Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Myocardial infarction wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Antihypertensive drug wikipedia , lookup
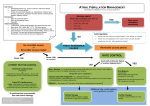
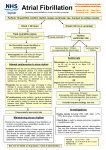
The Management Of Atrial Fibrillation At The Front Door Saxena AK, Iyer A Acute Medicine Department, Accident and Emergency, St Thomas’ Hospital, London SE1 7EH Introduction & Aims Atrial Fibrillation is the commonest presenting cardiac arrhythmia, with a prevalence of 9% in 80-90 year olds, and accounting for 3-6% of acute admissions to hospital in the UK. Fig.1 A&E Protocol based on 2006 NICE Guidelines [1]. Results •Confirmed diagnosis of AF- on ECG •General measures- O2, IV access, bloods (FBC, U+E, LFTs, Bone, Clotting, Glucose, Mg, TFT’s) •Treat pain, hypoxia, hypovolaemia, myocardial ischaemia •Is patient haemodynamically unstable- if so is this due to AF? Haemodynamic instability secondary to AF Life threatening? This is an audit which aims to review the management of atrial fibrillation or flutter (AF) with rapid ventricular response (FAF) in an Accident and Emergency Department (A&E) where there is an established Acute Medicine team. 2006 NICE guidelines for AF were used as the standard [1]. It also reviews whether appropriate antithrombotic therapy was administered using appropriate stroke risk stratification. Pt known to have AF previously? Emergency electrical cardioversion under sedation/GA Yes No -iv beta-blockers or ca antagonist Emergency electrical cardioversion under sedation/GA If delay in organising electrical cardioversion -iv amiodarone if above contraindicated Anticoagulation Emergency intervention should be performed as soon as possible. The initiation of anticoagulation should NOT delay any emergency treatment. -iv amiodarone In acute-onset AF- give heparin (if no contraindications), continue till a full assessment has been made eg thrombo-embolic risk stratification (see AF haemodynamically stable algorithm) This is a re-audit. The previous audit in 2007 revealed the inappropriate use of Digoxin in the management of FAF. Beta-blockers and DC cardioversion were underused. Following this audit a protocol for the management of FAF was instituted, based on the NICE guidance (Fig.1). All doctors and nurses in A&E were made aware of this protocol at departmental meetings. Yes No If sure AF onset less than 48 hrs ago no need to anticoagulate unless: Unable to restore sinus rhythm within 48 hrs Anticoagulation recommended by thromboembolic risk stratification History of failed cardioversions/ recurrences Structural heart disease Confirmed AF- haemodynamically stable Determine thromboembolic risk and anticoagulate appropriately: High risk (anticoagulate with warfarin and clexane, if contraindicted-give aspirin) Previous ischaemic stroke/TIA or thromboembolic event Methods Age ≥75 with hypertension, diabetes or vascular disease (CAD/PVD) Clinical evidence of valve disease, heart failure Moderate risk (consider each individual pt, warfarin or aspirin may be indicated) The following standards were set: Age ≥65 with no high risk factors Age <75 with hypertension, diabetes or vascular disease (CAD/PVD) 1. All patients should receive treatment as per the NICE 2006 Guidelines for AF. Low risk (start aspirin- loading dose 300mg, continue with 75 mg OD) •Age <65 with no moderate or high risk factors 2. Where Digoxin is prescribed first line, this is done appropriately and the reasons for this documented. 3. All patients should receive appropriate antithrombotic treatment as guided by an appropriate risk stratifying system, e.g. CHADS2 [2]. Patients coded for ‘arrhythmia’ were identified from the A&E computer database. Starting in August 2009, 189 consecutive admission electronic records were reviewed (both the scanned A&E notes and the electronic discharge summary). From these 50 patients (>18 years) were identified as been admitted with AF or Atrial Flutter with a ventricular rate > 100. Data pertaining to the patient demographics, clinical features, drugs/management used, antithrombotic use, CHADS2 score and patient outcome were recorded in a proforma. Chart 1 shows the age distribution and 2 the % with which presenting rhythm. The minimum ventricular rate was 114 beats/min. 64% of patients were managed in A&E Resus and 30% in Majors. 39/50 patients were previously not on any antiarrhythmic, 61.5% of these were given 1st line treatment with a beta – blocker (not Sotalol) as per guidance (39% in 2007). Rhythm or Rate? •many instances both are options- the choice is balance of various factors •discuss options with patient Consider Rhythm- control first if: Symptomatic Younger Presenting for first time with lone AF AF secondary to treated/corrected precipitant With congestive heart failure Consider Rate-control first if: Over 65 With coronary artery disease Mitral stenosis Known large atrium AF>12 months Hx of failed attempts at cardioversion Secondary to ongoing but reversible cause of AF (eg thyrotoxicosis/sepsis) Standard beta-blocker 21% of patients received digoxin as initial therapy compared with 32% in 2007 (Chart 4). 38% of these had a documented reason for its use, and 12.5% received this as per NICE guidance. Yes Beta-blocker or ca antagonist Structural heart disease? Yes Amiodarone Class 1c (flecainide/propafenone) Drug ineffective/ contraindicated. Previous relapse while on beta-blocker/sotalol/class 1c Only consider digoxin, as adjunct if above not working, or in sedentary elderly pts Most of the patients received antithrombotic therapy, however more could have been discharged on warfarin. Documentation of risk stratification for stroke needs to improve. CHADS2 scoring could be added to the protocol. References 1. NICE (2006) Atrial Fibrillation: The management of atrial fibrillation. CG36. London: National Institute for Health and Clinical Excellence. Overall 78% of patients were judged to have had the appropriate treatment (including DCCV) for AF as per NICE algorithms. 2 Gage BF et al. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001; 285:2864-2870 42% of patients were in AF on discharge, of these 95% were on antithrombotic therapy. 10 patients had a CHADS2 score of >1. Of these 3 had risk stratification documentation on admission and 6 were planned for warfarin on discharge. Acknowledgements No Sotalol or Following the previous Audit there has been an improved compliance with the NICE guidelines. More patients are being appropriately prescribed beta blockers and having acute DCCV. Although the use of digoxin is less it still continues to be overused. Of 5 patients who had clinical features of being ‘unstable,’ 2 received DC cardioversion. In 2007 8 were ‘unstable’ but nil had DCCV. Is rate control therapy needed?- aim for resting rate less than 90bpm Drug ineffective/ contraindicated. Previous relapse while on beta-blocker Conclusion Thank you to Dr N Drake, Consultant in Emergency Medicine for providing the data and protocol from the previous 2007 A&E Audit.