Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
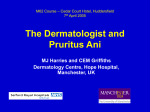
1130-0108/2012/104/1/41-42 REVISTA ESPAÑOLA DE ENFERMEDADES DIGESTIVAS Copyright © 2012 ARÁN EDICIONES, S. L. REV ESP ENFERM DIG (Madrid) Vol. 104, N.° 1, pp. 41-42, 2012 Letters to the Editor Perianal cutaneous metastases from colorectal adenocarcinoma Key words: Cutaneous metastases. Exfoliated cancer cells. Colorectal adenocarcinoma. remains asymptomatic 16 years after its complete removal with cutaneous adenocarcinoma metastasis diagnosis. Case 3. An 83 year-old male underwent surgery for rectal villous tumor using a Lone-Star retractor, with diagnosis of an invasive adenocarcinoma. Then, a rectal resection without anastomosis was done. A year later, a perianal tumor developed and it was resected, with biopsy of adenocarcinoma (Fig. 1 C). The patient died two years later of a heart attack, with no evidence of tumor relapse. Discussion Dear Editor, The appearance of cutaneous metastases in the perianal region from adenocarcinoma of colon and rectum is an uncommon feature, and its presence usually implies a worse prognosis as a disseminated disease. Occasionally, they present with no evidence of visceral involvement, therefore their diagnosis and treatment can significantly modify the course of the disease. We present 3 patients with perianal implants of colorectal cancer treated surgically with good long-term results, emphasizing that in one of them the implant was discovered before the primary tumor. Case reports Case 1. A 54-year-old male presented a hemorrhoidal thrombosis resistant to anti-inflammatory treatment that was biopsied with the diagnosis of adenocarcinoma. Preoperative tests showed a sigmoid colon neoplasm with lymphonodes and a small mass in low rectum-anal canal infiltrating sphincters and puborectalis muscle (T4 N1 M1) (Fig. 1 A and B). Abdominoperineal amputation was done including the sigmoid tumor and their anal canal implant. Two years after surgery, the patient is malignancy free. Case 2. A 55-year-old male who underwent surgery for a welldifferentiated low rectal carcinoma with a coloanal hand-sewn anastomosis showed a perianal tumor after two years. The patient The appearance of cutaneous metastasis from colorectal cancer is an uncommon fact (4%) (1). After tumor diagnosis, the average interval of the development of implants is 4.9 years, although they may appear at any time (2). The most common ways of cutaneous tumor dissemination are hematic or lymphatic spread. The hypothetical potential of implant exfoliated tumoral cells, was first time published by Charles Ryall (3). Subsequently has been demonstrated that exfoliated tumor cells are viable (4), requiring a mucosal damage for their implantation and growing (5). In the first patient, some mucosal fraction of his hemorrhoidal thrombosis was the base of cells implant from a hidden sigmoid neoplasia. It is the first case described in medical publications. In the second case, after hand-sewn coloanal anastomosis, the implant was most likely done during surgery (6). The third patient’s metastasis appeared probably in the small wounds made by the Lone-Star retractor used during the tumor resection, like has been previously published (7). Implants of malignant cells have been reported on benign anal lesions during colorectal cancer surgery (2), colonoscopy with biopsy (8), at the site of laparoscopic ports (1), or even in the injured perianal area during the introduction of an EEA stapling device to carry out a mechanical anastomosis (9). The appearance of perianal metastasis usually implies a worse prognosis, because it is a disseminated disease with 18-20 months survival rate (7). However, none of our patients presented recurrence. 42 LETTERS TO THE EDITOR A B REV ESP ENFERM DIG (Madrid) C Fig. 1. Perianal implant on a hemorrhoidal thrombosis. A. mucocutaneous erosion (arrows). B. Endoanal ultrasound scan showing a mixed echogenicity lesion (arrows) infiltrating sphincters at the medium-low anal canal. C. Perianal implant exposed with a Lone-Star retractor prior its resection. There are several measures to control tumor dissemination during surgery, although their real effect has not been well proved, but irrigation of rectal stump with tumoricidal agents before the anastomosis (10) is recommended. The perianal cutaneous metastases treatment ranges from limited local resection (1,7,9) to a more aggressive approach (2). In conclusion, we recommend using preventive measures for cutaneous implants in colorectal surgery, to rule out an intestinal origin of a perianal tumor with diagnosis of, and a complete exeresis of perianal implants without evidence of distant disease. Miriam Cantos-Pallarés, Juan García-Armengol, Claudia Mulas-Fernández, Cristina Sancho-Moya, Isabel Fabra-Cabrera, Marcos Bruna-Esteban and José Vicente Roig-Vila Unit of Coloproctology. Department of General and Digestive Surgery. Consorcio Hospital General Universitario de Valencia. Valencia, Spain References 1. Placer C, Elósegui JL, Irureta I, Mujika JA, Goena I, Enríquez Navascués JM. Metástasis cutánea perineal de adenocarcinoma tras cirugía de cáncer colorrectal. Cir Esp 2007;82:41-3. 2. Kouraklis G, Glinavou A, Kouvaraki M, Raftopoulos J, Karatzas G. Anal lesion resulting from implantation of viable tumour cells in a preexisting anal fistula. A case report. Acta Chir Belg 2002;102:212-3. 3. Ryall C. Cancer infection and cancer recurrence. Lancet 1907;II:13116. 4. Skipper D, Cooper AJ, Marston JE, Taylor I. Exfoliated cells and in vitro growth in colorectal cancer. Br Surg 1987;74:1049-52. 5. Hubens G, Lafullarde T, Van Marck E, Vermeulen P, Hubens A. Implantation of colon cancer cells on intact and damaged colon mucosa and serosa: an experimental study in the rat. Acta Chir Belg 1994;94:25862. 6. García-Armengol J, Roig JV, Alós R, Solana A. Metástasis cutánea perianal de adenocarcinoma rectal. Rev Esp Enferm Dig 1995;87:342-3. 7. Tranchart H, Benoist S, Penna C, Julie C, Rougier P, Nordlinger B. Cutaneous perianal recurrence on the site of Lone Star Retractor after J-pouch coloanal anastomosis for rectal cancer: report of two cases. Dis Colon Rectum 2008;51:1850-2. 8. Basha G, Ectors N, Penninckx F, Filez L, Geboes K. Tumor cell implantation with biopsy in a patient with rectal cancer: a case report. Dis Colon Rectum 1997;40:1508-10. 9. De Friend DJ, Kramer E, Prescott R, Corson J, Gallagher P. Cutaneous perianal recurrence of cancer after anterior resection using the EEA stapling device. Ann R Coll Surg Engl 1992;74:142-3. 10. Jenner DC, De Boer WB, Clarke G, Lewitt MD. Rectal washout eliminates exfoliated malignant cells. Dis Colon Rectum 1998;41:1432-4. REV ESP ENFERM DIG 2012; 104 (1): 41-42