Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Determinants of Perceived Health in Patients With Left Ventricular
Dysfunction: A Structural Modeling Analysis
RAYMOND C. ROSEN, PHD, RICHARD J. CONTRADA, PHD, LARRY GORKIN, PHD, AND
JOHN B. KOSTIS, MD
Objective: Few studies have evaluated the determinants of perceived health in patients with chronic illness.
The present study was designed to evaluate the role of biomedical, demographic, and psychosocial influences
on global subjective health by means of a structural equation modeling approach.
Method: A conceptual model of perceived health was tested in a subsample of patients {N = 146) from the
multicenter Studies of Left Ventricular Dysfunction (SOLVD) trial. Domain-specific quality of life constructs
(emotional status, social support, and physical functioning), were assessed by means of multiple indicators.
These latent (mediating) variables, along with six single-indicator biomedical and background variables, were
modeled as predictors of a composite index of perceived health.
Results: A satisfactory fit was obtained for the proposed model, with practical fit indices ranging from .89 to
.95. High levels of perceived health were associated with low levels of emotional distress and high levels of
physical functioning. Social support was positively correlated with physical functioning and negatively
associated with emotional distress. Among the background variables, no direct associations were observed
between any of the single-indicator variables and perceived health. Several background variables (eg, age,
income, walk-test scores) had indirect effects via associations with the latent variables of physical functioning
and emotional distress.
Conclusions: These findings support the use of a structural modeling approach in assessing determinants of
perceived health in patients with congestive heart failure. Further research is needed to evaluate the utility of
the model in other patient populations.
Key words: perceived health, left ventricular dysfunction.
INTRODUCTION
Global subjective assessments of health status
have been strongly linked to mortality (1-6). Furthermore, when the effects of age, gender, and education are statistically controlled for, perceived
health has emerged as a consistently better predictor
of long-term mortality than objective measures of
physical health (3,7). Whereas previous research has
shown modest effects of physical health and psychosocial factors on self-assessment of health status (4,
8] there has been little effort to develop a multivariate model of the determinants of global subjective
health in selected patient groups (9). The purpose of
this study was to evaluate a path-analytic model of
perceived health in patients with left ventricular
dysfunction (LVD).
From the University of Medicine and Dentistry, Robert Wood
Johnson Medical School (R.C.R., J.B.K.), Rutgers-The State University of New Jersey (R.J.C.), and Pfizer Inc. (L.G.).
Address reprint requests to: Raymond C. Rosen, PhD, Department of Psychiatry, Robert Wood Johnson Medical School, 675
Hoes Lane, Piscataway, NJ 08854
Received for publication October 17, 1995; revision received
April 9, 1996.
Psychosomatic Medicine 59:193-200 (1997)
0033-3174/97/5902-0193S03.00/0
Copyright © 1997 by the American Psychosomjtic Society
Perceived health and quality of life are significantly affected in patients with congestive heart
failure (10-12) Many of these patients have limited
physical capacity, restricted social interactions, and
dysphoric mood, in addition to a poor overall prognosis. Although significant advances have been
made in the treatment of heart failure in recent years
(13-16), it is unclear whether patients' perceptions
of their health status have been affected accordingly
(17). Furthermore, the determinants of subjective
health assessments in symptomatic or asymptomatic
LVD patients have not been investigated, nor has the
predictive value of those assessments been examined. For the present study, we evaluated medical
and psychosocial determinants of global subjective
health in a subgroup of patients participating in the
multicenter Studies of Left Ventricular Dysfunction
(SOLVD) Trial.
The SOLVD investigation consisted of two, largescale double-blind, placebo-controlled trials designed to evaluate the effects of pharmacological
therapy (enalapril) on the mortality and morbidity of
patients with left ventricular dysfunction and overt
heart failure (treatment trial) or covert heart failure
(prevention trial) (18, 19). To assess the impact of
treatment on quality of life and other psychosocial
factors in congestive heart failure (CHF), a sub-study
193
R. C. ROSEN et al.
was conducted at five participating clinical centers
(University of Alabama at Birmingham, University of
Florida, Brown University, UMDNJ-Robert Wood
Johnson Medical School, and West Roxbury Veterans Administration Medical Center). Details of the
design and methodology of the sub-study are reported elsewhere (20).
In the present study, a structural-modeling approach was utilized to assess physical and psychological determinants of perceived health before randomization in patients participating in the SOLVD
trial. Analyses were guided by a conceptual model of
perceived health that included a set of relatively
distal, background factors, such as physical disease,
social-demographic characteristics and cognitive-intellectual functioning. A second set of more proximal determinants of perceived health ratings reflect
the person's appraisal of quality of life in various
domains, and consists of emotional status, perceived
social support, and self-assessment of physical functioning. Each of these domains was represented in
the final model.
Structural modeling provides simultaneous evaluation of a set of measurement models and structural
path coefficients. In a measurement model, latent
constructs, such as global subjective health or domain-specific self-assessments, are defined as combinations of two or more measured variables. Structural path coefficients reflect associations between
latent constructs or between single-indicator predictors and a latent construct. It was anticipated that
cross-sectional examination of this model would
facilitate longitudinal assessment of the effects of
LVD treatment on global subjective health, and the
relationship between perceived health and longterm survival. These latter comparisons will be reported in a separate publication.
METHOD
Subjects
A total of 318 patients were enrolled in the SOLVD quality-oflife sub-study. The major criteria for enrollment in the SOLVD
trial were an ejection fraction s 35%, and no myocardial infarction within 30 days before enrollment. Patients over the age of 80
years were excluded, in addition to those with unstable angina
pectoris, severe pulmonary disease, or any other disease likely to
affect long-term participation in the trial. Patient screening was
conducted independently by each of the study centers, and
included a 1-week, single-blind lead-in period to assess possible
adverse drug reactions. Uniform screening criteria were employed
at each center, which resulted in a similar distribution of age,
racial characteristics, and gender (20). All patients provided
informed consent prior to participation in the sub-study.
194
Measures
Measures included in the study were divided into five separate
categories: a) background characteristics; b) physical functioning;
c) emotional status; d) social support; and e) subjective health. A
complete description of the rationale and psychometric properties
of the measurement battery has been reported elsewhere (20, 21).
For purposes of the present analysis, assessment of background
characteristics included three primary demographic variables,
age, education, family income; and two biomedical indices, ejection fraction (EF) and the 6-Minute Walk Test (22). The latter test
has patients walk as far as possible along a level track for 6
minutes. The distance walked, in meters, is used as an objective
measure of functional status (22, 23). Ejection fraction and Walk
Test Scores served as proxy variables for prior illness (eg, history
of myocardial infarction). Also included among the background
variables was verbal intelligence, which was assessed using the
Vocabulary Test from the WAIS (24). Background variables were
selected for inclusion based upon availability of complete data for
each subject, adequate baseline distribution of scores, and reported association with perceived health in previous studies (4, 5,
8, 9).
Domain-specific quality of life measures were included to
assess emotional status, perceived social support, and physical
functioning. Emotional status was assessed by means of the Rand
Corporation's Mental Health Inventory (25). This is a 38-item
self-report instrument that comprises four primary sub-scales:
positive affect, behavioral control, depression, and anxiety. Each
of these scales shows a high degree of internal consistency. In
addition, factor analysis indicates that correlations among these
scales reflect a single, underlying mental health dimension (25,
26).
Perceived social support was measured by means of the Rand
Social Support Scale (27). This 19-item questionnaire includes
sub-scales measuring positive interactions, tangible support, emotional support, informational support, and affection. Internal
consistency (Cronbach's a) for the full scale was .97 in a previous
report (20).
Physical functioning was assessed using two measures. The
first consisted of 7 items from the Functional Status Scale (28),
which assesses physical and role limitations. The second consisted of three items from the Dyspnea Scale (29). This scale
measures breathlessness according to the magnitude and effort of
tasks involved.
The third major category of measures was global perceived
health. Previous research has demonstrated that items requiring
subjects to rate the overall quality of their physical health show
high levels of internal consistency and unidimensionality (30).
Three Likert-scale items were used for assessment of global
subjective health in the present study (31): "In general, would you
say your health is: very good, good, fair, poor"; "I am somewhat
ill: l = definitely true, 5=definitely false"; and "I am as healthy as
anybody I know in my condition: 1 = definitely true, 5 = definitely
false". The three items were combined into a single factor,
reflecting global perceived health. This factor correlated highly
with individual item scores (r <85), and was internally consistent.
Analytic Strategy
The analyses reported below reflect a general approach to
structural equation modeling (SEM) that is described by Joreskog
and Sorbom (32). An SEM analysis has two major components. The
measurement component involves associations between a set of
Psychosomatic Medicine 59:193-200 (1997)
DETERMINANTS OF PERCEIVED HEALTH
measured variables and a smaller number of latent constructs that
are the hypothesized determinants of the measured variables. The
measurement model also includes estimates of the associations
between latent constructs. Although this feature of SEM requires
that at least one of the constructs under study is measured using
multiple indicators, it is possible to include in the full SEM model
both single- and multiple-indicator variables.
The second component of an SEM analysis is the structural
component, which involves directional effects among constructs.
These effects may be direct, or indirect. Indirect effects involve
mediating pathways whereby the influence of one predictor on
the dependent variable of interest is partially or completely
accounted for by another, more proximal determinant of the
outcome.
Following a strategy outlined by Anderson and Gerbing (33),
we examined the core measurement component of the model
before the structural component. This involved an evaluation of
the hypothesis that responses to the domain-specific quality of
life measures reflect three latent constructs, namely, emotional
status, social support, and physical functioning. A measurement
model was defined for these constructs by permitting each of the
relevant test items or scale scores to load on a single factor
representing the latent construct it was hypothesized to measure.
These loadings were estimated as free parameters, and all other
factor loadings were constrained to equal zero. Correlations
among the latent constructs were unconstrained and also were
estimated as free parameters.
After evaluating the measurement model, we examined the full
SEM model. Structural path coefficients were estimated to reflect
the influence of the six, single-indicator, background variables on
each of the three domain-specific quality of life constructs, as well
as on the general subjective health construct. In addition, path
coefficients were estimated to reflect the influence of each of the
three domain-specific quality of life constructs on the general
subjective health construct.
All analyses were conducted using the LISREL VIII computer
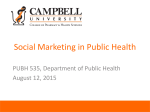
program (32). The complete SEM model submitted for analysis is
shown in Figure 1.
RESULTS
Characteristics of the Final Sample
Testing of the model was conducted on 146 subjects for whom complete data were available on all
variables included in the analysis model. Reasons
for missing data included patient non-compliance or
unavailability for testing, staff failure to administer
specific items or scales, and data entry errors or
omissions. While patients included in the trial were
no different on the major demographic variables (see
Table 1), small, but significant differences were
noted on indices of cardiovascular function. In particular, patients included in the trial had slightly
Fig. 1. Standardized maximum likelihood parameter estimates for a final structural model of the determinants of perceived health in
LVD patients. Pos. = positive; Behav. = behavior; Ctl .= Control; Int. = interaction.
Psychosomatic Medicine 59:193-200 (1997)
195
R. C. ROSEN et al.
TABLE 1. Demographic & Health Characteristics of Included Versus Excluded Study Patients
Variable
Age (yrs)
Gender (% male)
Race (% white)
Income (1-5)
Education (1-5)
EF (%)
NYHA(1-4)
Walk Test (meters)
Included patients (n = 146)
Excluded patients (n = 172)
p
Mean
SD
Mean
58.4
91.0%
95.8%
3.15
3.21
28.3
1.44
408.7
10.1
60.4
91.2%
91.7%
3.06
3.09
27.0
1.66
345.3
1.0
0.8
5.9
0.5
138.9
SD
9.2
0.7
0.6
6.4
0.7
160.4
NS
NS
NS
NS
NS
.05
.001
.001
EF = ejection fraction; NYHA = New York Heart Association classification of heart failure (1 = least severe, 4 = most severe); NS = not significant.
higher mean ejection fractions (28.3 vs. 27.0] and
lower mean scores on the New York Heart Association classification of heart failure (1.44 vs. 1.66).
Six-Minute Walk scores were similarly higher in the
included compared to excluded subjects (408.7 vs.
345.3). Overall, the sample was predominantly middle-aged (58.4 ± 10.1), male (91.0%), and white
(95.8%).
The Measurement Model
Table 2 presents the correlational matrix for all
variables examined in this study. The data array was
converted to a standard variance-covariance matrix
before structural modeling analyses were undertaken. Tests of normality were performed, and data
were found to be relatively normally distributed.
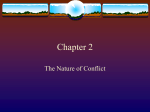
Table 3 presents goodness-of-fit indices examined
in this study. Model 1 is a measurement model
pertaining to the domain-specific quality-of-life
measures. Model 1 hypothesized that responses to
the 11 domain-specific quality-of-life measures reflect three latent constructs involving emotional distxess, perceived social support, and self-assessed
physical functioning. The null hypothesis associated
with Model 1 assumed that there is no covariation
among the variables measuring domain-specific
quality of life. Null models are used as standards
against which to evaluate the adequacy of substantive empirical models (32).
A significant *2 for Model 1, /(41) = 104.63, p <
.0001, indicated that this model is less than perfect
in the sense that the covariance matrix derived from
the model differs significantly from the observed
data. However, the #2 difference test indicated that
Model 1 fit the data better than the null model,
X2(14) = 1,431.6, p < .0001. Moreover, Model 1 fit
the data well in absolute terms as reflected by
practical fit indices ranging from .93 to .96 (see Table
3, Model 1). These values are analogous to estimates
196
of the proportion of variance in the observed data
that is accounted for by the model and should be .90
or higher in a well-fitting model.
The next stage in the analysis was to evaluate the
full SEM model that is depicted in Figure 1. The x*
test indicated that this model also showed less than
perfect fit, x2(131) = 223.9, p < .001. However, the
X2 difference test showed that Model 2 fit the data
better than its corresponding null model, x2(59) =
1,822.1, p < .0001. Practical fit indices ranged from
.89 to .95, indicating a satisfactory degree of fit (see
Table 3, Model 2).
Parameter estimates derived for the final model
are presented in Figure 1, These coefficients represent completely standardized, maximum likelihood
estimates of factor loadings and structural path coefficients. Not shown in Figure 1 are structural path
coefficients that failed to approach statistical significance at p < .05.
Measurement models for the three, domain-specific quality of life constructs generated substantial,
statistically significant factor loadings in the expected direction. Strictly speaking, zero-order correlations among these constructs are not part of the
SEM model, because they are statistically controlled
for in the calculation of structural path coefficients.
However, they are made available in the LISREL
output, and indicate moderate negative associations
between emotional distress and social support (r =
— .40), emotional distress and physical functioning
(r = —.48), and a positive association between social
support and physical functioning (r = .30). The
measurement model for global health perceptions
also indicated substantial, statistically significant
factor loadings in the expected direction.
Structural path coefficients representing predictive relationships between domain-specific and
global health self-assessments indicated that high
perceived health ratings reflected lower levels of
emotional distress (|3 = -0.28, p < .0001), and
Psychosomatic Medicine 59:193-200 (1997)
DETERMINANTS OF PERCEIVED HEALTH
I
I
I
i
i
i
i
I
I
I
I
higher levels of physical functioning (j3 = 0.68, p <
.0001). In addition, a slight trend was observed for
higher social support to be associated with lower
levels of perceived health (j8 = —0.15, p < .05).
As shown in Figure 1, a number of significant
associations were observed between single-indicator
background predictors and domain-specific quality
of life constructs. Age showed a modest inverse
relationship with emotional distress (/3= -0.21, p <
.01). Not surprisingly, the 6-Minute Walk Test was
predictive of the level of physical functioning
(|3 = 0.50, p < .001) and also showed a modest
negative association with emotional distress (/3 =
-0.20; p < .02) and positive association with social
support (/3 = 0.24; p < .01). There was a nonsignificant trend for educational status to be positively
associated with physical functioning (/3 = 0.16, p <
.10). Family income showed an inverse relationship
with emotional distress Q3 = -0.27, p < .002) and a
positive association with physical functioning (j8 =
0.26; p < .05). Neither ejection fraction nor verbal
intelligence showed significant associations with
any domain-specific quality of life constructs.
It is noteworthy that in no case was there a
statistically significant structural coefficient reflecting the effects of any of the background variables on
perceived health. The only such effect to approach
significance showed a direct, positive association
between family income and perceived health (j3 =
0.14, p < .10).
Inspection of standardized residuals and modification indices provided in the LISREL output indicated that overall goodness of fit of the model depicted in Figure 1 could be improved slightly if
parameters were added to estimate correlations between error terms for the social support measures,
rather than setting these correlations to zero as was
done in the analysis described above. This strategy
was not pursued since post hoc model adjustments
of this type may capitalize on chance variations.
DISCUSSION
S S S S ^ - o i S a ;
I I H 1 £ f IJ
Psychosomatic Medicine 59:193-200 (1997)
—
S 3
I 3 33
This is the first study of its kind to examine the
pattern of associations between global subjective
health and a broad array of objective and subjective
health indices in patients with left ventricular dysfunction. In the model presented, background factors
such as age, left ventricular function, intelligence,
and socioeconomic status were viewed as influencing perceived health via the mediating effects of
latent subjective variables, including emotional distress, physical functioning, and perceived social
197
R. C. ROSEN et al.
TABLE 3. Goodness of Fit Tests
Model
ModeM
Model 2
Goodness of Fita
Hypothesized
Null
Difference
104.63* (41)
233.91* (131)
1,536.24* (55)
2,045.97* (190)
1,431.61* (14)
1,8322.06* (59)
.93
.94
.93
.96
.95
" The first three columns contain x* values, with corresponding degrees of freedom given in parentheses. Values in columns 4 through 6 are
normed fit indexes (NFI), nonnormed fit indexes (NNFI), and comparative fit indexes. For columns 1 and 2, statistical significance indicates that
the model fails to account for the data. For column 3, statistical significance indicates that the hypothesized model provides improvement in fit
by comparison with the corresponding null model. The models are described in the text.
* p < .0001.
support. The latent variables in this model were
found to have a high degree of internal consistency,
and the overall model provided adequate predictive
power in accounting for the effects of both distal and
proximal determinants of perceived health. Furthermore, the use of a structural modeling approach
permitted simultaneous evaluation of the relationships between different classes of independent or
predictor variables, in addition to the association of
these variables with perceived health. Overall, these
findings provide strong support for the use of structural equation modeling in quality-of-life research,
and for the specific value of this approach in assessing determinants of global subjective health. Additionally, the model shows which elements or parameters patients used psychologically in arriving at
their rating of global subjective health.
Among the latent variables examined in the
present study, physical functioning was most
strongly related to perceived health. In patients with
left ventricular dysfunction, it thus appears that
perceived health is closely linked to the ability to
perform tasks of daily living and the relative absence
of dyspnea. This finding is consistent with results of
other studies indicating a positive relationship between these variables and severity of CHF (20, 34,
35). However, it should be noted that most patients
in the present study evidenced relatively mild degrees of heart failure (Class I and II) and had only
modest levels of physical disability associated with
the disease. It is therefore likely that other factors,
such as patients' knowledge and expectations regarding long-term effects of CHF on physical functioning, might partially account for the strength of
the association with global subjective health. Indeed,
this association might have been even stronger had
patients with more advanced heart failure been included in the study. In any event, these findings
underscore the importance of physical functioning
as a major determinant of perceived health in patients with CHF.
Emotional distress was negatively associated with
198
global subjective health, although the strength of this
relationship was relatively modest (fi = -0.28).
Similarly, a weak negative association was noted for
the dimension of social support (j3= -0.15). In
accounting for the negative effects of emotional
distress on subjective health, it should be noted that
the majority of patients in the present study (76.8%)
had previous myocardial infarctions (MI). Given the
growing evidence of depression and other emotional
disorders in post-MI patients (36-38), it is not surprising that emotional distress was evident in our
sample, and that it contributed significantly to perceived health. On the other hand, social support has
also been linked to survival in post-MI patients
(39-41) and the lack of positive association with
perceived health warrants explanation. It is possible
that the measure of social support used in this study
did not adequately capture the dimensions relevant
to this population, or that social support may affect
survival through other means.
Few direct effects on perceived health were observed for the independent or background variables,
including age, ejection fraction, 6-minute walk, income, education, and verbal intelligence. In fact, the
only association to attain even marginal significance
was that between income level and perceived health
(/3 = 0.14). Additional effects of the independent
variables on global subjective health were shown
indirectly via association with the latent variables.
Thus, age and walk test scores were both negatively
associated with emotional distress, whereas income,
education, and walk scores all correlated positively
with physical functioning. The lack of direct association between age and either perceived health or
physical functioning is noteworthy, given evidence
from other studies that age contributes negatively to
both physical functioning and perceived health (9,
42). It is possible that the limited age range of our
patients may have obscured this relationship. On the
other hand, a negative association was observed in
our study between age and emotional distress (ie,
older patients rated themselves as less distressed),
Psychosomatic Medicine 59:193-200 (1997)
DETERMINANTS OF PERCEIVED HEALTH
which is consistent with the findings of an earlier
study of psychosocial factors in chronic illness (43].
In contrast to the highly significant association
between walk test scores and physical functioning,
left ventricular ejection fraction failed to predict any
latent or dependent variables in the study. This
finding is consistent with results of other studies
showing little or no relationship between ejection
fraction and measures of functional status or quality
of life (20, 44, 45). Several factors might account for
the lack of association between this well-established
measure of disease severity and functional status,
although the most likely explanation is the relatively
truncated range of ejection fraction levels in most
multicenter clinical trials of heart failure (20).
A major limitation of the present study was the
homogeneity of the patient sample, which included
few minority or female subjects. According to Johnson and Wolinsky (9), the determinants of perceived
health in older adults vary according to both gender
and race. Therefore, it would be necessary to replicate the current findings in women or minority
patients with LVD if the model is to be generalized to
these populations. As noted above, individuals with
more advanced degrees of heart failure or a greater
degree of disability also were not included in the
present study. Inclusion of these individuals may
have strengthened the relationship between physical
functioning and global subjective health. Alternatively, emotional distress may have played a greater
role in determining perceived health if more disabled patients were included in the sample.
Despite the advantages of the structural modeling
approach for theory development and testing, certain weaknesses should also be noted. First, the
analyses were conducted using only subjects for
whom complete data were available, which represented less than half of the total sample studied.
Since the present study was also based upon a
secondary analysis of the SOLVD quality-of-life substudy data, weaknesses and omissions in the original
data set could not be corrected. The number of
subjects included in the analysis may have been less
than optimal considering the number of independent variables in the study (46), although other
authors have argued for the value of structural modeling analyses with even smaller sample sizes (47,
48). The limitation in sample size may have implications for the reliability of the model, however,
which warrants replication in a larger sample. Additionally, the model was developed and tested
solely on cross-sectional baseline data, which limits
the degree to which the results may reflect causal
associations. Thus, for example, global subjective
Psychosomatic Medicine 59:193-200 (1997)
health estimates may have influenced subjects' perceptions of physical limitations or emotional wellbeing. Finally, the maximum likelihood procedure
used to generate parameter estimates makes certain
assumptions regarding the structure of the data (eg,
multivariate normality), and it is possible that some
alternative method would have yielded superior
estimates.
Several clinical implications are apparent from the
findings of the present study. First, it would appear
that intervention programs aimed at improving
global health perceptions in patients with heart
failure should be directed at both increasing physical functioning and relieving emotional distress. In a
recent study in our laboratory examining drug and
nondrug treatments for CHF (9), we have noted
marked improvements in both objective and subjective measures of health in patients receiving a combination of structured exercise training and groupbased cognitive therapy. Older patients with CHF
should be targeted for such interventions as much as
younger patients, given that physical functioning
appears to be an especially important determinant of
perceived health in these patients.
REFERENCES
1. Mossey JM, Shapiro E: Self-rated health: A predictor of
mortality among the elderly. Am J Public Health 72:800808,1982
2. Kaplan G, Barell V, Lusky A: Subjective state of health and
survival in elderly adults. J Gerontol 43:Sll4-Sl20,1988
3. Idler EL: Self-assessed health and mortality: A review of
studies. In S Maes, H Leventhal, M Johnston (eds), International Review of Health Psychology, New York; Wiley, 1992,
33-54
4. Idler EL, Kasl, SV, Lemke JH: Self-evaluated health and
mortality among the elderly in New Haven, Connecticut, and
Iowa and Washington Counties, Iowa, 1982-1986. Am J Epidemiol 131:91-103, 1990
5. Wannamethee G, Shaper AG: Self-assessment of health status
and mortality in middle-aged British men. Int J Epidemiol
20:239-245, 1991
6. Wolinsky FD, Johnson RJ: Perceived health status and mortality among older men and women. J Gerontol 47:S304S312, 1992
7. Idler EL, Kasl, SV: Health perceptions and survival: Do global
evaluations of health status really predict mortality? J Gerontol Soc Sci 46:555-565, 1991
8. Kaplan GA, Camacho T: Perceived health and mortality: A
nine-year follow-up of the Human Population Laboratory
cohort. Am J Epidemiol 117:292-304, 1983
9. Johnson RJ, Wolinsky FD: Gender, race, and health: The
structure of health status among older adults. Gerontologist
34:24-35, 1994
10. Dracup K, Walden JA, Stevenson LW, Brecht M: Quality of
life in patients with advanced heart failure. J Heart Lung
Transplant 11:273-279, 1992
199
R. C. ROSEN et al.
11. Rogers WJ, Johnstone, DE, Yusuf S, et al: Quality of life among
5,025 patients with left ventricular dysfunction randomized
between placebo and enalapril: The Studies of Left Ventricular Dysfunction. J Am Coll Cardiol 23:393-400, 1994
12. Schron E, Gorkin L, Garg R: Evaluating quality of life in
congestive heart failure. In GT Kennedy, MH Crawford (eds).,
Congestive Heart Failure: Current Clinical Issues, New York,
Futura Publishing, 1994, 121-135
13. Hobbs RE, Czerska B: Congestive heart failure: Current and
future strategies to decrease mortality. Postgrad Med 96:167172, 1994
14. Kubo SH, Cohn JN: Approach to treatment of the patient with
heart failure in 1994. Adv Intern Med 39:485-515, 1994
15. White M, Rouleau JL: Overview of clinical trials in congestive
heart failure. Can J Cardiol 9:629-634, 1993
16. Uren NG, Lipkin DP: Exercise training as therapy for chronic
heart failure. Br Heart J 67:430-433, 1992
17. Wenger NK, Furberg CD: Cardiovascular disorders. In Spilker
B (ed). Quality of Life Assessments in Clinical Trials, New
York, Raven Press, 1990, 335-446.
18. The SOLVD Investigators: The Studies of Left Ventricular
Dysfunction (SOLVD)-rationale, design and methods: Two
trials that evaluate the effects of enalapril in patients with
reduced ejection fraction. Am J Cardiol 66:315-322, 1990
19. The SOLVD Investigators: Effect of Enalapril on survival in
patients with reduced left ventricular ejection fractions and
congestive heart failure. N Engl J Med 325:293-302, 1991
20. Gorkin, L, Schron EB, Brooks MM: Psychosocial predictors of
mortality in the Cardiac Arrhythmia Suppression Trial
(CAST). Am J Cardiol 71:263-267, 1993
21. Diener E: Subjective well-being. Psychol Bull 95:542-575,
1984
22. Guyatt GH, Sullivan MJ, Thompson, PJ et al: The 6-minute
walk: A new measure of exercise capacity in patients with
chronic heart failure. Can Med Assoc J 132:919-923, 1985
23. Bittner V, Weiner DH, Yusuf S, et al: Prediction of mortality
and morbidity with a six-minute walk test in patients with left
ventricular dysfunction. JAMA 270(14):1702-1707, Oct 1993
24. Wechsler D: The WAIS-R Manual. New York, Psychological
Corporation, 1981.
25. Veit CT, Ware JE: The structure of psychological distress and
well-being in general populations. J Consult Clin Psychol
51:730-742, 1983
26. Hays RD, Stewart AL: The structure of self-reported health in
chronic disease patients. J Consult Clin Psychol 2:22-30,1990
27. Sherbourne CD, Stewart AL: The MOS social support survey.
Soc Sci Med 32:705-714, 1991
28. Stewart AL, Ware, JE, Brook RH: Advances in the measurement of functional status: Construction of aggregate indexes.
Med Care 19:433-438, 1981
29. Mahler DA, Weinberg DH, Wells CK, Feinstein AR: The
measurement of dyspnea: Contents, interobserver agreement,
and physiological correlates of two new clinical indexes.
Chest 85:751-758, 1984
30. Hays RD, Marshall GN, Wang EY, Sherbourne CD: Four-year,
cross-lagged associations between physical and mental health
in the Medical Outcomes Study. J Consult Clin Psychol
62:441-449, 1994
200
31. Ware JE, Karmos AH: Development and validation of scales to
measure perceived health and patient role propensity. Vol.11
of final report. VirginiaTechnical Information Services, NTIS
Publication No. PB-288-231, 1976
32. Joreskog KG, Sorbom D: LISREL VIH: Structural equation
modeling with the SIMPLIS command language. Chicago:
Scientific Software International, 1993
33. Anderson JC, Gerbing DW: Structural equation modeling in
practice: A review and recommended two-step approach.
Psychol Bull 103:411-423, 1988
34. Feinstein AR, Fisher MB, Pigeon JG: Changes in dyspneafatigue ratings as indicators of quality of life in the treatment
of congestive heart failure. Am J Cardiol 64:50-55, 1989
35. Dracup K, Walden JA, Stevenson LW, Brecht M: Quality of
life in patients with advanced heart failure. J Heart Lung
Transplant 11:273-2791992
36. Frasure-Smith N, Lesperance F, Talajic M: Depression following myocardial infarction: Impact on 6-month survival. JAMA
270:1819-1825, 1993
37. Fielding R: Depression and acute myocardial infarction: A
review and reinterpretation. Soc Sci Med 32:1017-1027,1991
38. Schleifer SJ, Macari-Hinson MM, Coyle DA, et al: The nature
and course of depression following myocardial infarction.
Arch Intern Med 149:1785-1789, 1989
39. Case RB, Moss AJ, Case N, et al: Living alone after myocardial
infarction: Impact on prognosis. JAMA 267:520-524, 1992
40. Gorkin L, Schron EB, Brooks MM: Psychosocial predictors of
mortality in the Cardiac Arrhythmia Suppression Trial
(CAST). Am J Cardiol 71:263-267, 1993
41. Ruberman W, Weinblatt E, Goldberg JD, Chaudhary BS, Psychosocial influences on mortality after myocardial infarction.
N Engl J Med 311:552-559, 1984
42. Liang J: Self-reported physical health among aged adults. J
Gerontol 41:248-260, 1986
43. Cassileth BR, Lusk EJ, Strouse TB, et al: Psychosocial status in
chronic illness: A comparative analysis of six diagnostic
groups. N Engl J Med 311:506-511, 1984
44. Franciosa JA, Park M, Levine TB: Lack of correlation between
exercise capacity and indexes of resting left ventricular performance in heart failure. Am J Cardiol 47:33-39, 1981
45. Willens HJ, Blevins RD, Wrisley D, et al: The prognostic value
of functional capacity in patients with mild to moderate heart
failure. Am Heart J 114:377-382, 1987
46. Boomsma A.: On the robustness of LISREL against small
sample size and nonormality. Unpublished doctoral dissertation. University of Groningen, Groningen, Sweden.
47. Tanaka JS: "How big is big enough?" Sample size and goodness of fit in structural equation models with latent variables.
Child Dev 58:134-146, 1987
48. Gebring DW, Anderson JC: The effects of sampling error and
model characteristics on parameter estimation for maximum
likelihood confirmatory factor analysis. Multivariate Behav
Res 20:255-271, 1985
49. Kostis JB, Rosen RC, Cosgrove NM, et al: Nonpharmacologic
therapy improves functional and emotional status in congestive heart failure. Chest 106:1001, 1994
Psychosomatic Medicine 59:193-200 (1997)