Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
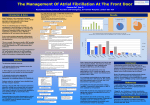
Rose Medical Center ED Atrial Fibrillation Algorithm Addendum B Initial Assessment AFib symptoms detected in triage Immediate EKG (Within 10 min) and notify attending provider Assess patient’s symptoms and hemodynamic status: palpitations, dyspnea, chest pain/discomfort, fatigue, dizziness, hypotension, mental status, etc. Acquire vital signs and apply oxygen Labs to be done: CBC, CMP, TSH, Mag, PT/INR Consider Echocardiogram if not already completed TO BE DETERMINED BY ED PROVIDER Atrial Fibrillation or atrial flutter? Paroxysmal or new onset/newly recognized? Persistent/Chronic with new rate problem? Duration (< 48hrs or > 48hrs or unknown) CHADsVASC Score (see up to date for reference on calculating) o If ≥ 2, consider anticoagulation Anticoagulated adequately already? – defined as on warfarin with INR ≥ 2 for 3 weeks or on another DOAC for 3 weeks with no missed doses (**this changed from 4 weeks w the 2014 updated guidelines) Is the ventricular rate controlled? Is the patient on antiarrhythmic therapy? Recent symptoms of TIA or CVA? Undiagnosed underlying condition (ACS, dehydration, acidosis, hypovolemia, sepsis, valve disease, hypoxia, electrolytes, PE, recent surgery, ETOH, hypothermia, hypotension) Signs of poor perfusion (Uncomfortable or rate > 150 bpm) Symptomatic hypotension Pulmonary edema (acute heart failure) Chest pain/angina Rate or Rhythm Control Strategy as outlines on Pages 2-3 HEMODNAMICALLY STABLE? YES NO Consider urgent external cardioversion if AFib believed to be etiology or contributing to current instability - reference Addendum C and/or ACLS tachyarrhythmia Algorithm on Crash Cart Risk/benefit assessment required as it applies to thromboembolism complications Anticoagulation should be started as soon as possible and continued for at least 4 weeks after cardioversion unless contraindicated 1 Rose Medical Center ED Atrial Fibrillation Algorithm Addendum B RATE CONTROL STARTEGY ED HEMODYNAMICALLY STABLE AFIB Consider rate control FIRST for patients with Persistent AFib who: Have a contraindication to antiarrhythmic drugs Do not meet criteria for cardioversion RATE CONTROL ASSESSMENT Assess underlying conditions that affect rate control (CHF, Hypoxemia, hypovolemia, sepsis, COPD, thyrotoxicosis, etc) Atrial fibrillation vs Atrial Flutter Symptomatic? HR > 100 or <100 bpm? Symptomatic Rate > 100 Consider IV diltiazem per hospital approved protocol; use caution if noted decompensated CHF Consider IV metoprolol tartrate 2.5-5mg bolus over 2 min, up to 3 doses If further rate control needed, consider Digoxin 0.25 mg IV w/ repeat dose to max of 1.5 mg over 24 hrs Refer to ACLS Tachyarrhythmia Algorithm PO AV nodal blocking agents (beta blockers, diltiazem, or digoxin). Use caution with BB in pts with pulmonary dx or known EF < 35% IV drugs only if unable to take PO Refer to ACLS Tachyarrhythmia algorithm Rate control NOT ACCOMPLISHED, significant ongoing symptoms or other conditions requiring immediate attention Rate < 100 Asymptomatic rate > 100 Admission to telemetry floor Refer to ACLS Tachyarrhythmia protocol and Addendum C AV nodal blocking drugs likely not needed if rate is consistently controlled (both at rest and with exertion) Rate control ACCOMPLISHED, no significant ongoing symptoms and no other conditions requiring immediate attention Consider discharge with oral rate control and OAC per their CHADsVASc score. Follow up as outpt with PCP or cardiology 2 Rose Medical Center ED Atrial Fibrillation Algorithm Addendum B RHYTHM CONTROL STARTEGY ED HEMODYNAMICALLY STABLE AFIB Consider Rhythm Control FIRST for patient with persistent AFib who: Are symptomatic Have an AFib duration of 48hrs or LESS. If AFib has been present > 48 hrs, unless therapeutic anticoagulation for the past 3 weeks can be verified, DO NOT attempt Rhythm Control without TEE CHRONIC AND ADEQUATE ANTICOGULATION? Defined as on warfarin with INR ≥2 for 3 weeks (**this is a change from 4 wks w/ the 2014 updated guidelines) or on a DOAC for 3 weeks with no missed doses. NO YES DURATION OF AFIB < 48HRS YES DURATION OF AFIB > 48HRS or UNKNOWN NO Significant ongoing symptoms or other conditions requiring immediate attention Consider external electrical cardioversion or Consider pharmalogical cardioversion Anticoagulate per CHADsVASC score Consider starting antiarrhythmic medication with cardiology consult Evaluation of structural heart disease +/coronary eval, if not previously done Rhythm control ACCOMPLISHED and/or no significant ongoing symptoms and no other conditions requiring immediate attention Consider emergent DCCV – see addendum C Consider TEE guided electrical cardioversion Consider pharmalogical cardioversion Anticoagulate per CHADsVASC score Consider starting antiarrhythmic medication with cardiology consult Evaluation of structural heart disease +/coronary eval, if not previously done Admission to telemetry floor Consider external electrical cardioversion or Consider pharmalogical cardioversion Anticoagulate per CHADsVASC score Consider starting antiarrhythmic medication with cardiology consult Rhythm control ACCOMPLISHED and/or no significant ongoing symptoms and no other conditions requiring immediate attention Consider discharge with oral rhythm control and OAC per their CHADsVASc score. Follow up as outpt with PCP or cardiology 3