Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
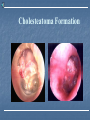
Acute otitis media and mastoiditis Chunfu Dai M.D & Ph.D Otolaryngology Department Fudan Univeristy Definition AOM: is an infectious process of the middle ear cleft and to a variable extent, of the mastoid air cell system. Bacteriology Streptococcus pneumoniae (48%) Haemophilus influenzae (31%) Moraxella catarrhalis (20%) P-hemolytic streptococcus (decreased following widespread immunization program) Pseudomonas aeruginosa (uncommon cause of AOM) 阻断细菌耐药性的“恶性循环” 感染 合理 治疗 不合理 治疗 耐药性 增加 传播 细菌 未消除 选择 耐药菌 临床 治愈 细 菌 消 除 青霉素耐药的肺炎链球菌 79-98年在美国流行情况 40 33% 中度敏感 (0.12 - 1.0 µg/ml) 耐药 ( 2.0 µg/ml) 30 29% 20 18% 10 (Doern. Am J Med. 1995;99(6B): 3S-7S; Jacobs et al., AAC 1999:43:1901; Jacobs et al abstract C-61, ICAAC 1999) 1998 1997 1994-95 1992-93 1990-91 1988-89 1987 1986 1985 1984 1983 1982 1981 1980 0 16% 1979 % Penicillin Resistance 50 Routine of infection Via eustachian tube upper respiratory infection (acute rhinonitis and nasal pharyngitis) Upper respiratory communicative disease (diaphea, mealse, et al) Swimming and dive in unclear water Anatomic contribution (Eustachian tube in infant is wide and short and the two orifice in the same level) Routine of infection Via external acoustic canal and TM Perforation Myringotomy or myrigotosis Via blood supply Pathology Mucosal inflammation Serous, hemorrhagic, or purulent exudate in middle cavity Rupture of tympanic membrane Symptoms Fever Otalgia It may be masked by analgesics or antibiotic 60% patients can spontaneous remission Fullness Hearing loss Physical findings Increased vascularization of the TM, initially located in pars of flaccida, frequently spreading beyond the annulus to the skin of the external canal. Bony landmarks are visible. Cholesteatoma Formation Physical findings Rapid middle ear exudation occurs, Blurring of the mallwall short process, followed by edema and bulging of the pars flaccida. Physical findings The progression of this disease may result in rupture of TM, releasing the middle ear contents (beating sign) leads to relief of otalgia and retraction of the pars flaccida Lab tests Blood counts usually shows leukocytosis with polymorphonuclear elevation. CT and MRI is necessary only for the rare patients with a serious complication (meningitis or brain abscess) Hearing tests Conductive hearing loss Degree of hearing loss will depend on the amount and viscosity of the middle ear exudate, TM edema It vary from 10-50 dB with predominant involvement of the low frequencies Hearing loss may mixed when there is labyrinthine extension. Managements Antibiotic therapy Experiences Antibiotic sensitivity and bacteriologic culture Traditional duration 10-14 d Currently duration 5-7 d Managements Nasal decongestants Best rest, light diet Avoidance of irritants (smoking) Managements Pre-perforation Pain relief drugs Surgery: myringotomy Progression with a red, bulging TM, severe otalgia and fever Otitis media with impending complications perforation is not big enough to drain all pus Managements Post-proferation: Clear-up pus with 3% hydro-oxygen Antibiotic ear drops With pus decreased and inflammation disappeared, alcohol can be used to facilitate dry ear. Follow-up Adequately treated AOM effusion may persist for 2-6 weeks or even longer. Managements may require extended antibiotic treatment Otoscope and audiometric tests should be performed 3-4 weeks following apparent resolution of the acute infection Insertion of pressure equalization tubes due to fluid persists beyond 3 months Acute mastoiditis Definition: an infection of the mastoid characterized by diffuse osteitis followed by rarefaction and breakdown of the bony septae. Acute coalescent mastoiditis Haemorrhagic mastoiditis Masked mastoiditis Predisposition to pneumatic mastoid Predilection to kid Mastoid is mature at age of 4 year old Acute mastoiditis Reduction of immune system Strong bacteria (type III pneumococus, haemolytic streptococcus) Obstruction- not effective drainage Imcompletely treatment Acute mastoiditis Symptoms Symptoms may follow AOM, with or without a symptom-free interval of a few days to several weeks or more. Otalgia Aural discharge Conductive hearing loss fever Acute mastoiditis Physical findings Fever, from a slight elevation to 39 Otorrhea may be absent Pulsatile may be observed Tympanic perforation is present, but it may be obscured by intense edema Swelling of the superior TM and posterosuperior wall of EAC Postauricular area erythema and tenderness Pitting edema Obliteration of the postauricular crease Acute mastoiditis Radiographic evaluation Diffuse rarefaction of bone and breakdown of cellular sepae Acute mastoiditis interventions Medical management Antibiotic Intravenous antibiotic therapy should be maintained for at least 24-48 h after the resolution of symptoms Then followed with oral antibiotic for 2 weeks Surgical management Emergency surgery: simple mastoidectomy Mastoidectomy + ventilation tube placement