Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
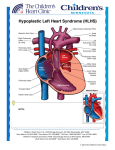
ANESTHETIC MANAGEMENT OF A PATIENT WITH PALLIATED HYPOPLASIC LEFT HEART SYNDROME FOR OPEN NISSEN FUNDOPLICATION Moderator: Andrea C. Pérez-Pradilla M.D Institution: National Institute of Pediatrics, Mexico City, Mexico. Goals: 1. Understand the single ventricle physiology of a patient with Hypoplasic left Heart Syndrome who underwent a Norwood procedure with a Sano Modification. 2. Discuss preoperative evaluation, preparation and anesthetic implications associated with a single ventricle physiology in order to maintain the balance between Qp:Qs 3. Recognize the importance of preserving central veins and arteries for future Access and intervention. 4. Identify the main causes of hypoxemia and how to correct them. 5. Acknowledge the importance of adequate analgesia in the postoperative setting. Case History A 57 days old female patient with Palliated Hypoplasic Left Heart Syndrome, who has gastroesophageal reflux and associated lung disease, comes to your institution and after evaluation from a multidisciplinary group is scheduled for an Open Nissen Fundoplication and gastrostomy tube placement. At 18 days of age, the patient underwent a Norwood Procedure with Sano modification, had a prolonged orotracheal intubation and mechanical ventilation (25 days) and also had two episodes of cardiac arrest associated with pneumothorax after withdrawing thoracostomy tubes. The patient is currently treated with Furosemide, Espironolactone and Captopril and in the previous month required antimicrobial treatment with Meropenem and Vancomicine because of Ventilator Associated Pneumonia. Questions ¿What is Left Hypoplasic Left Heart Syndrome?, ¿what is a Norwood procedure with Sano modification?, ¿what is the usual treatment for this disease?, ¿what is Qp:Qs?, ¿What is the importance of this surgical procedure for the prognosis of the patient?. Case History (continued) During the Preanesthetic Assessment you find an alert, well hydrated patient, without signs of respiratory distress, 3300 g of weight and 56 cms of height. Her non invasive arterial blood pressure, heart and respiratory rate as well as axilary temperature were normal, her SpO2 was 84% with 0,5 L of O2 through a nasal cannula. You find a systolic murmur grade 3/6 with greater intensity in the aortic and pulmonic areas and simmetric normal breath sounds and a subtle hepatomegaly (1 cm below the costal margin). There were no other relevant signs in the physical examination. At the time of the assessment she has only a peripheral 24G IV catheter for the administration of mainteinance fluids. Preoperative testing showed a normal CBC (Complete cell blood count) as well as normal PT, PTT and INR. Renal function tests and electrolytes were normal. An EKG showed no arrhythmias and an echocardiographic evaluation showed adequate single ventricle function and permeability of the Sano conduit. The chest X ray showed no abnormal infiltrates. Questions ¿what are the preanesthetic considerations for this patient to choose the perfect timing for surgery?, ¿Do you consider it necessary to have a consultation with other healthcare members (cardiologists, ICU)?, If so, who would we involve and what preoperative studies would you order?. ¿What risks and complications would you expect and explain to the patient`s parents?. ¿Do you require packed red cells or other components for transfusion? ¿What is your anesthetic plan? ¿is there any consideration or contraindication for the use of regional anesthesia techniques?, ¿what is your plan for IV access?, ¿Do we need invasive monitoring?, if so, what would you use?, ¿how would you maintain the balance between Qp:Qs?, ¿what would you use for anesthesia?, ¿what would you use to ensure adequate analgesia?, ¿Would you consider extubation after the procedure?, ¿Where would you take the patient after surgery for postoperative care? Discussion The Hypoplasic Left Heart Syndrome (HLHS) describes a heterogeneous group of cardiac malformations consisting of various degrees of underdevelopment of the left heart and the aorta, resulting in significant obstruction to flow of blood into the systemic circulation and compromising coronary perfusion and therefore adequate ventricular function. It is the most common congenital heart defect, comprising 7-‐9% of all anomalies diagnosed within the first year of life. The incidence is 0,16/1000 births and is estimated that it causes 25% of deaths during the first week of life. The prognosis of this disease without surgical intervention is dismal. There are three basic strategies for the neonatal management of HLHS: surgical palliation with staged interventions (Norwood procedure, Bidirectional Glenn or Hemi-‐Fontan procedure and the Fontan procedure), Hybrid palliation with surgical bilateral pulmonary artery banding and transcatheter ductal stenting, and orthotopic transplantation. The Norwood procedure is the first step of the staged intervention; it involves constructing a neoaorta from the proximal pulmonary artery and the hypoplasic ascending aorta using a patch of homograft material. This homograft connects the pulmonary valve and proximal main pulmonary trunk to the aorta so that the single right ventricle supplies unobstructed blood flow to both the body and coronary arteries. Pulmonary blood flow is achieved either through a modified Blalock-‐Taussig shunt or a Right ventricle (RV) to Pulmonary artery (PA) conduit (Sano modification). Improvements in the management of these patients are resulting in prolonged survival, allowing them to develop comorbid conditions such as malnutrition and gastroesophageal reflux disease. These conditions may require surgical interventions in patients with Stage I physiology. There are few case reports of anesthetic management of patients with HLHS for Nissen Fundoplication. Congenital Heart Disease adds a significant risk of mortality in children requiring noncardiac surgery, especially in patients with single ventricle physiology who cannot have a “definite” surgical repair. When possible, elective, noncardiac surgery should be scheduled after superior cavopulmonary shunt. Preoperative evaluation should focus on the evaluation of the balance between Qp:Qs, presence of cardiac failure and end-‐organ injury from low systemic perfusion. It includes a thorough history, cardiovascular, respiratory (recent infection, chronic disease), medication (diuretics, ACE inhibitors, Acetylsalicylic acid), functional status and a complete physical examination with vital signs. It’s important to evaluate a recent electrocardiogram and an echocardiogram to assess ventricular function, AV valve function, RV-‐PA conduit permeability and to understand patient´s physiology; if available, catheterization reports must be reviewed. Chest radiograph and blood work (CBC, electrolytes, urea, creatinine, coagulation profile and liver function tests) should be added and a cardiology consultation is in order. Preoperative fasting periods should be kept to a minimum because the single ventricle is preload dependent and intolerant to sudden increases in afterload. Anesthetic induction method can be chosen depending on the status of the patient, however, intravenous induction is advisable. Bacterial endocarditis prophylaxis is necessary for all procedures. These patients have a high risk of developing subendocardial ischemia and ventricular fibrillation due to increases in heart rate. This demands the maintenance of normovolemia and the availability of inotropic and cardiac resuscitation drugs. Anesthetic maintenance is usually achieved with volatile anesthetics and opioids. There are no specific recommendations or contraindications for the use of regional anesthesia techniques. The arterial oxygen saturation usually increases once the patient is anesthetized due to reduced peripheral O2 extraction and improved cardiac output (reduced afterload). The primary goal in the management of patients with single ventricle physiology is optimizing systemic oxygen delivery and perfusion pressure. This is achieved by balancing systemic and pulmonary circulations (Qp:Qs). It´s important to avoid hyperventilation and hyperoxia because it would reduce Pulmonary Vascular Resistance (PVR) and cause pulmonary “overcirculation”; Hypoxia and Hypercarbia will elevate PVR and cause pulmonary “undercirculation”. SaO2 must be kept between 75-‐80% and SaO2-‐SmvO2 between 25-‐30%. Elevation of Systemic Vascular Resistance (SVR) could generate lactic acidosis and low cardiac output (High afterload). Hypothermia should also be avoided because it could elevate SVR and also elevate VO2. The requirement for invasive monitoring is defined by the patient´s clinical condition and programmed procedure. These patients will need various cardiac surgical procedures involving the superior and inferior vena cava in order to complete the stages of palliation; therefore, preservation of central veins for future access in these patients is of paramount importance. The use of an arterial line will provide valuable information during noncardiac surgery as well as echocardiography if available. Air embolism should be prevented at all times. There are no specific recommendations about the ideal method for analgesia in these patients; however, inadequate management of pain would generate elevation of SVR and PVR. Therefore, adequate evaluation and management of postoperative pain should be carefully planned. In summary, patients with palliated HLHS have anesthetic considerations that must be followed in order to reduce perioperative morbidity and mortality in this high-‐risk population. The improvement in life expectancy will make more likely for these patients to come to our Institutions for perioperative care. References 1. Feinstein J, Benson W, Dubin A, Cohen M, Maxey D, Mahle W et al. Hypoplastic Left Heart Syndrome. JACC 2012; 59 (1), Suppl S:S1-‐42. 2. Yuki K, Casta A, Uezono S. Anesthetic management of noncardiac surgery for patients with single ventricle physiology. J Anesth 2011; 25:247–256. 3. Mariano E, Boltz G, Albanese C. Anesthetic Management of Infants with Palliated Hypoplastic Left Heart Syndrome Undergoing Laparoscopic Nissen Fundoplication. Anesth Analg 2005;100:1631–3. 4. Schwartz S, Dent C, Musa N, Nelson D. Single-‐ventricle physiology. Crit Care Clin 2003;19: 393–411. 5. Walker S, Stuth E. Single-‐Ventricle Physiology: Perioperative Implications. Seminars in Pediatric Surgery 2004; 13(3):188-‐202. 6. Leyvi G, Wasnick J. Single-‐Ventricle Patient: Pathophysiology and Anesthetic Management. J Cardiothorac Vasc Anesth. 2010 Feb;24 (1):121-‐30.