Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
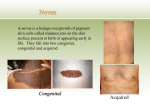
Melasma Dr Z. Shahmoradi Associate professor of dermatology melanogenesis Melanin is produced in melanocytes and stored in melanosomes within the keratinocytes. 1) The number, 2) melanin content, 3) and location of these melanized cells (along with oxygenated and deoxygenated hemoglobin) help determine the color of the skin. Melanocytes contain tyrosinase, a coppercontaining enzyme, that catalyzes the conversion of L-tyrosine to L-dopa and L-dopa to L-dopaquinone in melanin synthesis. Melasma is a dysfunction of this pigmentary system, resulting in an irregular brown or grayishbrown facial hypermelanosis. Causes of acquired hyperpigmentation Skin disease and conditions: Melasma, erythromelanosis follicularis, poikiloderma of civatte, PIP, Riehl’s melanosis Exogenous causes: cosmetics, drugs (estrogens, tetracyclines, amiodarone, phenytoin, phenothiazines, sulfonamides, aldacton), photosensitizing agents (bergamot oil, furocoumarins), UV (melasma, freckle, solar lentigo) Other causes: Addison, hemochromatosis, liver disease, pituitary tumors, pregnancy, hyperthyroidism Melasma Acquired, brown hypermelanosis of the face that develops slowly & symmetrically. Female (90%) , Male (10%) Etiology: Sunlight, pregnancy, genetic, racial, endocrine (thyroid dysfunction,…) In men with melasma: higher LH & lower testosterone Stress: release of MSH can be influenced by stress 50-70% of pregnant women & 8-30% with OCP ..Melasma Centrofacial=63% in cheeks, forehead, upper lip, nose, chin Malar=21% in cheeks & nose Mendibular=16% in ramous mendibular Centrofacial localization of melasma(63%) Malar localization of melasma(21%) Mandibular localization of melasma(16%) Chloasma: can resolve within a few months after delivery and treatment may not be necessary. However, there are many cases in which the disorder persists indefinitely. Pregnancy-associated melasma may be caused by an increase in placenta, ovarian, and pituitary hormones. Melasma has also been attributed to an elevation of melanocyte-stimulating hormone (MSH), estrogen, and progesterone leading to increased melanogenesis. Pathology In epidermal type: increased number of melanocyte & melanocyte activity increased melanization transport of melanosomes to epidermal cells In dermal type: melanophage in dermis (papillary & reticular) ..Melasma Examination with Wood’s lamp: 1) Epidermal, enhancement of pig. [70%] 2) Dermal, no enhancement 3) Mixed, slightly enhancement 4) a type seen in type 5-6 skin in which the lesions are not discernible under a wood’s light. D.D Actinic lichen planus Drug-induced hyperpigmentation Riehl’s melanosis Poikiloderma of Civatte Exogenous ochronosis Erythema dyschromicum perstans PIP Treatment of melasma Treatment of Melasma Eliminate inciting agents: drugs, cosmetics HQ alone > 3% Tretinoin 0.05%-0.1% HQ with retinoic acid, Arbutin, Kojic acid (2-4%) ,Mandelic acid , Azelaic acid 20% , Steroid,... Broad-spectrum sunscreen 4-isopropyl catechol (66%) N-acetyl-4-cysteine 3% …Treatment of melasma Chemical peeling: glycolic acid 30-70% , TCA 10-35% , S.A 20-30% Dermabrasion, microdermabrasion Lasers: Erbium:YAG , Q-switched , CO2- laser General management General management recommendations that assist in the clearing of melasma include discontinuation of birth control pills, scented cosmetic products, and phototoxic drugs, coupled with UV protection with use of broad spectrum (UVA+UVB) sunscreens. Solar exposure exacerbates melasma ,and its avoidance is fundamental for the successful management of the disease. Hydroquinone: HQ remains one of the most prescribed agents for melasma and is considered the gold standard of therapy, especially for epidermal melasma. The epidermal type generally has a good response to topical therapy, -Whereas skin with mainly dermal deposition of Alternative therapies such as chemical peeling agents or laser therapy are sometimes also used. Hydroquinone: Mechanism of action: HQ (1,4-dihydroxybenzene) is a hydroxyphenol, which, in the presence of catalytic amounts of dopa, will compete with tyrosine, the natural substrate of tyrosinase. This process prevents the enzymatic oxidation of tyrosine to dopa, thus, preventing the synthesis of melanin. This is consistent with the selective mode of action toward cells with active tyrosinase activity. HQ 3-5% concentration was determined to be the optimal strength. Interestingly, their impression from clinical observations was that many of the side effects experienced may occur from misuse, excessive use, and the application of multiple preparations. It has also been suggested that patients may use unsuitable cleansing agents, carry out vigorous rubbing of the affected areas, and apply excessive amounts of medication. Tri-Luma Cream: HQ 4% +fluocinolone 0.01% + tretinoin 0.05% Westerhof formula: HQ 2% + N-acetyl cysteine 3% + hydrocortisone 1% . - In 8 weeks: 77% improved the melasma HQ 4% + tretinoin 0.1% + lactic acid 7% in aqueous gel Kligman formula: HQ + tretinoin + dexamethasone Ochronosis: Erythema & pigmentation due to HQ Colloid milium Tretinoin: Mechanism of action (5) Retinoids, such as vitamin A acid and retinoic acid (RA) or tretinoin, were first used in combination with HQ to 1) enhance the penetration of HQ, but were later recognized to have their own effect on the pigment. 2)Tretinoin's ability to depigment is based on its ability 3)to disperse keratinocyte pigment granules, interfere with pigment transfer, 4)and accelerate epidermal turnover and, therefore, pigment loss. 5) In addition, there is also evidence that it can inhibit the induction of tyrosinase, DOPAchrome conversion factor, and melanogenesis Tretinoin is available in 3 forms: gel, cream, and liquid, at strengths ranging from 0.01% to 0.1% and is approved for the treatment of acne vulgaris and photoaging. As a monotherapy it is not an approved treatment for melasma; however, it is part of a combination HQ, tretinoin, and fluocinolone acetonide cream (TriLuma) which is an approved treatment for melasma. Safety and tolerability: The most common side effects of tretinoin include a retinoid dermatitis characterized by burning or stinging, erythema, scaling, and dry skin. inflammation may cause hyperpigmentation, especially in those with dark skin. Fortunately, most adverse effects (AEs) are reversible on discontinuation of therapy, although the hyperpigmentation/hypopigmentation may persist for many months. Topical tretinoin is not considered mutagenic or carcinogenic, however, animal tests have demonstrated evidence for teratogenicity. There have not been adequate and well-controlled studies performed in pregnant women.(category C) In addition, the safety of tretinoin gel has not been established in children younger than 12 years, neither has the safety of the emollient cream in patients younger than 18 years. Corticosteroids: Mechanism of action(4) Corticosteroids may directly affect the synthesis of melanin, although the mechanism by which the skin is lightened is 1) not completely known. 2) Melanocytes respond to a variety of chemical mediators such as prostaglandins and leukotrienes and, thus, it has been theorized that steroids might alter melanocyte function by inhibition of prostaglandin or cytokine production by various cells of the epidermis. 3) Corticosteroids may suppress secretory metabolic products from melanocytes without causing their destruction, and this could be the reason for their short-lived effect on pigmentation disorders. 4)Topical steroids also inhibit tyrosinase activity & affect endoplasmic reticulum secretory function of melanocytes. Efficacy: The use of corticosteroids in the treatment of melasma is seen more often in conjunction with other topical therapies (eg, tretinoin and HQ). As a monotherapy there has been little published research Unfortunately, the study failed to assess whether the improvement caused by steroid treatment was a longterm benefit. Azelaic acid A.A is a naturally occurring dicarboxilic acid derived from P.ovale. It inhibits mitochondrial oxidoreductase activation & DNA synthesis, as well as tyrosinase. Minimal effect on normal pig. and greatest effect on heavily pigmented melanocytes. …Azelaic acid: Useful in facial lentigo maligna (specificity for abnormal melanocytes), rosacea, solar keratosis, PIP due to herpes or burns. Effect comparable with HQ, 15-20% twice daily for 3-12 months, effective in dark skin Side effects: erythema, irritation Azelaic acid: Mechanism of action: Az.A has anti-inflammatory, antibacterial, and antikeratinizing effects, which make it useful in a variety of dermatologic conditions., acts on hyperactive and abnormal melanocytes by competitively inhibiting tyrosinase. Safety and tolerability: Topical administration of 20% Az.A has produced pruritus, burning, stinging, and tingling in 1% to 5% of patients. Other adverse reactions, such as erythema, dryness, rash, peeling, irritation, dermatitis, and contact dermatitis, have been reported in less than 1% of patients. Rarely asthma, vitiligo, small depigmented spots, hypertrichosis, development of keratosis pilaris, and exacerbation of recurrent herpes labialis may occur. Kojic acid: 5-hydroxymethyl-4H-pyrane-4-one is a hydrophylic fungal derivative obtained from Aspergillus & penicillium species. Some studies indicate kojic acid = HQ in skinlightening ability. The activity of kojic acid: prevent tyrosinase activity by binding to copper. Other topical agents Kojic acid is not an approved treatment for melasma. However, because both kojic acid and HQ are tyrosinase inhibitors, the combination should be expected to augment efficacy. Thus, those who do not respond to HQ and GA may benefit from the addition of kojic acid to the treatment regimen Licorice extract (glabridin): The principal active compound of licorice root extract is glabridin : 10-40% in skin lightening Depigmenting effect: 16 times greater than HQ It is faster acting: after 7 days 0.4% licorice extract + 0.05% betamethasone + 0.05% retinoic acid = 70% of patient reported excellent effects. Licorice extracts are used as topical anti-inflammatory agents to decrease skin redness & hyperpig. ..Licorice extracts: The active agents are known as liquiritin & isoliquiritin, which are glycosides containing flavonoids. Liquiritin induced skin lightening by dispersing melanin. Ascorbic acid Vit C interrupts the production of melanogenesis by interacting with copper ions to reduce dopaquinone & blocking dihydrochinindol-2carboxyl acid oxidation. Vit C, an antioxidant, is rapidly oxidized when exposed to air and is of limited stability. High concentrations of Vit C must be used with caution, as the low pH can be irritating to the skin. Cream 10% magnesium L-ascorbic acid-2phosphate (MAP), a stable derivative of vit C=lighten pig. L-ascorbic-2-phosphate (magnesium-L-ascorbyl-2- phosphate; VC-PMG) is a stable vitamin C derivative that suppresses melanin production. Applying VC-PMG cream 10% twice daily to the skin of 34 patients produced an improvement in 55% of those treated, suggesting that it may be effective in reducing hyperpigmentation Arbutin: Arbutin (HQ-BETA-D- glucopyranoside) and methyl-arbutin are skin-lightening glycosides found in bearberry, a fruit enjoyed by bears but not by humans. Arbutin is also present in certain herbs & pear tree Inhibiting melanosomal tyrosinase activity. A dose-dependent reduction in tyrosinase activity & melanin content in melanocytes. Arbitin is nontoxic to melanocytes Efficacy is less than kojic acid 3% is also applied. Higher concentrations=more effective but paradoxically skin darkening may occur. Glycolic acid: AHAs in low concentrations =rapid desquamation of pigmented keratinocytes. High= epidermolysis 30-70%, removal of superficial layers of epidermis, can enhance the penetration of other topical skin lighteners, such as HQ. Aloesin: Aloesin is a natural derevative of aloe vera that inhibits tyrosinase at noncytotoxic concentrations. In contrast to HQ, it shows no cell cytotoxicity; however, its ability to penetrate the skin is limited by its hydrophilic nature. Mixed with arbutin =enhance its skin-lightening ability Aloesin is an experimental products. Mequinol(4-Hydroxyanisol): 5-20% for treatment of solar lentigines. Mequinol is a substrate to the enzyme tyrosinase and acts as a competitive inhibitor of melanogenesis. Mequinol 2% + retinoic acid 0.01% , LASER + mequinol, reduced cessation of LASER therapy, as well as prevent recurrences. In dark skin : prevent the postprocedural PIP Niacinamide: Niacinamide, the amide form of Vit B3, inhibits the transfer of melanosomes to the epidermal keratinocytes. 3.5% niacinamide + retinyl palmitate useful in melasma Chemical peels: The mechanism of action of chemical peeling agents is the removal of melanin, rather than the inhibition of melanocytes or melanogenesis. Peels are usually well tolerated by individuals with lighter complexion; The risk of complications from chemical peels increases proportionately with the depth of the wound. Superficial peels carry the lowest risk of adverse reactions, but have still been associated with hyperpigmentation. Common adverse reactions to all types and depths of peel are persistent postpeel erythema, and the possibility of infection. a, b. Malar melasma before and after combined peeling with 25% salicylic acid and 10% TCA gel Conclusions: Melasma may be treated using monotherapy or with combination therapy. HQ is a reliable treatment and MKF is also effective. These therapies, coupled with regular application of a UVA and UVB blocking sunscreen to avoid UVinduced recurrence, are the most common therapies for epidermal melasma. AzA, currently only used as an off-label treatment, has also shown notable efficacy. Alternative treatments to topical include chemical peels, laser treatment, and dermabrasion. The GA peel seems to have the most promise as an alternative to bleaching creams. Laser treatments seem to show limited efficacy, although in many cases the number of participants with melasma in the studies are very small. IPL has also shown potential, however, combining topical agents such as HQ, tretinoin, and a corticosteroid, in addition to patient education, sun avoidance, and regular sunscreen use is the mainstay of treatment in this difficult and frustrating condition. :لیزر در ضایعات پیگمانته 1) Highly selective Q-switch lasers 2) Less pigmented selective, longer pulsed laser 3) Non-pigment specific ablative lasers - highly: Q-switched frequency doubled Nd-YAG( 532 nm), Q-S ruby (694 nm), Q-S alexandrite (755 nm), Q-S NdYAG (1064) 532 nm: epidermal pigment 694 & 755 nm: epidermal & dermal pigment 1064 nm: dermal pigment موفق باشید دکتر شاهمرادی