Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
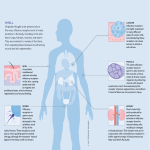
Lecture 1, 2 Autonomic Pharmacology • Explain the function and mechanism of action of all elements of the ANS • Define the roles of cholinergic receptors, their differences, and systemic responses • Differentiate between the actions of muscarinic, nicotinic and adrenergic receptors and their subtypes • Identify and explain the mechanism of action for pharmacologic agents used to manipulate these systems, and their role in pharmacotherapy • Define the pharmacologic rationale for therapeutic application of autonomic-acting agents • Given a generic drug name, define mechanism of action, side effects, and therapeutic utility Peripheral Nervous System Autonomic NS • Regulates activity of: – Smooth muscles – Exocrine glands • Some endocrine glands – Cardiac tissue – Metabolic activities • Involuntary • Regulated by brain stem centers Somatic NS • Activates skeletal muscle contraction • Voluntary body movements • Regulated by corticospinal tracts & spinal reflexes Side note: exocrine- section into external environment through ducts, e.g. (sweat, oil, wax, enzymes, etc.); endocrine- secretion into internal environment with no ducts and hormones are secreted Preganglionic autonomic neurons and somatic neurons are myelinated Ach N- ANS preganglionic + somaticNS Ach M- ParaNS postganglionic + SymNS sweat glands **Exception Adrenergic- SymNS postganglionic Concept: ganglia use Ach/neuronal tissue The adrenal medulla has Ach receptors and acts like a neuronal ganglia. It releases NE (80%) and Epi (20%) **Epi is only made by the adrenal medulla by SNS Enteric Nervous System - part of the PNS • Meshwork of fibers innervating the GI tract • Controls GI motility and secretion • Has – Independent control! – And highly regulated by the autonomic nervous system – And higher levels of the CNS • “Brain of the Gut” Autonomic Nervous System • Sympathetic NS – Nerves arise from the thoracic and lumbar spinal cord – Short preganglionic fibers & long postganglionic fibers • Parasympathetic NS – Portions of cranial nerves III (oculomotor), VII (facial), IX (glossopharyngeal) and X (vagus) all are both sensory and motor except CNIII which is just motor – Long preganglionic fibers and short postganglionic fibers EPSP- Na+ influx- Nicotinics is Na+ channel faster IPSP- K+ efflux, Cl- influx Muscarinic Receptors Regulate (slow IPSP/EPSP)- 2nd messengers regulate K+ or Clchannels and are slower Ganglia Phenomenon: have both receptors and Ach can act on both– Nicotinic causes EPSP. When Ach binds to muscarinic they regulate the EPSP and these can be slow IPSP or EPSP regulated by M1 receptors . Neurotransmission • 7 Steps of Synaptic Transmission **all drug targets – – – – – – – Synthesis and storage Action potential and depolarization Activation of voltage-dependent Ca2+ channels Vesicle fusion and release Receptor binding Signal termination in the synaptic cleft Termination of postsynaptic intracellular signaling There are also autoreceptors that determine how the cell will release the NT in presynaptic cellusually inhibitory Synthesis-storage-inactivation of ACh After the release of ACh and its interaction with its receptors, it is hydrolyzed by acetylcholinesterase (AChE) to acetate and choline; the latter is taken back up into the nerve terminal and is reused for ACh synthesis. The acetyl CoA was donated by the Mitochondria. Choline +AcetylCoA become Ach via acetylcholine transferase. There are massive amounts of Mito at the terminal. Synthesis, Storage and Inactivation of NE The action of NE is terminated by neuronal reuptake into the nerve terminal NE may be inactivated by monoamine oxidase (MAO) w/i the nerve terminal or catechol-Omethyltransferase (COMT) extraneuronally MOA The rate limiting step is Tyr DOPA via tryosine hydroxylase COMT is also in the brain and glial cells but is extraneuronal COMT You can’t give NE in mouth and it must be peripheral b/c it will break down if given orally. Receptors Acetylcholine receptors muscarinic or nicotinic (none to blood vessels except certain glands**) • Muscarinic – parasympathetic neuroeffector junctions (G-protein coupled, metabotropic) – Sweat glands use M2, M3 receptors – Odds are G (alphaq, get constriction in smooth muscles) and evens are G (i, inhibit adenylate cyclase and get constriction) – M2- heart, respiratory, brain, inhibition of NE (heteroreceptor) and Ach (autoreceptor) – M3- eye, stomach (sphincter relaxation, secretion stimulation), bronchoconstriction, vasodilation, emesis, GI (sphincter relaxation, increase sectretion), urinary bladder, pancreas secretion, salivary gland blood vessels, these increase the blood to the gland to get increase in section and this is ONLY area where blood vessels have PARA that cause vasodilation!!! • Nicotinic – all autonomic ganglia, somatic neuromuscular junctions & brain [+sympathetic in the adrenal medulla] Adrenoceptors α and β • • • • • α1: contraction of vascular smooth muscle (vasoconstriction), the iris dilator muscle (mydriasis), and urinary tract smooth muscle, increased peripheral resistance – Found in vascular smooth muscle, Also found in exocrine glands and the CNS α2: mediate smooth muscle relaxation by feedback inhibition of norepinephrine and Ach release from nerve terminals [decrease outflow of NE] (ex. nasal decongestants work on this in the nose to constrict), prejunctional , inhibit insulin release – Also found in platelets and the pancreas β1: cardiac stimulation positive chronotropic ( HR), ionotropic ( contractility) & dromotropic ( conduction velocity) effects, increase in lipolysis – Found in the heart; Activation also increases renin secretion in the kidney β2: mediate relaxation of bronchial (use these for asthma patients), uterine and vascular smooth muscle (vasodilation) – Skeletal muscle: mediate K+ uptake – Liver: mediate glycogenolysis (increase in muscle and liver, increase blood sugar) β3: enhances lipolysis N.E.D mnemonic for catecholamines: norepinephrine, epinephrine, dopamine Adrenoceptors α and β Domamine receptors • D1: mediate relaxation in vascular smooth muscle • D2: modulate neurotransmitter release • Imidazoline receptors: natriuresis (eliminating Na+ in urine causes diuresis and water to follow Na+) and decrease in sympathetic outflow from the CNS (used for the eye and to regulate the enteric NS) these decrease sympathetics “Rest and Digest” Slows heart rate Promotes digestion, defecation, & micTurition CNX- not sure of Para functin in the kidney so consider it null; visceral organs, parotid CNIII- ciliary m. and lacrimal gland CN VII, IX- to salivary gland, sublingual and submandibular gland “Fight or Flight” Cardiovascular stimulation Skeletal muscle activation Glycogenolysis Lipolysis How DO I Remember All of This Remember the parasympathetic • DUMBBELLS – – – – – – – – – Diarrhea Urination Miosis Bradycardia Bronchoconstriction, Bronchospasm Erection (Excite skeletal muscle, Emesis) Lacrimation Lethargy Salivation and Sweating The Baroreceptor Reflex Brody’s Human Pharmacology 5th ed. Storage and Release of Acetylcholine • 1. 2. 3. 4. 5. 6. 7. Drugs acting at each step of Synaptic Transmission Hemicholinium- block choline uptake Tetrodotoxin- blocking AP Na+ channels α-Latrotoxin*- form pores in lipid membranes induce Ca2+ inflow (from black widow spider) Botulinium toxin- - blocks synaptobrevin preventing vesicle fusion Atropine- muscarinic receptor antagonist Physostigmine- ACHE inhibitor Dantrolene- blocks ryanodine receptor which are major mediators of intracellular Ca2+ release • Do Hemicholinium and Vesamicol have a Clinical Use? • No, because they are nonselective cholinergic antagonist causing complete depletion and inactivation of all cholinergic systems. Nicotinic Receptor Agonists • Nicotine – prototype • Activates sympathetic (vascular system) & parasympathetic ganglia (GI tract) • blood pressure & heart rate • Diarrhea & urination • Crosses BBB alertness, vomiting, tremors, convulsions and coma Nicotinic Receptor Agonists • Varenicline (Chantix) – partial agonist in the brain • Indicated for smoking cessation • Reduces craving and withdrawal effects BUT • Associated with suicidal ideation, depression, changes in behavior Muscarinic Receptor Agonists • • • • • • • • • M1 - M5 Activate parasympathetic nerves Constriction of iris (miosis) Contraction of ciliary muscle Constriction of airways Increase in GI motility Contraction of bladder and relaxation of its outlet Decrease in heart rate Increased secretions (sweat, saliva, lacrimal, etc.) Muscarinic Receptor Agonists Bethanecol (Urecholine) • Stimulates bladder and GI w/o affecting HR or BP • Indicated for postoperative ileus, urinary retention Pilocarpine • Lowers intraocular pressure by increasing outflow of aqueous humor (glaucoma) • Stimulates salivary gland secretion (xerostomia) Cevimeline (Evoxac) • Stimulates salivary gland secretion (xerostomia) • Indicated in patients with Sjögren's syndrome • Side effects – extension of the parasympathomimetic actions • If given in high doses or parenterally, acute circulatory failure & cardiac arrest • CI: asthma, COPD, PUD ‘Shrooms Amanita muscaria • Mushrooms - Inocybe and Clitocybe contain muscarine • Diarrhea, sweating, salivation and lacrimation • No current medicinal use • Edibility: Toxic Clitocybe dealbata Clitocybe rivulosa Inocybe erubescens Heterotrimeric G proteins involved in the regulation of smooth muscle tone. Gq/G11-coupled receptors increase the intracellular Ca2+ concentration, leading to Ca2+/calmodulin (CaM)-dependent MLCK activation and MLC20 phosphorylation. Especially G12/G13coupled receptors mediate RhoA activation, thereby contributing to Ca2+-independent smooth muscle contraction. Relaxation is induced by activation of Gscoupled receptors, but the mechanisms underlying cAMP-mediated relaxation are not clear. Gi-mediated signaling might contribute to contraction by inhibiting Gs-mediated relaxation. cGKI, cGMP-dependent protein kinase I; DAG, diacylglycerol; IP3, inositol 1,4,5-trisphosphate; MLC20, regulatory chain of myosin II; MLCK, myosin light-chain kinase; MPP, myosin phosphatase; PIP2, phosphatidylinositol 4,5bisphosphate; PKA, cAMP-dependent kinase; PLC-β, phospholipase C-β; RhoGEF, Rho specific guanine nucleotide exchange factor; ROCK, Rho kinase; TRP, transient receptor potential channel. Acetylcholinesterase (AChE) • Removes ACh from the synapse by degradation to choline + acetate • Terminates neurotransmission at cholinergic synapses • Time required is less than 1 millisecond Cholinesterase Inhibitors Reversible – short-acting • Noncovalent – bind to the anionic domain of AChE, rapid hydrolysis • Covalent – also bind to AChE, but form a carbamoylated enzyme that undergoes slow hydrolysis • Edrophonium – used in diagnosis of myasthenia gravis • Neo- and pyridostigmine – myasthenia gravis, reversal of neuromuscular blockade, postoperative urinary retention • Physostigmine - glaucoma • Donepezil, galantamine, rivastigmine – Alzheimer’s disease Myasthenia Gravis – “Grave muscle weakness” Autoimmune disease • Autoantibodies against the nicotinic cholinergic receptor at the NM junction reduced numbers of receptors skeletal muscle weakness • Symptoms: drooping of one or both eyelids (ptosis), double vision (diplopia); altered speech, difficulty swallowing, problems chewing, loss of facial expressions • Muscle weakness increases during activity and improves after rest Myasthenia Gravis: Diagnosis • AChE inhibitors amplify the • Rapid but brief effects of ACh, temporarily improvement in strength restoring muscle strength after IV administration • Edrophonium – blocks ACh • Fasciculation (muscle hydrolysis twitch) generally occurs if NOT Myasthenia • Also used in myasthenic crisis Myasthenia Gravis: Treatment • Pyridostigmine (Mestinon) taken orally every day • Dose may vary on day to day basis (stress, infection, etc.) • Immune suppressants given concomitantly (corticosteroids) • AEs: abdominal cramping, diarrhea Cholinesterase Inhibitors Irreversible – long-acting • Phosphorylate AChE – strong bond, very slow hydrolysis • Organophosphates – pesticides and nerve gases • Highly lipid-soluble and absorbed from skin, mucous membranes and gut • Activate both muscarinic and nicotinic receptors Therapeutic uses • Echothiophate - glaucoma • Malathion (Ovide) – pediculosis capitis; kills ova and adult lice Organophosphate Poisoning • Toxic nerve gases – sarin, soman, tabun and VX • Insecticides – parathion and malathion • Agriculture major source of intoxications • Time to death - 5 min to 24 h if untreated, depending on route of exposure Symptoms • Initial - miosis, salivation, sweating, bronchoconstriction, vomiting, diarrhea • CNS – cognitive disturbance, seizure, coma • Neuromuscular blockade Treatment: 1) supportive care (airway), 2) decontamination, 3) atropine (large doses), 4) benzodiazepines (for seizures), 5) pralidoxime [2-PAM] (regenerates ChE) Cholinergic Transmission Drugs that enhance cholinergic transmission: 1. Nicotinic receptor agonists, e.g., nicotine 2. Muscarinic receptor agonists, e.g., bethanechol 3. Cholinesterase inhibitor, e.g., physostigmine Drugs that inhibit cholinergic transmission: 4. Inhibitors of vesicular ACh transport , e.g., vesamicol 5. Inhibitors of exocytotic release, e.g., botulinum toxin 6. Nicotinic receptor antagonists 7. Muscarinic receptor antagonists (e.g., atropine) 8. Inhibitors of high-affinity choline transport, e.g., hemicholinium 9. Inhibitors of pyruvate dehydrogenase, e.g., bromopyruvate Nicotinic receptor antagonists • Ganglionic blocking drugs – block nicotinic receptors on postjunctional neurons in sympathetic and parasympathetic ganglia Effect depends on which is dominant: • Sympathetic – hypotension • Parasympathetic – dry mouth, blurred vision & urinary retention • Not used clinically Role of Cholinergic Receptors of the Autonomic Ganglia Copyright © 2012 McGraw Hill Medical PARASYMPATHETIC → SYMPATHETIC → Predominant Autonomic Tone and The Consequences of Autonomic Ganglionic Blockade SITE PREDOMINANT TONE EFFECT OF GANGLIONIC BLOCKADE Arterioles Sympathetic-adrenergic Vasodilation, hypotension Veins Sympathetic-adrenergic Dilation, peripheral pooling Heart Parasympathetic-ACh Tachycardia Iris Parasympathetic-ACh Mydriasis Ciliary Parasympathetic-ACh Cycloplegia GI Parasympathetic-ACh Reduced tone & secretions Urinary Parasympathetic-ACh Urinary retention Salivary Parasympathetic-ACh Xerostomia Sweat Sympathetic-ACh Anhidrosis Genital Sympathetic & Para- Decreased stimulation Hexamethonium Man He is a pink complexioned person, except when he has stood for a long time, when he may get pale and faint. His handshake is warm and dry. He is a placid and relaxed companion; for instance he may laugh, but he can’t cry because the tears cannot come. Your rudest story will not make him blush, and the most unpleasant circumstances will fail to make him pale. His socks and his collars stay very clean and sweet. He wears corsets and may, if you meet him out, be rather fidgety (corsets to compress his splanchnic vascular pool, fidgety to keep the venous return going from his legs). He dislikes speaking much unless helped with something to moisten his dry mouth and throat. He is long-sighted and easily blinded by bright light. The redness of his eyeballs may suggest irregular habits and in fact his head is rather weak. But he always behaves like a gentlemen and never belches or hiccups. He tends to get cold and keeps well wrapped up. But his health is good; he does not have chilblains and those diseases of modern civilization, hypertension and peptic ulcers, pass him by. He is thin because his appetite is modest; he never feels hunger pains and his stomach never rumbles. He gets rather constipated so his intake of liquid paraffin is high. As old age comes on he will suffer from retention of urine and impotence, but frequency, percipitancy, and strangury will not worry him. One is uncertain how he will end, but perhaps if he is not careful, by eating less and less and getting colder and colder, he will sink into a symptomless, hypoglycemic coma and die, as was proposed for the universe, a sort of entropy death. W. D. M. Paton, Pharm. Rev. 6, 59 (1954) Discussion and Questions? • Is hexamethonium used to treat anything? • No, however, trimethaphan and mecamylamine were the first anti-hypertensive agents ever used. They were developed and used during the 1950-1960. Today, trimethaphan can be used to treat aortic dissection, to lower blood pressure and block sympathetic response while mecamylamine is an orphan drug for Tourette’s syndrome • Is this how cigarettes work? Discussion and Questions? • Is hexamethonium used to treat anything? • Is this how cigarettes work? • Nicotine’s effects are a summation of its effects on sympathetic and parasympathetic systems. This includes autonomic ganglia stimulation followed by a depolarization block. It also effects sensory and chemo receptors including the CTZ causing vomiting. It has the same biphasic effect on epinephrine release from the adrenal medulla. It causes CNS stimulation primarily at prejunctional nerve terminals causing neurotransmitter release. This includes excitatory amino acids, leading to it’s stimulatory action, and dopamine which leads to the addiction and pleasure. Nicotinic Receptor Antagonists • Neuromuscular blocking drugs - bind to muscle nicotinic receptors and inhibit ACh neurotransmission at skeletal neuromuscular junctions muscle weakness and paralysis • Remember this for later Muscarinic Receptor Antagonists • Competitive antagonists: compete with ACh at parasympathetic neuroeffector junctions inhibit parasympathetic nerve stimulation • AKA parasympatholytics • Relax smooth muscle, increase heart rate, inhibit exocrine gland secretion • Generally not selective for different receptor subtypes Muscarinic Receptor Antagonists Belladonna alkaloids • Atropine • Hyoscyamine • Scopolamine Semisynthetic/synthetic agents • • • • • Dicyclomine Glycopyrrolate Ipratropium Oxybutynin etc… Case • A 16-year-old male was brought to the ER by friends after becoming highly agitated and experiencing visual hallucinations, claiming that one of his friends had a mailbox for a head • He ingested some seeds from plants growing in a vacant lot; denied EtOH or other substances • PE: Dry skin and mucous membranes, absent bowel sounds, sinus tachycardia, dilated pupils & blurred vision • Labs: WNL; EtOH - 0 Case • Gastric lavage was performed & activated charcoal was administered to remove any unabsorbed substances • The patient became more agitated and delusional • An infusion of physostigmine was administered x 2 • His symptoms began to subside and 12 hours later he was much improved • 36 hours later he was discharged with normal vital signs and mental status • The plant material was identified as Datura stramonium Anticholinergic Toxicity • Jimson weed or locoweed (Datura stramonium) • Hallucinogenic plant containing belladonna alkaloids found throughout the U.S. • Toxic via ingestion or inhalation • Fatalities have occurred Treatment • Remove drug (plant material) from GI tract • Supportive care • Cholinesterase inhibitor (physostigmine); ACh & counteracts central nervous system toxicity (hallucinations, seizures) Belladonna alkaloids • • • • Atropa belladonna (deadly nightshade) Datura stramonium (Jimson weed) Hyoscyamus niger Belladonna – “fair lady”, referred to pupil dilation produced by extracts of these plants; considered attractive during the Renaissance • Atropine – Hyoscyamine - Scopolamine Atropine/Scopolamine/Hyoscyamine • • • • Well absorbed Tertiary amines so distribute in to the CNS Excreted via urine; t1/2 ~ 2 hours Ocular t1/2 is longer; bind to iris pigmentation, pigments slowly release drug over days; darker irises bind more • Toxicity: Dry as a bone, blind as a bat, red as a beet and mad as a hatter Atropine/Scopolamine/Hyoscyamine Ocular: Mydriasis Cycloplegia Dry eyes Respiratory: Dilation secretions GI/Urinary: LES – reflux Motility Gastric acid secretion Urinary retention CNS: Sedation OR stimulation Delirium Cardiac: HR (standard dose) HR (low dose) Misc: Sweating hyperthermia Can’t see Can’t pee Can’t spit Can’t s*%t Atropine, et al: Indications Ocular: Mydriasis – ophthalmoscopic exam Cycloplegia – refractive errors of lens Iritis, cyclitis Cardiac: HR– sinus bradycardia (IV) Respiratory: Palliative care – decrease respiratory secretions CNS: Motion sickness (scopolamine) blocks ACh from vestibular to vomiting center Parkinson’s disease GI/Urinary: Motility – intestinal/urinary spasm & pain (hyoscyamine) Misc: SEs of myasthenia gravis treatment Reverse cholinesterase inhibitor overdose Semisynthetic/Synthetic Agents • Pharmacologic effects similar to atropine-like agents but pharmacokinetic profiles make them useful in specific situations • Ipratropium/tiotropium – administered via inhalation; few systemic side effects; COPD • Dicyclomine – symptoms of irritable bowel: intestinal cramping • Oxybutynin, darifenacin, solifenacin, fesoterodine, tolterodine, trospium – overactive bladder (frequency, nocturia, urgency, incontinence) Semisynthetic/Synthetic Agents • Glycopyrrolate – Preoperatively to inhibit secretions of salivary and respiratory tract – During anesthesia to inhibit secretory and vagal effects of cholinesterase inhibitors used to reverse neuromuscular blockade – Manage oral secretions in terminally ill patients • Tropicamide – mydriatic for eye exam; short duration of action (~ 1 hour) Muscarinic Receptor Antagonist Contraindications • Ophthalmic preps in elderly & • Urinary retention those with narrow angles – • Prostatic hypertrophy can trigger acute angle• Co-administration with closure glaucoma other anticholinergic • Bowel atony agents Ocular Effects of Muscarinic Drugs A: Relationship between the iris sphincter and ciliary muscle in the normal eye. B: Effects of pilocarpine, a muscarinic receptor agonist: pupillary constriction (miosis), contraction of the ciliary muscle, relaxation of the suspensory ligaments connected to the lens, increase in lens thickness. As the lens thickens, its refractive power increases so that it focuses on close objects. C: Effects of atropine, a muscarinic receptor antagonist: pupillary dilation (mydriasis), increased tension on suspensory ligaments, lens becomes thinner & focuses on distant objects. * *Do not penetrate BBB very well fewer CNS side effects Brody’s Human Pharmacology 5th ed. Review Questions • The major neurotransmitter in the parasympathetic nervous system is _________, while the major neurotransmitter in the sympathetic nervous system is ________. • Acetylcholine and norepinephrine • Norepinephrine and acetylcholine Review Questions • Reversible cholinesterase inhibitor • Malathion • Edrophonium • Irreversible cholinesterase inhibitor • Physostigmine • Donepezil • Echothiophate Review Questions • Which of the following are effects of muscarinic receptor activation? – Decrease in heart rate – Increase in heart rate – Decrease in GI motility – Secretion of hydrochloric acid – Bronchodilation Review Questions • A patient presents with confusion, blurred vision, dry mouth and constipation. These are symptoms of: – Anticholinergic toxicity – Cholinergic toxicity – Myasthenia gravis – Organophosphate poisoning Lecture 3, 4, 5 Autonomic Pharmacology • Explain the function and mechanism of action of all elements of the ANS • Define the roles of cholinergic and adrenergic receptors, their differences, and systemic responses • Differentiate between the actions of muscarinic, nicotinic and adrenergic receptors and their subtypes • Identify and explain the mechanism of action for pharmacological agents used to manipulate these systems, and their role in pharmacotherapy • Define the pharmacologic rationale for therapeutic application of autonomic-acting agents • Given a generic drug name, define mechanism of action, side effects, and therapeutic utility Noradrenergic transmission Drugs that enhance or mimic noradrenergic transmission (sympathomimetics): 1. Facilitate release, e.g., amphetamine 2. Block reuptake, e.g., cocaine 3. Receptor agonists, e.g., phenylephrine Drugs that reduce noradrenergic transmission (sympatholytics): 4. Inhibit synthesis, e.g., 4a, α-methyltyrosine; 4b, carbidopa; 4c, disulfiram 5. Disrupt vesicular transport and storage, e.g., reserpine 6. Inhibit release, e.g., guanethidine 7. Receptor antagonists, e.g., phentolamine 3 Classes of: Adrenoreceptor agonists • Direct-acting: bind to and activate the receptors – Catecholamines & noncatecholamines • Indirect-acting: increase the concentration of norepinephrine at neuroeffector junctions • Mixed-acting: direct & indirect actions Direct-acting agonists: Catecholamines Naturally occurring Synthetic • Norepinephrine • Epinephrine • Dopamine • Isoproterenol • Dobutamine Rapidly inactivated by monoamine oxidase (MAO) and catechol-O-methyltransferase (COMT) in the gut, liver, & other tissues Catecholamine basic structure must have –OH at 3 and 4 or lose activity Low bioavailability, short half-life = parenteral administration required Direct-acting agonists: Catecholamines • • • • • NE: α1= α2 , β1> β2 Activation of α1 receptors = vasoconstriction, peripheral resistance; systolic & diastolic blood pressure reflex bradycardia EPI: α1= α2 , β1= β2 – Low dose: β2 receptor stimulation = vasodilation, DBP; bronchodilation – High dose: α1 stimulation = vasoconstriction, SBP & DBP Isoproterenol: β1= β2 >>>α Activation of β1& β2 = cardiac stimulation & vasodilation; DBP but SBP by increasing heart rate & contractility; potent chronotropic effect may lead to tachycardia and tachyarrhythmias; bronchodilation Dopamine: D1> β1 >α – Low dose: D1 = renal vasodilation; – Mid dose: β1 = cardiac contractility, cardiac output, tissue perfusion; – High dose: α1 receptors = vasoconstriction Dobutamine: β1> β2 >α β1 = cardiac contractility, cardiac output; β2 = vasodilation, vascular resistance SBP = systolic blood pressure; DBP = diastolic blood pressure Mean Arterial Pressure • Perfusion pressure seen by organs in the body • Want MAP > 60 mmHg is enough to sustain the organs of the average person (70 to 110 mmHg) • If the MAP falls significantly below this number for an appreciable time, the end organ will not get enough blood flow, and will become ischemic • MAP = 1/3(SBP-DBP)+DBP Catecholamines: Indications Shock • Cardiogenic • Neurogenic & Septic • Anaphylactic • Cardiac arrest (Epi) • Bradycardia/AV block (Iso) • Prolongation of local anesthetic action (Epi) • Acute heart failure (Dobu) Note: Catecholamines that increase blood pressure are also called vasopressors Shock Profoundly decreased blood flow to vital organs • Hypovolemic: inadequate blood volume; tx by giving fluid saline • Cardiogenic: inadequate heart function; called cold shock • Neurogenic/septic: inadequate vasomotor tone – Septic: pathogenic microorganisms produce toxins causing massive vasodilation; called warm shock • Anaphylactic: severe immediate hypersensitivity reaction with hypotension and difficulty breathing Shock: General principles Fluid resuscitation if hypovolemic • Cardiogenic shock: 1) dobutamine, 2) dopamine • Neurogenic/septic shock: norepinephrine; often in combination with dopamine to preserve renal blood flow; goal MAP > 60 mm Hg • Anaphylactic shock: epinephrine Catecholamines: Adverse effects Excessive vasoconstriction • Tissue ischemia/necrosis • Reduction of blood flow to vital organs Excessive cardiac stimulation • Arrhythmias Glycogenolysis (β2) • Hyperglycemia Non-catecholamines Do not contain a catechol moiety Not substrates for COMT May be resistant to degradation by MAO Effective orally Longer duration of action Phenylephrine (the friend of the receptor) • Well absorbed orally and topically; may also be given IV • Partly metabolized by MAO in the liver and intestine • Activates α1 receptors Phenylephrine: Indications • Viral/allergic rhinitis: nasal decongestant • Allergic conjunctivitis: ocular decongestant • Mydriasis: ophthalmologic exam Hypotension/shock due to: • Excessive vasodilators • Drug-induced • Septic shock • Neurogenic shock • Maintenance of BP during surgery (anesthesiainduced hypotension) Midodrine • Rapidly absorbed after oral administration • Metabolized in the liver/tissues to active metabolite (desglymidodrine) • Activates α1 receptors = vasoconstriction, SBP & DBP while standing, sitting & supine • Indicated to treat postural (orthostatic) hypotension when non-pharmacologic treatment fails • AE: Hypertension, especially when supine β2 agonists • Selective β2 agonists, however, at higher doses may stimulate β1 receptors as well • Bioavailability 30-50% (incomplete absorption, 1st-pass metabolism) • Metabolized to inactive compounds; renally excreted • PO, IV or via inhalation β2 agonists: Indications • β2: relaxation of bronchial, uterine and vascular smooth muscle • Obstructive lung disease: asthma, COPD • Premature labor • AEs: tachycardia, skeletal muscle tremor, nervousness • • • • • • • Albuterol Metaproterenol Salmeterol Formoterol Bitolterol Ritodrine Terbutaline- relaxes uterine muscles More on these in the Cardio-Pulmonary Block! Imidazolines • α1 receptor activation: oxymetazoline (non-selective αadrenergic agonist) – Nasal & ocular decongestant • α2 receptor activation: apraclonidine, brimonidine – intraocular pressure with ocular surgery –”onidines” • α2- & imidazoline- receptor activation in the CNS – Clonidine – hypertension – Dexmedetomidine – sedation during mechanical ventilation Clonidine • α 2-receptor agonist in the CNS (medulla) reduced sympathetic outflow • peripheral resistance, heart rate, and cardiac output = BP • AEs: dry mouth, sedation, dizziness • Abrupt withdrawal = sympathetic NS over activity (HTN, tachycardia & sweating); “rebound HTN” • Guanabenz & guanfacine Indirect acting agonists Amphetamine Cocaine • Inhibits the storage of norepi by • Blocks neuronal uptake of neuronal vesicles reverse norepi at central and transport back into the synapse peripheral synapses stimulates the sympathetic NS • Highly lipid soluble • Vasoconstriction, pupillary • Increases norepi in the CNS & dilation, cardiac stimulation, peripherally BP and CNS stimulation • Vasoconstriction, cardiac cardiac damage/heart failure stimulation, BP and CNS • Local anesthetic stimulation Mixed-acting agonists Ephedrine & pseudoephedrine (isomer) • Activate α1 receptors vasoconstriction (nasal decongestants), BP & urinary retention • Activate β1 receptors tachycardia • Activate β2 receptors bronchodilation • CNS stimulation insomnia Mixed-acting agonists • Ephedrine derived from a naturally occurring plant, Ephedra, AKA Ma Huang • Well absorbed, lipid soluble • Relatively resistant to MAO and COMT metabolism = long duration of action • Found in dietary supplements until banned by the FDA due to deaths caused by hypertension and cardiac stimulation Adrenoreceptor antagonists Reduce sympathetic stimulation; sympatholytics Therapeutic effects • Blocking α1 receptors = vascular & smooth muscle relaxation • Blocking β1 receptors = reduces sympathetic stimulation of the heart Adverse effects • Blocking α2 receptors = dizziness, headache, nasal congestion • Blocking β2 receptors = bronchoconstriction, inhibits glycogenolysis Selective α1- antagonists • Vasodilation, BP; relax the bladder, urethra and prostatic smooth muscle • Indications – it is an o-sin to block alpha1 – Hypertension (doxazosin, prazosin & terazosin) – Urinary symptoms (frequency, urgency & nocturia) due to benign prostatic hypertrophy (alfuzosin, tamsulosin) • AEs: hypotension, dizziness, sedation Selective α1- antagonists • Prazosin – duration of action ~ 6 hours; first-pass metabolism; renal/biliary excretion • Doxazosin – duration of action ~ 30 hours • Terazosin – duration of action ~ 20 hours • Although indicated in the treatment of HTN, not firstline • AE: Orthostatic hypotension • Alfuzosin/tamsulosin – “uroselective” • Relieve lower urinary tract symptoms without as much hypotension, dizziness & sedation Nonselective α-adrenergic antagonists Phenoxybenzamine • Spontaneous chemical transformation to an active metabolite stable covalent bond with the α receptor noncompetitive antagonism of epinephrine & other adrenergic agonists • Gradual onset, duration ~ 3-4 days • Vascular resistance, BP • Indication: hypertension in pheochromocytoma until surgery Phentolamine • • • • • • Imidazoline Competitive antagonist Onset immediate (IV), duration 1015 min Hepatic metabolism, renal excretion Vascular resistance, BP Indications: hypertension caused by α1-agonists; dermal necrosis & ischemia caused by extravasation of epinephrine. Perioperative use for patients with pheochromocytoma. Selective α2-blockers • Yohimbine (Yocon) • • • • • Competitive antagonist, α2 selective Bark of Pausinystalia yohimbe Enters CNS – BP, HR, motor activity Actions appear opposite that of clonidine Used (herbal treatment) for male sexual dysfunction • Neuroleptic Agents • Dopamine (D2) receptor antagonists • Chlorpromazine, haloperidol, phenothiazines • Induce side effects via blockade of α2 • • • • • • • Selective β1 - antagonists β 1 > β2 Primarily located in cardiac tissue β1-blockers AKA cardioselective β-blockers However, as dose increases, β2 receptor blockade increases Negative chronotropic, ionotropic and dromotropic effects Decrease cardiac output and BP Decrease aqueous humor secretion in the eye and intraocular pressure Drug Lipid solubility Bioavailability Half-life Indications Acebutolol Medium 40% 10-12 h HTN Arrhythmias Atenolol Low 50% 6-7 h HTN, acute MI, angina Adverse effects Bronchoconstriction Betaxolol Low 90% 14-22 h HTN, HF, Glaucoma Fatigue Bisoprolol Low 80% 9-12 h HTN, HF Depression Esmolol Low 100% (IV) 10 min Acute SVT Bradycardia Metoprolol Medium 40% 3-4 h HTN, HF, angina, MI Sexual dysfunction Nonselective β - antagonists • Block β1-receptors in cardiac tissue and β2receptors in smooth muscle, liver, & other tissues • Intrinsic sympathomimetic activity • Membrane-stabilizing activity • Inhibit epinephrine-stimulated glycogenolysis • Mask signs of early hypoglycemia (sweating, tachycardia) Intrinsic sympathomimetic activity ISA • Partial agonist activity = smaller reduction in heart rate when the patient is resting and sympathetic tone is low • Pindolol (non-selective) and acebutolol (selective) Membrane-stabilizing activity • Local anesthetic activity • Block sodium channels cardiac nerves = slow conduction velocity, perhaps contributing to antiarrhythmic effects • Pindolol and propranolol (nonselective) Drug Lipid solubility Bioavailability Half-life Indications Adverse effects nadolol Low 35% 15-20 h HTN, angina, migraine HA prophylaxis Broncho- pindolol Medium 75% 3-4 h HTN constriction Fatigue Propranolol1st drug discovered timolol High Medium 25% 50% 4-6 h 4-6 h HTN, angina, essential tremor, migraine HA prophylaxis Depression Bradycardia Sexual HTN, migraine dysfunction HA prophylaxis, glaucoma α- and β-antagonists- go to the lab to carve out receptors lol Drug MOA F HalfLife Effects Indications Carvedilol β1 & β2-blocker; α1- blocker 30% 6-8 h Vasodilation, HR & BP, CO HTN Heart Failure Labetalol β1 & β2-blocker; α1- blocker 20% 6-8 h Vasodilation, HR & BP HTN Review questions • Activation of β1 receptors produces cardiac stimulation while activation of β2 receptors mediates smooth muscle relaxation. Review questions • Which of the following receptors are associated with renal vasodilation when activated? – α1 – β1 – D1 • Which catecholamine has this effect? dopamine Review questions • Catecholamine Z is injected. The patient’s BP and peripheral resistance rises; the HR decreases. Which catecholamine was given? – Dopamine – Epinephrine – Isoproterenol – Norepinephrine Review questions • A new patient of yours with episodic severe HTN is found to have markedly elevated levels of epinephrine and norepinephrine metabolites in his urine. What would you prescribe to lower his blood pressure before surgery? – Doxazosin – Metoprolol – Phenoxybenzamine – Tamsulosin Lecture 6 Neuromuscular Blocking Agents • Define the mechanism of action of neuromuscular blocking agents and know their indications • Relate pharmacokinetic parameters to drug selection • Convey information related to drug interactions and side effects • Explain the pharmacological rationale behind use of these drugs in clinical settings History • In the 16th century, European explorers found that South American natives in the Amazon basin were using an arrow poison, curare, to produce skeletal muscle paralysis in the animals they were hunting • Active compound – d-tubocurarine Nicotinic Receptors • • • • • N1 or NM and N2 or NN Ligand-gated ion channel Requires binding of two acetylcholine molecules Composed of five subunits (pentamer) Five different types of subunits – α, β, γ, δ and ε – 10 different α and 4 different β subunits • NM receptors contain only α1 and β1 subtypes plus δ and γ/ε • NN receptors contain α2-10 and β2-4 subtypes ε Neuromuscular blocking agents • Introduced in the 1940s • Structural analogs of acetylcholine (ACh) • MOA: Bind to the nicotinic acetylcholine receptor at the motor end plate and inhibit binding of ACh at skeletal neuromuscular junctions muscle weakness and paralysis • Do not cross the blood-brain barrier, thus a patient may be paralyzed but completely aware • Classified as either depolarizing or nondepolarizing Classification Depolarizing agents – Occupy and activate the nicotinic receptor for a prolonged period of time, leading to blockade: nicotinic receptor agonists • Structures resemble that of acetylcholine (ACh) Nondepolarizing agents • Competitively antagonize the actions of ACh at the nicotinic receptor • Majority of agents fall into this classification Peripheral Nerve Stimulator • Contraction of the adductor pollicis muscle • Determine – – – – Type Onset Magnitude Duration • ED95 – 95% suppression on a single twitch – Used to quantify the potency of a neuromuscular blocker Other pharmacologic actions • Stimulate the release of histamine bronchospasm & hypotension (tubocurarine, mivacurium and atracurium) • Block autonomic ganglia hypotension & tachycardia (tubocurarine) • Block cardiac muscarinic receptors tachycardia (pancuronium) Pharmacokinetics • Poor absorption from GI tract; only administered by intravenous route • Do not enter cells or cross blood-brain barrier; distribution volume is similar to blood volume • Eliminated in urine and bile primarily as unchanged compounds, some as hepatic metabolites • Atracurium & cisatracurium (a stereoisomer of atracurium) undergo spontaneous nonenzymatic degradation (Hofmann elimination); preferred for patients with impaired liver and kidney function Drug Histamine release Ganglionic blockade Onset of action (min) Duration of action (min) Elimination Succinylcholine*depola Minimal None 1.5 Short (5-10) Plasma cholinesterase Atracurium Varies Low 3 Intermediate (3060) Plasma esterase Cisatracurium None Low 3 Intermediate (3060) Spontaneous degradation Pancuronium None Medium 3 Long (60-120) Renal Rocuronium None Low 1 Intermediate (3060) Biliary/renal Tubocurarine High High 2 Long (60-120) Renal/biliary Vecuronium None Low 2 Intermediate (3060) Biliary/renal Hepatic metabolism rizing Succinylcholine • Persistent depolarization of the motor end plate due to lack of metabolism by Acetylcholinesterase (AChE) • Phase I block – initial muscle fasciculations over the chest and abdomen flaccid paralysis of eye and face muscles, arms, legs and neck muscles, then intercostal muscles and diaphragm • Phase II block – membrane repolarizes but is still unresponsive; desensitized nicotinic receptor • Recovery occurs in reverse order: diaphragm regains function first, followed by limb and trunk muscles, and lastly small muscles Succinylcholine MOA Phase I – depolarizing These effects cannot be reversed by cholinesterase inhibitors Phase II - desensitizing Succinylcholine: Adverse effects • Genetic variations in butyrylcholinesterase activity either 1) lower concentrations of the enzyme or 2) an abnormal enzyme resulting in a longer duration of activity and apnea • May cause increased intraocular pressure and intragastric pressure • Hyperkalemia ( K+) patients with burns, neuromuscular disease or nerve damage, closed head injury and other trauma may release potassium into the blood, rarely resulting in cardiac arrest Indications of NM Blockers • Endotracheal intubation • muscle contractility, decreasing the depth of anesthesia required for surgery • In patients on mechanical ventilation (ICU) to decrease O2 consumption and prevent high airway pressures if sedation alone is not enough • Prevent bone fractures during electroconvulsive therapy Drug interactions • Inhaled anesthetics potentiate neuromuscular blockade Isoflurane Sevoflurane Desflurane Enflurane Halothane Nitrous oxide Malignant hyperthermia: rare interaction with succinylcholine; abnormal release of calcium from skeletal muscle causes muscular contraction, rigidity and heat production; hyperthermia, metabolic acidosis, tachycardia • Dose must be reduced when used together Drug interactions Antibiotics potentiate neuromuscular blockade • Aminoglycosides (gentamicin, tobramycin) - Ach release; lower sensitivity to ACh • Tetracyclines – chelate Ca++ and Ach release • Clindamycin – block nicotinic receptors; depress muscle contractility • Dose must be reduced when used together Drug interactions Local anesthetics • Bupivacaine potentiates blockade by blocking neuromuscular transmission and muscle contractions • Lidocaine and procaine prolong the duration of action of succinylcholine by inhibiting butyrylcholinesterase Drug-disease considerations • Myasthenia gravis – resistance to succinylcholine but increased sensitivity to nondepolarizing agents; avoid long-acting agents • Advanced age – prolonged duration due to decreased clearance by the liver and kidneys • Hyperkalemia – potentiates depolarizing agents; antagonizes non-depolarizing agents • Hypokalemia – potentiates non-depolarizing agents; antagonizes depolarizing agents Drug-disease considerations • Renal disease – prolonged elimination of compounds that depend on glomerular filtration, tubular secretion and reabsorption for clearance • Hepatic disease – prolongs the duration of blockade Drug selection Considerations • Onset of action • Duration of action • Adverse effects (cardiovascular, respiratory) • Renal/hepatic function Reversal • Nondepolarizing agents can be reversed by cholinesterase inhibitors (neostigmine, physostigmine, pyridostigmine) Which of the following NMBs is the DOC for intubation due to its short onset of action? a. b. c. d. Pancuronium Vecuronium Succinylcholine Atracurium Which of the following NMBs would you avoid in a patient with renal insufficiency (ClCr ~ 25 mL/min)? a. b. c. d. Atracurium Cisatracurium Pancuronium Rocuronium Which of the following NMBs would you avoid in a patient with a history of malignant hyperthermia? a. b. c. d. e. Atracurium Cisatracurium Pancuronium Rocuronium Succinylcholine A 22-year-old patient underwent a surgical procedure. Anesthesia was provided by isoflurane, supplemented by intravenous midazolam (a benzodiazepine sedative) and pancuronium. Which of the following will reverse the effects of the pancuronium at the end of the procedure? What is its MOA? a. b. c. d. Aminoglycoside Bupivicaine Nitrous oxide Physostigmine Lecture 7 Skeletal Muscle Relaxants • Explain the mechanism of action of muscle relaxants • Describe indications and contraindications for this group of drugs • Describe the most common adverse effects for these drugs Introduction • Musculoskeletal pain is common • Surveys indicate a yearly prevalence of low-back symptoms in 50% of working age adults • 15% to 20% seek medical care • 1 of 7 primary-care visits is prompted by musculoskeletal pain or dysfunction • Musculoskeletal disorders are leading causes of disability and work absenteeism • In 1990, an estimated $192 million were spent on medications for back pain in the United States Beebe et al. American Journal of Therapeutics 2005; 12:151-171. Spasmolytics Antispasticity drugs Antispasmodic agents • muscle cramping and tightness in neurological disorders, e.g., multiple sclerosis and cerebral palsy, spinal cord injury and disease • Prevent use-related minor muscle spasms • AKA centrally active muscle relaxants ANTISPASTICITY DRUGS Baclofen - Diazepam - Tizanidine – Dantrolene Diazepam – Tizanidine- also anti-spasmotics Spasticity • Common neurological problem in patients with damage of central motor pathways • Characterized by hyperexcitability of α-motorneurons in the spinal cord due to a loss of normal inhibitory function and an imbalance of excitatory and inhibitory neurotransmitters • Antispasticity drugs alter the activity of neurotransmitters in the CNS and peripheral neuromuscular sites Management of spasticity Identify specific patient and caregiver objectives: • Improve gait, activities of daily living, hygiene • Provide pain relief, ease of care • Decrease spasm frequency and pain CMAJ 2003;169(11):1173-9 Management of spasticity Initiate comprehensive spasticity management program: • Removal or treatment of noxious stimuli • Physical/occupational therapies; proper positioning & regular stretching • Oral drug therapy • Injection of botulinum toxin type A • Intrathecal baclofen • Surgical intervention Start at the top and work your way down. CMAJ 2003;169(11):1173-9 Sites of antispasticity drug action Drug Mechanism of action Baclofen Binds to GABAB receptors on presynaptic terminals of spinal interneurons resulting in hyperpolarization of the membrane, decrease in Ca++ influx, decrease in excitatory neurotransmitters Diazepam Acts on GABAA receptors to enhance inhibition at pre- and postsynaptic sites in the spinal cord; it also acts in the brain Tizanidine Acts presynaptically at α-2 adrenergic receptors to inhibit spinal motor neurons Dantrolene Reduces Ca++-mediated excitation-contraction coupling through block of release channels on the sarcoplasmic reticulum of skeletal muscle Baclofen: pharmacokinetics • • • • Well absorbed; relative bioavailability: 70%–80% Time to peak concentration: 2–3 h Onset of action: hours to weeks (3 – 4 d) Widely distributed; crosses blood-brain barrier readily; protein binding: 30% • Metabolism: minimal hepatic (15% of dose) • Excretion: 70%–80% (parent compound in urine/feces) • Elimination t 1/2: 2.5–4 h Baclofen: adverse effects • • • • • • • Drowsiness initially; tolerance develops with chronic use Hypotension Elevated transaminases (ALT, AST, alkaline phosphatase) May cause positive stool guaiac Increase in serum glucose (hyperglycemia) Avoid abrupt withdrawal (hallucinations, seizures) Caution recommended in patients with seizures or renal impairment Baclofen • Continuous intrathecal baclofen is an option for patients unable to tolerate or unresponsive to oral therapy Pump/reservoir implanted between the muscle and skin of the abdomen A catheter carries baclofen from the pump to the spinal cord and nerves Diazepam (valium): pharmacokinetics • • • • • • • • Well-absorbed Time to peak concentration: 1-2 hours Onset of action: 15 – 30 minutes Widely distributed; crosses blood-brain barrier readily Metabolism: hepatic via CYP450 to n-desmethyl-diazepam (active metabolite) Multiple drug interactions! Excretion: urine as glucuronide conjugates Elimination t 1/2: > 48 hours Anything that causes sedation is a drug interaction for ALLL of the drugs in this presentation (ex. anti-histamines, sedatives, hypnotics, etc…) and metabolized via CYP450 Diazepam: adverse effects • • • • Sedation, lightheadedness, ataxia, lethargy Impaired mental and psychomotor function Anterograde amnesia Physical dependence and withdrawal upon abrupt discontinuation • Abuse potential (C IV) • Pregnancy Category D: freely crosses the placenta and accumulates in fetal circulation Tizanidine: pharmacokinetics • Bioavailability is 40% due to extensive hepatic first-pass metabolism (95%) • Peak effect: 1–2 h • Metabolism: hepatic via CYP 1A2; avoid with ciprofloxacin • Excretion: urine (60%); feces (20%) • Elimination t1/2: 2.5 h • Caution in patients with renal insufficiency as clearance is reduced by 50% Tizanidine: adverse effects • Tizanidine is an α-2 agonist similar to clonidine • Dose-related hypotension, sedation and dry mouth • Rare but severe hepatotoxicity; monitor transaminases (ALT, AST) • Withdrawal and rebound hypertension with abrupt discontinuation; tapering is recommended Dantrolene Pharmacokinetics Adverse effects • Well absorbed • Metabolism: hepatic CYP450 • Excretion: urine/bile • Elimination t 1/2: 15 h • Hepatotoxicity with chronic use • Drowsiness, dizziness, weakness, malaise, fatigue Drug of Choice (DOC) for malignant hyperthermia: high fever, tachycardia, hypertension, rigidity MOTOR NERVE BLOCKER Botulinum toxin Botulinum toxin type A • Produced by anaerobic bacterium Clostridium botulinum • MOA: Blocks the release of ACh from the motor nerves resulting in long-lasting muscle paralysis (~3 months) Used IM for: • muscle disorders of the eye (blepharospasm, strabismus) • elective cosmetic purposes • spasticity, e.g., cerebral palsy Best for small areas of focal spasm • Contraindicated in pregnancy & lactation ANTISPASMODIC DRUGS Chlorzoxazone – Cyclobenzaprine – Diazepam - Metaxalone – Methocarbamol – Orphenadrine - Tizanidine Indications Painful musculoskeletal conditions including: • Low back pain Myofascial pain syndrome • Fibromyalgia • Tension headaches Fast facts • Among the top 200 drugs dispensed in 2006 • However, NOT recommended as first line therapy • Acetaminophen & NSAIDs are the DOC • Use as adjuncts to physical therapy Pharmacology • Unknown! Do not act on motor neurons or the muscle itself • Act on the brain, maybe spinal reflexes • CNS depressants induce sedation • Diazepam enhances the effects of GABA at receptors in the brain Chlorzoxazone: pharmacokinetics • Readily absorbed • Peak concentration: 1–2 h • Metabolism: extensive hepatic phase II to glucuronides – CYP 450 Substrate: 1A2, 2A6, 2D6, 2E1, 3/4 – CYP 450 Inhibitor: 2E1, 3A4 • Excretion: urine (conjugates); <1% excreted unchanged Chlorzoxazone: adverse effects • • • • Dizziness, drowsiness Red or orange urine Hepatotoxicity (rare); monitor LFTs Contraindicated in patients with hepatic dysfunction • FDA Pregnancy category C Cyclobenzaprine: pharmacokinetics • • • • • GOLD STANDARD DRUG= DRUG OF CHOICE Absorption: oral, complete Peak concentration: 3–8 h Protein binding: 93% Metabolism: extensive; conjugation to glucuronide – CYP450 Substrate: 1A2, 2D6, 3A4 • Elimination: renal (50%) inactive metabolites; unchanged drug in feces via bile • Elimination t1/2: 1–3 d Cyclobenzaprine: adverse effects • • • • • • • • 5-HT2 receptor antagonist, related structurally to cyclic antidepressants Tachycardia, hypotension, arrhythmias (rare), MI (rare) Drowsiness, lethargy, lightheadedness, dizziness Dry mouth, urinary retention, intraocular pressure Seizures (rare) MOST evidence for efficacy Avoid with other serotonergic agents, recent MI, arrhythmias, glaucoma QT prolongation and possible torsade de pointes have been reported with fluoxetine, a CYP4502D6,3A4 inhibitor • FDA Pregnancy Category B Metaxalone: pharmacokinetics • Well absorbed; peak levels: 2-3 h • Metabolism: hepatic – CYP450 substrate 1A2, 2A6, 2D6, 2E1, 3/4A – CYP450 inhibitor: 2E1, 3A4 • Elimination: metabolites via kidney • Elimination t1/2: 2.4h (fat meal) to 9.2 h (fasting) Metaxalone: adverse effects • • • • Drowsiness, dizziness, headache, nervousness Leukopenia, hemolytic anemia (rare) hepatic transaminases Contraindications: significant renal/hepatic impairment; hypersensitivity • FDA Pregnancy Category C Methocarbamol: pharmacokinetics • • • • • • Absorption: rapid and complete Peak serum concentration: 1 - 2 h Distribution: widely throughout the body Metabolism: hepatic (first pass) Elimination t1/2: 1–2 h Elimination: renal 3d after 1 dose Methocarbamol: adverse effects • Black, brown, or green urine • Lightheadedness, dizziness, drowsiness • FDA Pregnancy category C; fetal abnormalities have been reported Orphenadrine: pharmacokinetics • Readily absorbed from GI tract, variable in overdose due to anticholinergic effects • Peak effects: 2–4 h • Widely distributed; protein binding: 20% • Metabolism: hepatic • Elimination: primarily renal (60%) metabolites, 8% parent compound • Elimination t1/2: 14–16 h Orphenadrine: adverse effects • Drowsiness, dry mouth, urinary retention, increased intraocular pressure • Aplastic anemia (rare) • Confusion • Tachycardia • Contraindications: glaucoma, myasthenia gravis • Reduce dose in older patients • FDA Pregnancy Category C Carisoprodol • Brand name: Soma • Metabolized to meprobamate, a C III controlled substance physical & psychological dependence • No better than any other SMRs • DO NOT USE!!! Safety • Sedation – caution when driving or operating heavy machinery • Additive effects with alcohol or other sedativehypnotics • Caution in elderly Evidence of effectiveness Studies are not well-designed: • • • • Inadequate randomization No mention of allocation concealment Not using intention-to-treat methods Incomplete reporting of compliance Evidence of effectiveness A formal literature synthesis concluded that oral SMRs • are effective in acute low-back pain and roughly equivalent to NSAIDs but found little evidence of effectiveness in chronic low-back pain • it is not clear to what extent pain relief is affected by muscle relaxation versus the sedative effect of SMRs • combinations of an SMR with an NSAID show increased efficacy over single agents SORT: Key Recommendations for Practice Clinical recommendation Evidence rating Skeletal muscle relaxants are not considered first-line therapy for musculoskeletal conditions. C Skeletal muscle relaxants may be used as adjunctive therapy for acute low back pain. B Antispasmodic agents should be used short-term (two weeks) for acute low back pain. C There is no clear evidence that one skeletal muscle relaxant is superior to another for musculoskeletal spasms. B Choice of skeletal muscle relaxant should be based on individual drug characteristics and patient situation. C A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patientoriented evidence; C = consensus, disease oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, see See et al. Am Fam Physician 2008; 78:365-70. http://www.aafp.org/afpsort.xml.