Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
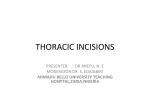
1306-14.qxd 11/23/03 9:22 PM Page 565 Cardiol Young 2003; 13: 565–567 © Greenwich Medical Media Ltd. ISSN 1047-9511 Brief Report Midaxillary lateral thoracotomy for closure of atrial septal defects in pre-pubescent female children: reappraisal of an “old technique” Christian Schreiber, Sabine Bleiziffer, Rüdiger Lange Clinic of Cardiovascular Surgery, German Heart Center Munich at the Technical University, Munich, Germany Abstract Our long-term follow-up has revealed that symmetrical development of the breasts is significantly impaired in pre-pubescent female patients subsequent to an anterolateral thoracotomy. Although standard posterolateral and anterolateral right-sided thoracotomies are used for correction of “simple” cardiac lesions such as patency of the arterial duct, coarctation of the aorta, or atrial septal defect, the required partial transection of large muscle groups, and injury to the developing tissues of the breast, may contribute to an unfavourable cosmetic outcome. Over the years, many surgeons, mostly specialising in thoracic procedures, have advocated mini- or axillary thoracotomies. In an attempt to improve surgical and cosmetic outcome, we have now adopted such a muscle-sparing approach, using a small horizontal midaxillary incision. We have now successfully employed the technique to close atrial septal defects in the oval fossa in 17 pre-pubescent females. Keywords: Minimal invasive cardiac surgery; posterolateral thoracotomy; anterolateral thoracotomy S TANDARD POSTEROLATERAL AND ANTEROLATERAL right-sided thoracotomies have now gained general acceptance as the standard surgical approaches in correction of “simple” cardiac lesions such as persistent patency of the arterial duct, cooarctation of the aorta, and atrial septal defect in the oval fossa. These approaches are considered minimally invasive, since they avoid median sternotomy, and help to improve the cosmetic result. The division or incision of the latissimus dorsi, serratus anterior, or pectoralis muscles, nonetheless, produces significant trauma to the chest, and may cause substantial perioperative morbidity and long-term disability.1–3 Because of this, thoracic surgeons have described the use of limited thoracotomies.4–6 More recently, Yang et al.7 have described their results using such a technique in combination with cardiopulmonary bypass. With this in mind, we describe here our own modification of the technique used in patients undergoing an anterolateral thoracotomy whilst below the Correspondence to: Christian Schreiber MD, German Heart Center Munich, Clinic of Cardiovascular Surgery at the Technical University, Lazarettstrasse 36, 80636 Munich, Germany. Tel: 0049 (0)89 12184111; Fax: 0049 (0)89 12184113; E-mail: [email protected] Accepted for publication 18 August 2003 age of 12 years at the time of operation.8 So as to avoid impaired development of the breasts, we have successfully employed the modified midaxillary technique in 17 patients undergoing closure of an atrial septal defect in the oval fossa between the ages of 4 and 12 years. Technique The patient is placed in an anterior oblique position at an angle of 45°, and the arm is suspended at a right angle. The skin incision is performed near the midaxillary line. It begins at the height of the mammary areola, and passes posteriorly towards the tip of the scapula, ranging in length from 5 to 6.5 cm. Although the latissimus dorsi muscle inserts on the posterior aspect of the iliac crest, in the lateral position the anterior margin is usually found on the line between the posterior axillary fold and the anterior-superior iliac spine. The subcutaneous attachments of the latissimus dorsi muscle are mobilized with electrocautery by dissecting just superficial to the fascia. The entire anterior border of the muscle is thus freed. The muscle can now be retracted posteriorly, exposing the serratus anterior muscle. This muscle is dissected 1306-14.qxd 11/23/03 566 9:22 PM Page 566 Cardiology in the Young December 2003 sutures are placed, and the muscles are allowed to return to their normal position. Single sutures can be placed on the posterior border of the serratus muscle, and another on the anterior border of the latissimus muscle, thus anchoring them to the surrounding fascia. Figure 1. The exposure of the lateral aspect of the right side of the heart achieved through the midaxillary thoracotomy. by dividing the fascia along its posterior border up to, and just above, the tip of the scapula, and down to the lowest attachment on the anterior aspect of the sixth rib. The muscle is retracted forward. The thorax is opened in the bed of the fourth rib. The heart is exposed adequately by opening the pericardium, and placing suitable stay sutures (Fig. 1). Tapes are passed around the caval veins. Two standard purse-string sutures are placed on the ascending aorta, and direct cannulation is performed. We have used “Medtronic” DLP® cannulas. After placing standard purse-string sutures at the junctions of the caval veins with the right atrium, we perform bicaval cannulation using straight cannulas, currently employing wire-reinforced cannulas from Stöckert®. The use of angled cannulas may also be considered. We have not used femoral or iliac cannulation in any patient in our series. Cardiopulmonary bypass is instituted. The caval venous tapes are snared, the right atrium is opened under normothermia, and fibrillation is induced electrically. We perform a vertical incision in the mid portion of the atrium, believing this to facilitate subsequent closure after the modified thoracotomy in contrast to the primary standard oblique atrial incision. Two sump suckers, of which one is placed in the coronary sinus, allow clear exposure of the right atrial cavity. The intraatrial defect is either closed with direct suture or patch material. The pericardial stay-sutures are then removed before gradually inflating the lungs for de-airing. With a needle and a syringe, blood is withdrawn from the pulmonary veins, or directly from the left atrium and the ascending aorta. The operating table is then rotated, keeping down the head of the patient, and the heart is defibrillated. After a short period of reperfusion, the patient is weaned from bypass. To close, the retractors are removed, pericostal Discussion Considerable discussion continues, not only between thoracic surgeons but also cardiac surgeons, regarding the merits of different thoracotomies. It is accepted that standard posterolateral or anterolateral thoracotomy incisions provide good exposure of the intrathoracic structures. In cardiac surgery, these lateral thoracotomies are used in children9,10 as an alternative access to anterior approaches such as full sternotomy, ministernotomy, or the transxyphoid approach. Despite their popularity, the advocates of the muscle-sparing alternatives claim that acute and late pain, and morbidity, are reduced.1–3 Thoracic surgeons have long considered the axillary thoracotomy as an optimal approach for pulmonary and mediastinal lesions.4-6 We claim no originality in describing our current approach, wishing only to highlight the possible advantages of a midaxillary thoracotomy that spares the major groups of external muscles. Furthermore, in contrast to the anterolateral approach, the midaxillary approach helps to hide the scar within axillary region when used in pre-pubescent females. In this subgroup of patients, the submammary grooves are not yet defined, thus presenting a problem in determining the exact position of the desired incision. The midaxillary incision is not even close to the future tissues of the breast, a fact that should avoid with certainty any impairment of mammary development (Fig. 2). Apart from the intercostal musculature, the approach obviates the need to divide or incise any other muscles. We have preferred to use a short horizontal midaxillary incision in the skin, as this does not compromise any axillary glands, and does cross Langer’s lines in perpendicular fashion. Especially today, where percutaneous closure of an atrial septal defect is becoming an accepted technique using catheters, substantial scaring or deformity needs to be avoided after any surgical intervention. Our described approach may represent a useful alternative. The technique we describe, nonetheless, is by no means “standard”. It requires not only thorough preoperative assessment of the nature of the interatrial communication, ensuring that it is within the oval fossa, but also requires that both the surgeon and the anaesthetist are experienced in minimal invasive surgery. The primary goal of this alternative approach, in our mind, is the avoidance of trauma to the future tissues of the breast, and midline scarring. The surgeon, however, must be fully acquainted with both the 1306-14.qxd 11/23/03 9:22 PM Vol. 13, No. 6 Page 567 Schreiber et al: Midaxillary thoracotomy in children 567 References Figure 2. The early postoperative result after using the muscle-sparing thoracotomy in a female patient aged 4 years and weighing 14.8 kg. surgical access and the technical aspects described, since the safety of an elective operation in an otherwise healthy patient must not be jeopardized by the introduction of procedures foreign to daily practice. 1. Landreneau RJ, Pigula F, Luketich JD, et al. Acute and chronic morbidity differences between muscle-sparing and standard lateral thoracotomies. J Thorac Cardiovasc Surg 1996; 112: 1346–1351. 2. Bendetti F, Vighetti S, Ricco C, et al. Neurophysiologic assessment of nerve impairment in posterolateral and muscle-sparing thoracotomy. J Cardiovasc Surg 1998; 115: 841–847. 3. Nomori H, Ohtsuka T, Horio H, Naruke T, Suemasu K. Difference in the impairment of vital capacity and 6-minute walking after a lobectomy performed by thoracoscopic surgery, an anterior limited thoracotomy, an anteroaxillary thoracotomy, and a posterolateral thoracotomy. Surg Today 2003; 33: 7–12. 4. Noirclerc M, Dor V, Chauvin G, et al. Extensive lateral thoracotomy without muscle section. Ann Chir Thorac Cardiovasc 1973; 12: 181–184. 5. Becker RM, Munro DD. Transaxillary minithoracotomy: the optimal approach for certain pulmonary and mediastinal lesions. Ann Thorac Surg 1976; 22: 254–259. 6. Mitchell R, Angell W, Wuerflein R, Dor V. Simplified lateral chest incision for most thoracotomies other than sternotomy. Ann Thorac Surg 1976; 22: 284–286. 7. Yang X, Wang D, Wu Q. Repair of atrial septal defect through a minimal right vertical infra-axillary thoracotomy in a beating heart. Ann Thorac Surg 2001; 71: 2053–2954. 8. Bleiziffer S, Schreiber C, Burgkart R, et al. Impaired development of the right mamma after right anterolateral thoracotomy in prepubescent female patients. Cardiol Young 2003; 13 (Suppl 1): 86. 9. Giamberti A, Mazzera E, Di Chiara L, Ferretti E, Pasquini L, Di Donato RM. Right submammary minithoracotomy for repair of congenital heart defects. Eur J Cardio-thorac Surg 2000; 18: 678–682. 10. Yoshimura N, Yamguchi M, Oshima Y, Oka S, Ootaki Y, Yoshida M. Repair of atrial septal defect through a right posterolateral thoracotomy: a cosmetic approach for female patients. Ann Thorac Surg 2001; 72: 2103–2105.