nerve, causing third nerve palsy. Stretching and shearing of the perforating
branches of the basilar artery occur, resulting in ischemia and hemorrhage within the brainstem, called Duret's hemorrhage [23,24].
This occurrence is a late finding and portends a poor prognosis, usually death [22,25]. Hydrocephalus develops because of distortion and
obstruction of the cerebral aqueduct, further increasing the volume and pressure of supratentorial contents. Stovring pointed out that
preferential dilatation of the contralateral temporal horn tends to occur, because it is relatively shielded within the middle cranial fossa
from compression by the supratentorial mass [26]. There also is a propensity for dilatation of the contralateral occipital horn because of
relative shielding by the rigid posterior falx cerebrei. For the same reason, preferential dilatation of the contralateral temporal horn and
occipital horn may also occur with subfalcine herniation, although the cause of the hydrocephalus is the result of obstruction of the
foramen of Monro, rather than the aqueduct. Further descent can result in tonsillar herniation, with compression and distortion of the
medulla oblongata causing cardiorespiratory compromise. It has been well established clinically that patients who decompensate from
descending transtentorial herniation do so in an orderly rostral to caudal fashion of diencephalic and brainstem dysfunction [27]. The
clinical consequences of progressive central herniation are oculomotor paresis, progressive alteration of consciousness, decerebrate
rigidity, coma, and death.
Figure 13. Duret's hemorrhage. Axial CT scan of the head in a patient who had a large traumatic acute subdural hematoma (not shown)
and unilateral descending transtentorial herniation reveals a hemorrhage (arrowhead) within the dorsal brainstem consistent with a
Duret's hemorrhage.
Figure 14. Postmortem specimens showing hemorrhage (arrowhead) within the dorsal brainstem consistent with a Duret's hemorrhage.
The so-called Duret hemorrhages seen here in the pons are secondary to downward compression that leads to stretching, ischemia and
rupture of perforating arterioles and brain stem hemorrhage
Figure 15. A, These are sections of pons and cerebellum, showing severe Duret hemorrhages of the pons. The largest areas of
hemorrhage are marked by arrows, but the grey discoloration in the midline indicates damage there as well. In less severe cases, the
hemorrhages can be small, midline and linear. B, This is a mid-sagittal section of brain demonstrating the kinking of the brainstem due
to herniation, as well as the Duret hemorrhages of the midbrain and pons.
Effacement of the cisternal spaces, caudal displacement of the
basilar artery and pineal gland, deformity and displacement of the
midbrain, hydrocephalus, and infarction of the posterior cerebral
artery have all been described on CT as findings associated with
descending transtentorial herniation [17,28-30]. Most of these
findings are indirect, secondary, and late manifestations of descending transtentorial herniation. Effacement of the perimesencephalic
cisterns, though qualitative, is probably the most useful and consistent finding on CT. With its better soft tissue definition and
multiplanar imaging, MR provides superior anatomical detail of the tentorial incisura and adjacent structures. MRI findings of
descending transtentorial herniation include downward descent of the brainstem, effacement of the basal cisterns, flattening of the pons
against the clivus, and inferoposterior displacement of the quadrigeminal plate. As herniation progresses, deformity and buckling of the
brainstem occur. Hydrocephalus develops because of aqueductal obstruction.
Effacement of the cisternal spaces, caudal displacement of the basilar artery and
pineal gland, deformity and displacement of the midbrain, hydrocephalus, and
infarction of the posterior cerebral artery have all been described on CT as findings
associated with descending transtentorial herniation
Numerous authors have attempted to quantitate the degree of downward shift on MR images [19,31,32]. Ropper et al measured
horizontal and vertical components of brain displacement on coronal MR images in 10 patients with supratentorial masses [33].
Feldman et al compared vertical brainstem position on 50 images from normal patients and 21 images from 15 patients with large
supratentorial masses [31]. The methods of both Ropper and Feldman are cumbersome to employ in the clinical setting, and neither
study demonstrated significant correlation between measured vertical descent and neurologic signs. Reich et al measured the
relationship of the iter (proximal opening of the aqueduct of Sylvius) to the incisural line on mid-sagittal MR images [ 1 9]. The incisural
line was defined as a straight line from the anterior tuberculum sellae-to the inferior point of the confluent of the straight sinus, the vein
of Galen, and the inferior sagittal sinus. In 123 normal patients, the iter was 0.2 ñ .8 mm below the incisural line. Displacement of the
iter by more than two standard deviations (1.8 mm) below the incisural line was considered as MRI criterion for descending
transtentorial herniation. Eighteen patients with supratentorial masses demonstrated downward displacement of the iter ranging from
2.0 mm to I 1.0 mm, which correlated well with clinical signs of acute brain herniation, but less so with chronic cases [19]; however, in
clinical practice, qualitative assessment of downward shift on MRI scans is probably more widely applied, though measurement of
displacement of the iter relative to the incisural line can be useful.
Figure 16. Descending transtentorial herniation. Axial CT scan of the head demonstrates obliteration of the basal cisterns (arrows) in a
patient who sustained massive head trauma. There is downward displacement of the diencephalon and medial temporal lobes through
tentorial incisura, resulting in effacement of the perimesencephalic cisterns and compression and displacement of the brainstem.
Ascending transtentorial herniation
Just as a supratentorial masses may cause descent of brain tissue through the hiatus, an infratentorial mass may cause brain tissue to
ascend through the hiatus [30,34,35]. Ascending transtentorial herniation has been most frequently reported in association with a
cerebellar mass or a hydrocephalic ("trapped") fourth ventricle. Cerebellopontine angle masses and intrinsic masses of the pons have
also been reported, albeit much less commonly [34,36,37]. The propensity for ascending tentorial herniation to occur is more likely when
the mass is near the incisura (ie, superior cerebellar vermis), when shunting of the lateral ventricle reduces hydrocephalus and pressure
above, and when the opening of the incisura is large [34]. MR and CT findings of ascending transtentorial herniation include effacement
of the superior cerebellar cistern, superior displacement of the superior vermis through the incisura, compression of the midbrain, and
forward displacement of the pons against the clivus [31,34]. Ascending tentorial herniation can compress the posterior cerebral artery or
superior cerebellar arteries against the tentorium, resulting in infarctions, or it can compress the aqueduct of Sylvius, resulting in
hydrocephalus. Obstruction of venous outflow by compression of the vein of Galen and basal vein of Rosenthal may occur and further
increase intracranial pressure [38,39].
Figure 17. Ascending transtentorial herniation. (A) Axial T I - weighted MR image and (B) sagittal enhanced T I -weighted MR image
demonstrate ascending transtentorial herniation in a patient with a cerebellar lung metastases. Note the upward displacement of the
superior cerebellar vermis (black arrows) through the incisura, compression of the fourth ventricle, and anterior displacement of the
pons (arrowhead) against the clivus.
Tonsillar (foramen magnum) herniation
Tonsillar herniation is defined as inferior displacement of the cerebellar tonsils through the foramen magnum into the cervical spinal
canal. This is most commonly caused by a posterior fossa mass, but may also be caused by a supratentorial mass that causes downward
transtentorial herniation [40]. In fact, tonsillar herniation occurs in association with descending transtentorial herniation anywhere
from 20 to 50% of the time [14,19,41,42]. The propensity of tonsillar herniation to follow descending tentorial herniation is related to the
size and shape of the incisura. If the incisura is small, the patient will be less likely to have tonsillar herniation.
Figure 18. Tonsillar (foramen magnum) herniation. B, Here a head injury has resulted in tonsillar herniation of the cerebellum. The
arrows outline the necrotic cerebellar tissue which is overlying the medulla. There is also subarachnoid hemorrhage on the left
cerebellar hemisphere.
When tonsillar herniation progresses, pressure necrosis may develop where the tonsil is squeezed against the unyielding foramen
magnum. Compression of the medulla oblongata by the displaced cerebellar tonsils may lead to loss of consciousness secondary to
involvement of the ascending reticular activating system. Further progression of tonsillar herniation may damage cardiac and
respiratory centers of the brainstem and even result in death. Additionally, occlusion of the posterior inferior cerebellar artery between
the displaced tonsils and foramen magnum may result in cerebellar infarction.
Obstruction of the outlet foramina of the fourth ventricle causes hydrocephalus, further increasing intracranial pressure within the
posterior fossa and worsening the herniation.
Figure 19. Tonsillar herniation. Sagittal enhanced T I -weighted MR image demonstrates a large enhancing cerebellar mass causing both
tonsillar herniation and ascending transtentorial herniation. Note the inferior displacement of the tonsils (arrow) below the foramen
magnum and the effacement of the surrounding CSF spaces. The brainstem is compressed and displaced against the clivus and there is
upward displacement of the superior cerebellar vermis (arrowhead) through the incisura.
There are large variations in the anatomy of the foramen magnum and the inferior cerebellum [2]. In a group of 200 normal patients,
Barkovich et al demonstrated that the position of the tonsils ranged from 8 mm above the foramen magnum to 5 mm below the foramen
magnum [43]. Also, Aboulez et al reported the average distance of the tonsillar tips from the foramen magnum was 2.9 ñ 3.4 mm above
the foramen magnum in 82 normal patients [44]. They concluded that extension of the tonsils below the foramen magnum is considered
normal up to 3 mm, borderline between 3 mm and 5 mm, and clearly pathological when it exceeds 5 mm. Perhaps more important than
strict quantitative criteria of tonsillar displacement are the morphologic appearance of the brainstem and the surrounding CSF spaces.
When the tonsils extend below the foramen magnum, anterior displacement of the lower brain stem and loss of CSF space surrounding
the brainstem are important in distinguishing tonsillar herniation from normal variations [45].
Tonsillar herniation can be difficult to assess on axial CT because of beam hardening artifacts at the skull base and partial volume
average effects. MR imaging is the study of choice and sagittal images best delineate the relationship of the tonsils to the foramen
magnum. The foramen magnum can be identified on sagittal MR images by drawing a line from the inferior tip of the clivus (basin) to
the posterior lip of the foramen magnum (opisthion). Identification of the tonsils below the foramen magnum, anterior brainstem
displacement, and loss of CSF surrounding the brainstem indicate tonsillar herniation [46]. Of course, chronic tonsillar herniation, such
as occurs with Chiari malformations, must be distinguished from acquired tonsillar herniation. Fortunately, the clinical history and
imaging are characteristic and rarely cause diagnostic difficulty. The exception may be the presence of a posterior fossa mass with a preexisting Chiari I malformation.
Transphenoidal (transalar) herniation
Transphenoidal herniation is less well known, but occurs when brain tissue is displaced across the superior sphenoid alae, which
incompletely separate the anterior and middle cranial fossae [2]. Areas of necrosis and hemorrhage may develop where the brain is
displaced against the bony sphenoid ridge. There are two types of transphenoidal herniation: descending and ascending. Descending
transphenoidal herniation occurs when anterior cranial fossa mass effect causes displacement of the posterior frontal lobe over the
sphenoid wing into the middle cranial fossa. Ascending transphenoidal herniation is produced by middle cranial fossa mass effect, which
causes displacement of the anterior temporal lobe over the sphenoid ridge into the anterior cranial fossa. The middle cerebral artery can
become compressed between the displaced brain and the sphenoid ridge, resulting in middle cerebral artery infarction [4] Although
vascular compromise may occur with transphenoidal herniation, it is rare. Moreover, the clinical features of this type of herniation are
poorly defined.
Figure 20. Transphenoidal herniation. Sagittal enhanced Tl- weighted MR image demonstrates a large ring enhancing mass (arrowhead)
in the right frontal lobe causing descending transphenoidal herniation (arrow)
External herniation
External herniations, also known as fungus cerebrei, are the rarest of acquired herniations [45]. They are most frequently caused by
post surgical and posttraumatic defects that allow swollen or displaced brain to pass through. This type of herniation may be beneficial
by relieving intracranial pressure and thereby preventing more devastating complications due to internal herniation; however, external
exposure of the brain can result in infectious complications, and many of these patients have a poor prognosis because of the severity of
their underlying illness. Both CT and MR imaging are effective at demonstrating these herniations. MR imaging, however, is clearly
superior at defining soft tissue, which can be critical in certain clinical scenarios. Distinguishing brain tissue from other tissues such as
granulation tissue, cholesteatoma, tumor, or other lesions involving defects of the skull is essential, and MR imaging accomplishes this
well [4,47]. MR imaging is also superior for evaluation of congenital encephaloceles, which are essentially congenital external hernias.
Figure 21. (A) Axial CT scan and (B) axial T I weighted MR image of the head demonstrate a large right frontal external hernia in a
patient who underwent a wide scalp excision, craniectomy, and free flap for an infiltrative squamous cell carcinoma. The flap became
infected and failed, and the patient developed encephalitis resulting in external herniation.
Intracranial hypotension
Intracranial hypotension is a cause of cerebral herniation that should be considered in patients who do not harbor an intracranial mass
or edema, or in patients in whom the degree of herniation is out of proportion to the degree of mass effect. Intracranial hypotension is
caused by a CSF leak, either iatrogenic or spontaneous. As previously stated, the intracranial cavity is essentially a closed system and the
volume is constant. These principles were described as early as the 1780s by Scottish anatomists Alexander Monro and George Kellie in
what is known as the Monro Kellie doctrine, which states that intracranial volume is constant and is represented by the summed
volumes of brain substance, CSF, and blood [3]. Since brain volume is constant, the volumes of CSF and blood fluctuate reciprocally.
This buffering capacity is very limited, but does explain the imaging findings in patients with intracranial hypotension. With a loss in
CSF volume, there is a greater increase in blood volume. This results in dural venous hyperemia and pachymeningeal venous
engorgement and edema, which can be identified on MR imaging as diffuse pachymeningeal enhancement. Furthermore, the decrease in
volume of the suspending CSF results in downward descent of the brain and can cause descending central transtentorial herniation and
tonsillar herniation. A blood patch or surgical repair of the dural defect is usually required.
Figure 22. Intracranial hypotension. (A) Coronal enhanced T1-weighted MR image demonstrates diffuse pachymeningeal enhancement
(arrows) in a patient with severe postural headaches. (B) Sagittal enhanced T1-weighted NM image reveals tonsillar herniation (arrow),
descending transtentorial herniation (note downward descent of the brainstem, loss of surrounding CSF spaces and flattening of the
pons against the clivus) and pachymeningeal enhancement (arrowheads). (C) Postmyelogram CT scan of the thoracic spine shows an
extradural accumulation of contrast (arrow) within die spinal canal consistent with a CSF leak. The extradural and intradural confluent
medium outlines the dura (arrowhead) at the T10 level. A blood patch performed at this level resulted in resolution of the patient's
symptoms.
SUMMARY
The consequences of cerebral herniation are compression of the brain, cranial nerves, and blood vessels that may result in serious
neurologic morbidity, coma, and even death. A thorough understanding of the various patterns of cerebral herniation is essential, and it
is important to remember that many of these patterns of herniation overlap. CT and MR imaging are effective at establishing the
diagnosis of cerebral herniation, which will guide important decisions regarding therapeutic options and prognosis.
References
[1] Plum F, Posner JB. The diagnosis of stupor and coma. 3rd edition. Philadelphia: F.A. Davis; 1980.
[2] McComb JG, Davis RL. Choroid plexus, cerebrospinal fluid, hydrocephalus, cerebral edema, and herniation phenomena. In: Davis
RL, Robertson DM, editors. Textbook of neuropathology. Baltimore: Williams & Wilkins; 1985. p. 164-71.
[3] Mokri B. The Monro-Kellie hypothesis, applications in CSF volume depletion. Neurology 2001;56:1746-8.
[4] Laine FJ, Sheden Al, Dunn MM, Ghatak NR. Acquired intracranial herniations: MR imaging findings. AJR 1995;165:967-73.
[5] Coburn MW, Rodriquez FJ. Cerebral herniations. Appl Radiol 1998;27:10-16.
[6] Gray H. Gray's anatomy. In: Warwick R, Williams PL. Philadelphia: Running Press; 1974. p. 512-23.
[7] Strong OS, Elwyn A. Strong and Elwyn's neuroanatomy. 5th edition. In: Truex RC, Carpenter MB, editors. Baltimore (MD): 1987.
[8] Hassler 0. Arterial pattern of human brainstem: normal appearance and deformation in expanding supratentorial conditions.
Neurology 1967;17:1-6.
[9] Sohn D, Levine S. Frontal lobe infarcts caused by brain herniation: compression of anterior cerebral artery branches. Arch Pathol
Labe Med 1967;84:509-12.
[10] Marshall LF, Toole BM, Bowers SA. The National Traumatic Coma Data Bank. Part 2: patients who talk and deteriorate:
implications for treatment. J Neurosurg 1983;59:285-8.
[11] Miller JD, Becker DP, Ward JD, et al. Significance of intracranial hypertension in severe head injury. J Neurosurg 1977;47:503-16.
[12] Ross DA, Walter OL, Ross AM, et al. Brain shift, level of consciousness and restoration of consciousness in patients with acute
intracranial hematoma. J Neurosurg 1989;71:498-502.
[13] Finney LA, Walker AE. Transtentorial herniation. Springfield (IL): Thomas; 1962.
[14] Meyer A. Herniation of the brain. Arch Neurol 1920;4: 387-400.
[15] Collier J. The false localizing signs of intracranial tumors. Brain 1904;27:490-508.
[16] Kemohan JW, Woltman HW. Incisura of the cuts due to contralateral brain tumor. Arch Neurol Psychiatry 1929;21:274-87.
[17] Sato M, Tanaka S, Kohwna A, Fujii C. Occipital lobe infarction caused by tentorial herniation. Neurosurgery 1986;18:300-5.
[18] Osborn AG. Diagnosing of descending transtentorial herniation by cranial computed tomography. Radiology 1976;123:93-6.
[19] Reich JB, Sierra J, Camp W, et al. Magnetic resonance imaging: measurements and clinical changes accompanying transtentorial
and foramen magnum brain herniation. Ann Neurol 1993;33:159-70.
[20] Stovring J. Descending tentorial herniation: findings on computed tomography. Neuroradiology 1977;14: 101-5.
[21] Johnson RT, Yates PO. Clinico-pathological aspects of pressure changes at the tentorium. Acta Radiol 1956b; 46:250-6.
[22] Howell DA. Longitudinal brain stem compression with buckling. Arch Neurol 1961;4:572-9.
[23] Fisher CM. Acute brainstem herniation: a revised concept. Semin Neurol 1984;4:417-21.
[24] Thompson RK, Scalman M. Brainstem hemorrhages: historical perspective. Neurosurgery 1988;22:623-8.
[25] Scheinker IM. Transtentorial herniation of the brain- stem; a characteristic clinicopathologic syndrome: pathogenesis of
hemorrhages in the brainstem. Arch Neurol Psychiatr 1945;53:289-98.
[26] Stovring J. Contralateral temporal horn widening in unilateral supratentorial mass lesions: a diagnostic sign indicating tentorial
herniation. J Comput Assist Tomogr 1977;1:319-23.
[27] McNealy DE, Plum F. Brainstem dysfunction with supratentorial mass lesions. Arch Neurol 1962;7:10-32.
[28] Hahn F, Gurney J. CT signs of central descending transtentorial herniation. AJNR 1985;6:844-5.
[29] Hahn F, Rim K, Schapiro RL. The normal range and position of the pineal gland on computed tomography. Radiology
1976;119:599-600.
[30] Speigelman R, Hadani M, Ram Z, et al. Upward transtentorial herniation: a complication of postoperative edema at the
cervicomedullary junction. Neurosurg 1989;24:284-8.
[31] Feldman E, Gandy SE, Becker R, et al. MRI demonstrates descending transtentorial herniation. Neurology 1988;38:697-701.
(32] Ropper AH. A preliminary MRI study of the geometry of brain displacement and level of consciousness with acute intracranial
masses. Neurology 1989;39:622-7.
[33] Ropper AH. Lateral displacement of the brain and level of consciousness in patients with an acute hemispheral mass. N Engl J Med
1986;314:953-8.
[34] Cuneo RA, Caronna JJ, Pitts L, et al. Upward transtentorial herniation. Seven cases and a literature review. Arch Neurol
1979;36:618-23.
[35] Ecker A. Upward transtentorial herniation of the brain- stem and cerebellum due to tumor of the posterior fossa: with a special
note on tumors of acoustic nerve. J Neurosurg 1948;5:51-61.
[36] Binkow SM, Smimov NA, Onischenko GT, translator. Lindsley DB, editor. Brain displacements and deformations. New York:
Plenum Press; 1971.
[37] Dinsdale HB. Spontaneous hemorrhage in the posterior fossa. Arch Neurol 1964;10:98-115.
[38] Azainbuja N, Lindren E, Sjorgen SE. Tentorial herniations. 1,11,III. Acta Radiol 1956;46:215-41.
[39] Sunderland S. The tentorial notch and complications produced by herniations of the brain through that aperture. Br J Surg
1958;455:422-38.
[40] Cushing H. Some experimental and clinical observations concerning states of increased intracranial tension. Am J Med Sci
1902;124:375-400.
[41] Ryder JW, Kleinschmidt-Demasters BK, Keller TS. Sudden deterioration and death in patients with benign tumor$ of the third
ventricle area. J Neurosurg 1986; 64:216-23.
[42] Schwarz GA, Rosner AA. Displacement and herniation of the hippocampal gyros through the incisura tentorii. Arch of Neurol
Psychiatry 1941;46:297-321.
[43] Barkovich AJ, Wippold FJ, Sherman JL, Citrin CM. Significance of cerebellar tonsil position on MRI. Am J Neuroradiol
1986;6:795-9.
[44] Aboulezz AO, Sartor K, Geyer CA, et al. Position of cerebellar tonsils in the normal population and in patients with Chiari
Malformation: a quantitative approach with MR imaging. J Comput Assist Tomogr 1985;9: 1033-6.
[451 Andrews BT, Chiles BW, Olsen WL, et al. The effect of intracerebral hematoma location on the risk of brainstem compression and
on clinical outcome. J Neurosurg 1988;69:518-22.
[46] Ishikawa M, Kikuch H, Fujisawa I, Yonekawa Y. Tonsillar herniation on magnetic resonance imaging. Neurosurgery 1988;22:7781.
[47] Kaseff LG, Seidenwurin DJ, Nieberding pH, et al. Magnetic resonance imaging of brain herniation into the middle ear. Am J Otol
1992;13:74-7.
Addendum
A new version of topic of the month publication is uploaded in my web site every month (it remains for a month and is changed with the monthly update of the neurology bulletin at:.http://neurology.yassermetwally.com)
To download the current version of topic of the month publication follow the link "http://neurology.yassermetwally.com/topic.zip"
You can also download the current version of topic of the month publication from within the publication or go to my web site at:
"http://yassermetwally.com" to download it.
At the end of each year, all the publications are compiled on a single CD-ROM, please author to know more details.
Screen resolution is better set at 1024*768 pixel screen area for optimum display
For an archive of the previously published topics in downloadable PDF format go to http://yassermetwally.net, then under pages in the
right panel, scroll down and click on the text entry "topic of the month"
In order to view a list of the previously published topics in downloadable PDF format, follow the link:
http://wordpress.com/tag/neurological-topic-of-the-month/
The author: Professor Yasser Metwally, professor of neurology, Ain Shams university, Cairo, Egypt
www.yassermetwally.com