Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
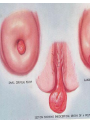
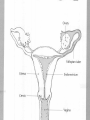
Applied Female Reproductive Physiology and the Anatomy of the Female Genitourinary System • Modified from material provided by Professor Michael Chapman • Revised February 2017 • The multiparous cervix Cervical erosion – better called “Ectropion” Cervical polyp CERVICAL CANCER Bimanual Palpation of the Uterus Ultrasound-guided vaginal egg collection for IVF Hysteroscopy • Normal Female Pelvis Laparoscopic view of pelvis Filshie Clips for Tubal Ligation Tubal Dye Studies Some pelvic pathology that can be seen by laparoscopy • Types of uterine fibroids or leiomyomas ENDOMETRIOSIS External Genitalia (Female) Episiotomy Marsupialization of a Bartholin’s Cyst • Structural abnormality Imperforate hymen Anatomical abnormality Double vagina Uterus didelphys Embryology of the male and female genital tracts The Pelvic Floor The pelvic floor from below Uterine Supports Laparoscopic view of pelvis Types of Prolapse Course of the Ureter in Females Hysterectomy complications Reproductive Physiology (Female) Ovarian function begins with PULSATILE release of a SINGLE GnRH from the hypothalamus into the pituitary portal system Female Menstrual Cycles Implantation ENDOMETRIAL CYCLE Changes in during cycle uterine lining Window of Receptivity Intervening in the Human Menstrual Cycle • Combined Oral Contraceptive (The Pill) • • • • • • Daily oestrogen and progesterone taken by mouth Inhibits FSH (and LH) release So a follicle never develops And ovulation never occurs It is essentially a state of “mini pregnancy” The synthetic oestrogen and progesterone will stimulate endometrial growth and decidual change • Endometrial shedding will occur if the pill is stopped and the levels of (synthetic) oestrogen and progesterone fall • This occurs during the week of “sugar tablets” • But it is not necessary every month hence the “3-month” pill Intervening in the Human Menstrual Cycle -2 • Ovarian stimulation for IVF • A long-acting GnRH agonist or antagonist is injected • This switches off the pituitary – no endogenous FSH and no LH surge • FSH is injected in supra physiological concentrations • So that more than one follicle is stimulated to grow • At the stage of optimal follicle growth and egg development an injection of HCG is given as an LH surrogate • Eggs are collected exactly 36 hours later for IVF • Embryo(s) are transferred in the proliferative phase of the cycle to a receptive endometrium • HCG injections are continued to sustain the corpus lutea OR • Progesterone is given to sustain the endometrium to prevent menstruation The Development of the Female WHAT MAKES A GIRL, A GIRL? The Development of the Female XX vs XY Chromosomal Determination The Development of the Female Action through specific genes on X differentiation Ovaries Mullerian ducts tubes, uterus,upper 1/3 vagina The Development of the Male specific genes on Y chromosome (eg SRY-1) differentiation testis testosterone Internal genitalia prostate ,seminal vesicles, vas, epididymis, descent of testes AMH/MIF Mullerian duct suppression no uterus,tubes, upper vagina Some causes of abnormal sexual development - Chromosomal abnormalities Androgen receptor defects Steroid synthesis malfunction Exogenous hormone exposure Hypothalamic or pituitary problems Gonadal problems Anatomical abnormality Turner’s Syndrome • Chromosomes 45 XO • Short stature, low hairline, webbed neck, primary amenorrhoea • Normal female external & internal genitalia but with streak ovaries • 1:5000 females but common aneuploidy in miscarriage • Will “menstruate” on The Pill • Can carry a pregnancy if primed with E2 and PROG and donated egg/embryo Chromosomal abnormality Turner’s Syndrome Gonadal dysgenesis Klinefelter’s Syndrome • Chromosomes 47 XXY • Tall males sometimes with gynaecomastia • Normal male external genitalia but with small, soft testes and ↓testosterone • 1:750 males but may never be detected • Commonly infertile with azospermia • Can be assisted to fatherhood using IVF/ICSI if any sperm can be found Chromosomal abnormality Klinefelter’s Sydrome Kallmann’s Syndrome • Chromosomes can be 46XY or 46XX • Absence of GnRH from the hypothalamus results in... • Hypogonadotrophic hypogonadism • Also have anosmia • 1:4,000 males and 1:12,000 females • Have male or female genitalia but will not enter puberty • Can be treated with sex steroids or FSH/LH Gene defect Kallmann’s Syndrome Androgen Insensitivity Syndrome • Chromosomes 46XY (≈ 1 per 2000 girls) • Classically a result of absent androgen receptors so all cells are unresponsive to testosterone • Have female external genitalia but absent uterus and vagina and undescended testes • Present with primary amenorrhoea but good breast development, absent pubic hair • Testes are usually surgically removed • But what do you tell these girls? Androgen receptor defect Testicular feminisation Androgen insensitivity syndrome Congenital Adrenal Hyperplasia • Chromosomes can be 46XY or 46XX • A block in cortisol synthesis causes ↑ACTH and ↑androgens by the adrenals • Females will exhibit virilization • Babies have fused labia and clitoramegaly • May require urgent identification and treatment with cortisol etc soon after birth Endogenous androgen excess Congenital adrenal hyperplasia 5-alpha-reductase deficiency • This enzyme converts Testosterone to Dihydrotestosterone in peripheral tissue • Affects males i.e. those who are XY • Often raised as girls because testes are undescended at birth and external genitalia appear female with hypospadias • However identify as male & undergo spontaneous sex change at puberty when T levels rise and DHT is produced by alternative enzymes in the liver and testes • Autosomal recessive condition. Very rare, seen only in Dominican Republic, PNG and Turkey • Affects 1:90 males in the remote village of Salinas in the Dominican Republic where they are called “Guevedoces” = “penis at 12” Catherine and his cousin Carla “Guevedoces” from the Dominic Republic feature in Michael Mosely’s BBC Feature, “The Extraordinary Making of You” For further information on disorders of sexual development... • Consult “Intersex” on Wikipedia Please leave a note on the Welcome Page to this website Any Questions or Comments?