Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
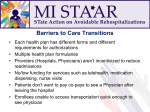
MOUNT CARMEL WEST: DISCHARGE MEDICATION RECONCILIATION AND COUNSELING INITIATIVE Issue: Improving the patient experience and safety by reducing medication errors, increasing patient satisfaction, and reducing hospital readmissions through a discharge medication reconciliation and counseling initiative is the goal at Mount Carmel West Hospital. Through the collaboration of pharmacists, nursing staff, and case managers Mount Carmel West was able to develop a process to ensure appropriate medication reconciliation and patient counseling of medications at discharge. Project Description: Pharmacists worked with the team on a medical intermediate care unit to establish which patients will be discharged, establish eligibility, and prioritize counseling. Pharmacists start the review of a patient by reading the physicians discharge summary to ensure the plan for discharge medications was accurately reflected in the discharge medication reconciliation. The pharmacist also uses their disease state management skills to assess whether the patients are discharged on the most appropriate and affordable medications, and help facilitate proper access to medications through our Medication Assistance Program or retail four dollar/free prescription programs. Patient education materials are printed for all new medications, highlighting important facts, and a simplified purpose is added to all medication listed, to provide better understanding for the use of the medications. Three to seven days post discharge the pharmacist calls the patient to follow-up on his/her medications. The intent of the call is to ensure that the patient has started their new medications, answer any questions pertaining to medications, and see if they are experiencing any possible side effects. Results: The initiation of a discharge medication reconciliation and patient counseling service has greatly impacted the patient safety and quality of care on one of our medical intermediate care units. Thirty-three percent of all patients seen by our pharmacists have had an intervention made to improve their discharge medications and prevent medication errors. During the initial twenty weeks of this initiative the pharmacists were able to review, counsel, and follow up with 431 patients. 144 patients required a pharmacist intervention and 213 interventions were made on these patients. Over 75 of those interventions had the potential for “serious capacity for harm” or were potentially “life threatening”. Medication errors with serious harm cost on average $2,200. Over the twenty week timeframe 75 interventions were made to avoid “serious capacity for harm” errors resulting in $165,000 in cost avoidance (75 errors x $2,200/serious error = $165,000). After adding in the cost of 1.5 FTE pharmacist for the twenty week timeframe ($54,000) the net savings totaled $111,000 for twenty weeks on one medical intermediate care unit. Patient satisfaction has also shown a positive trend with patients “strongly agreeing” that when they left the hospital they clearly understood the purpose for taking each of their medications. Data continues to be collected to evaluate the effectiveness of this initiative on readmission rates. Lessons Learned: Three main lessons were learned during this initiative: 1. Putting medication experts, pharmacists, at the bedside to counsel patients on medications increased patient satisfaction and reduced the nursing burden at discharge. 2. Review of the discharge medication reconciliation resulted in ~35% fewer potential medication errors. 3. Collaboration between the multidisciplinary team at discharge increases patient safety and satisfaction. Submitters: Virginia Ruef, PharmD Mount Carmel West Hospital – Pharmacy Department [email protected] Leslie Roth, RN, BSN Mount Carmel West Hospital- Medical Intermediate Care Unit [email protected] Karla Miklos, CRN,BSN Mount Carmel West Hospital- Medical Intermediate Care Unit [email protected]