Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Atrial fibrillation wikipedia , lookup
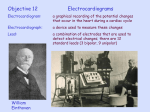
EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ CARDIAC EFFECTS OF CILOSTAZOL: A SELECTIVE TYPE-3PHOSPHODIASTERASE INHIBITOR, AN EXPERIMENTAL STUDY By Mahmoud Samy Zakaria, and Manal Abdel Aziz A. Department of Forensic Medicine and Clinical Toxicology El-Minia Faculty of Medicine ABSTRACT: This study was done to estimate the effects of cilostazol on the heart. It was carried out on 60 adult male guinea pigs weighing 400±20 (400-450). Guinea pigs were divided into three groups, each contained 20 animals. Group (1) was the negative control group, group (2) was the positive control group received 1ml. benzyl alcohol ( 15 %) daily by orogastric tube, and group (3) which received cilostazol in a dose of 6.2 mg/animal/day dissolved in 1ml. (15%) benzyl alcohol also administered by the orogastric infusion method. The experiment continued for 3 months then the whole animals were anaesthetized through intraperitoneal injection of 1 ml. (25%) urethane sodium to facilitate performance of electrocardiogram. Using limb leads connected to the animal 4 limbs all over a duration of 3 minutes. Lastly animals were sacrificed and the cardiac specimens were collected for the histopathological examination. Results of the present study revealed that ECG of the negative control group was within normal rhythm and rate (150.4±5.914) and without any pathological changes. The same could be considered for the positive control group but with a mild increase in the heart rate (165.95±8.71). However cilostazol administered group showed a well manifest sinus tachycardia with the heart rate ranged from 216 to 246 beats /minute (236.5±5.92) with a short P-R and Q-T intervals. Histopathological changes were within normal for the whole examined animals. In a conclusion oral administration of cilostazol is able to induce a potent enhancement of heart rate which is the early manifestation of heart failure. KEY WORDS:Cilostazol Ventricular tachycardia. Cardiac effects Antiplatelets aggregation aged Phosphdiasterase inhibitors peripheral vascular insufficiency particularly intermittent claudication. It has been demonstrated that cilostazol has positive chrontropic and dromotropic effects in patients with supraventricular bradyarrhythmia, such as those with sick sinus syndrome,and in those patients with atrioventricular block (Dormandy & Rutherford, 2000). INTRODUCTION: Cilostazol (6-[4-cyclohexyl1H-tetrazol-5-yl) butoxy]-3,4-dihydro2 (1H)-quinolinone) was opproved for marketing in Japan in 1988, as an antiplatelet agent to improve peripheral ischeamic symptoms, such as pain, cold sensations, and ulcerations that were caused by chronic arterial occlusive diseases (Okuda et al., 1993). Cilostazol is an antiplatelet drug which inhibits platelets aggregation. Cilostazol specifically inhibits type III phosphdiasterase (PDEIII), In 1999, cilostazol was approved by the U.S. Food and Drug Administration for treatment of 262 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ which is compartmentalized in cardiac moncytes and vascular smooth vessels. PDEIII is also found in platelets. Inhibition of PDEIII causes cascade of effects including higher tissue levels of cAMP, local activation of protein kinase, and ultimately cardiac contractility. The drug is contraindicated, however in patients with congestive heart failure (Bristow et al., 2001). - Crystalline cellulose - Corn starch - Carmellose calcium -Hydroxypropyl methylcellulose - Magnesium stearate 2- Benzyl alcohol (15 %):It was obtained from the faculty of Agriculture in El- Minia University. 3- The anaesthetic drug:Urethane sodium 25% (PDH, London), marketed as urethane sodium obtained from laboratory of biology department, Faculty of Sciences, El Minia University. Peripheral arterial disease is a highly prevalent manifestation of atherosclerosis that is associated with a substantial risk of illness and death and a marked reduction in ambulatory capacity and quality of life. The severity of peripheral arterial disease is closely associated with the risk of myocardil infarction, ischeamic stroke and death from vascular causes. Cilostazol improves both pain- free and maximal tread mill walking distance and the quality of life (William & Hiatt, 2001). B) Animals:A total of 60 adult male guinea pigs were used in this expermintal work, obtained commercially weighing about 400±20 (400-450).Animals were acclimatized at the constant environmental condition for one week prior to the experiment. A) Instruments:1- Orogastric tube used for orogastric infusion of the drug and its solvent. 2- Plastic syringe graded from 0.1:1 ml. used for intraperitoneal injection of the anaesthetic drug. 3- Electrocardiogram apparatus (Fokoda- Japan), using lead II. Added to the antiplatelet activity, cilostazol possesses also a potent vasodilating properties making the drug as an interesting candidate for the future clinical trials of delayed cerebral vasospasm (Birk et al., 2004). This study was designed to assess the cardiovascular toxicity of cilostazol. MATERIALS AND METHODS: I) Materials:A) Chemicals:1- Cilostazol:It was obtained from Egypt Otsuka Pharmaceutical Co., S.A.E., marketed as Pletaal. It was in a tablet form each contained 100mg. cilostazol. The active ingredient was as an odourless and tasteless white tablets formed of pale yellow white crystalline powder, highly soluble in benzyl alcohol (Cheng, 1999). Each tablet contained also inactive ingredients such as:- II) Methods: Administration:1- Cilostazol:- According to Fumio et al., (2000) who gave a human oral dose equls 100mg. twice daily for prevention of recurrence of cerebral infarction, also according to Dawson et al., (1998) who used the same dose in human for treatment of peripheral vascular disorders such as claudication. The drug was given to animals in a dose of 6.2mg/animal/day dissolved in 1 ml. benzyl alcohol (15%). Human dose was transformed into dosage for 263 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ guinea pigs by Paget and Barnes table (1964). 2- Benzyl alcohol (15%):According to Ettinger et al., (1978) who used benzyl alcohol as a solvent. The alcohol was given to animals in a dose of 1 ml./animal/day. Route of administration:- orogastric infusion using orogastric tube. The experiment ended after 3 months. 3- Urethane sodium (25%):According to Langou et al., (1980) who anaesthetized guinea pigs using urethane sodium, animals were injected intraperitoneally by 1 ml. urethane sodium to facilitate perfomance of electroca-rdiogram. The experiment ended after 3 months. All animals were anaesthetized and electrocardiogram was performed using lead II over a duration of 3 minutes. ECG changes were recorded and the heart rate changes were submitted to statistical analysis using Unpaired student t test. Autopsy and sampling:Animals were sacrified at the end of the study and the cardiac specimens were carefully dissected, then put into a container felt with 10% formalin for primary fixation over 24 hours duration. Parrafin sections were prepared, stained with Heamatoxylin and Eosin stain (H&E) and examined microscopically for histopathological evaluation, then photographs were taken. Guinea pigs were divided into 3 groups, each contained 20 animals: * Group (1):- was the negative control group. Animals of this group were kept in the ordinary environmental and allowed to free access to food and water. Handling was only during the routine weekly cage cleaning. * Group (2):- was the positive control group. Animals of this group received benzyl alcohol (15 %) * Group (3):- was the drug examined group. Animals of this group received cilostazol dissolved in benzyl alcohol. RESULTS: I)Electrocardiographic changes:1-Negative control group:As shown in figure (1), ECG record was of an average rate equals 150 beat/minute, with a regular rhythm, normal P-R and Q-T intervals, normal S-T segment and normal P&T waves. Figure (1): showing ECG record of the negative control group with heart rate = 150 beat/ minute, with regular rhythm, normal P-R and Q-T intervals, normal S-T segment and normal P& T waves 264 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ 2- Positive control group:Administration of benzyl alcohol resulted into a significant acceleration of the mean heart rate from (150.4±5.914) for the negative control group up to (165.95±8.71). Figure (2): Showing ECG record of the positive control group with the minmal increase in heart rate (168 beat/minute) with regular rhythm, short P-R and QT intervals. Figure (3): Showing ECG record of the positive control group with the maximal increase in heart rate (180 beat/ minute) with regular rhythm, short P-R and QT intervals. 3- Cilostazol administered group:Oral administration of cilostazol significantly accelerated the mean heart rate from (150.4±5.914) for the negative control group up to (236.5±5.92). As shown in figure (4) ECG record with the minimal increase in heart rate = 225 beat/minute, (a well manifest sinus tachycardia), with short P-R and Q-T intervals, but still within its regular rhythm. 265 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ Figure (4): Showing ECG record of cilostazol administered group with the minmal increase in heart rate = 225 beat/ minute with regular rhythm, short P-R and Q-T intervals. Figure (5) showing ECG record with the maximal increase in heart rate =236 beat/minute with a well manifest sinus tachycardia, short P-R and Q-T intervals, but still within its regular rhythm. Figure (5): Showing ECG record of cilostazol administered group with the maximal increase in heart rate =236 beat/ minute (a well manifest tachycardia) but still within regular rhythm , also with a short P-R and Q-T intervals. Unpaired t test demonstrated that cilostazol could significantly accelerate the heart rate in comparison to the negative control group (Table-1), and in comparison to the group received the benzyl alcohol as a solvent (table-2) 266 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ Table (1): Showing the effects of benzyl alcohol and cilostazol on heart rate in comparison to the negative control group. Group (1) Group (2) Mean ± SD 150.4 ± 5.914 (141-160) Group (3) Mean ± SD P value t value 65.95±8.71 (148-190) 0.000 ** 6.627 Mean ± SD p value t value 236.5±5.92 (216-246) 0.000 ** 46.057 Group (1) : The negative control group Group (2) : The positive control group received benzyl alcohol Group (3) : The drug administered group SD = Standard deviation *P<0.05 **P<0.001 Table (2) : Showing the effects of cilostazol on heart rate in comparison to the positive control group Group(2) Mean ± SD Group (3) Mean ± SD p value 165.95±8.71 236.5±5.92 29.97 (141-160) (216-246) Group (1) : The negative control group Group (2) : The positive control group received benzyl alcohol Group (3) : The drug administered group SD = Standard deviation *P<0.05 t Value 0.000 ** **P<0.001 II) Histopathological changes:There were no evidences indicating any pathological changes in the whole examined cardiac specimens related to the three examined groups. . Photomicrograph (1):- Section of a heart showing normal histological structure of the negative control group H&E X 400 267 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ Photomicrograph (2):- Section of a heart showing normal histological structure of the positive control group H&E X 400 Photomicrograph (3): Section of a heart showing normal histological structure of cilostazol administered group H&E X 400 268 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ Also these results are in agreement with Gamssari et al., (2002) who described a 92 year old woman with no apparent predisposing factors and a recent history of cilostazol use and suffered several episodes of ventricular tachycardia, two days after admission and intake of cilostazol, and when cilostazol was discontinued the condition subsided. DISCUSSION: Peripheral arterial disaese may be asymptomatic, or may be associated with critical limb ischaemia. Coronary artery disease and other atheroscelerotic vascular disorders may coexist with the peripheral arterial disease. Modifiable risk factors such as cessation of cigarette smoking and control of dyslipideamia, hypertention and diabetes should be treated. Antiplatelet drugs especially aspirin, exercise rehabilitation programs and cilostazol improve the limb threatening ischaemia (Aronow, 2005) Results of the current study supported the hypothesis described by Kishida et al., (2001) who said that cilostazol has beneficial effects in patients with bradycardic atrial fibrillation. The increased heart rate may be mediated by improvement of conductivty in the atrioventricular node and increase of coronary blood supply caused by dilatation of the vessels. In such study, cilostazol increased 24hour total heart beat counts from 69.685±1.690 to 87.532±3.123. Cilostazol is a quinolinone derivative with antithrombotic, vasodilator, and cardiotonic properties. Cilostazol causes positive inotropic and chronotropic effects both directly and indirectly. Clinical trials have shown that the antiplatalet agents are effective in treatment of peripheral vascular insufficiency. However, oral administration of cilostazol is accompanied with an equivilant cardiovascular risk (Ciancerelli et al., 2003). The minimal increase in cardiac adverse events following administration of cilostazol, could be related to its phosphdiasterase type-3 inhibitory activity, a condition which could explain the results of the study Shintani et al., (1985), as cilostazol in anaesthetized dogs, increased the the heart rate, cardiac contractile force, myocardial oxygen consumption and also increased the respiratory rste. And in conscious rats, the drug inreased the heart rate, while in guinea pigs, cilostazol produced a very slight increase in beating rate of the isolated atrium and a very slight increase in contraction of the papillary muscle. Consequently this study was done to evaluate the cardiovascular toxicity following 3 months medication with cilostazol. The present study revealed a highly significant sinus tachycardia from (141-160 beat/minute) up to (227-246 beat/minute) following intake of cilostazol in comparison to the negative control group, a matter coinciding with Woo et al., (2002) who detected approximately the maximal increase in heart rate 13.49% about 6 hours after administration of cilostazol in a study which was done to correlate between the peak plasma level of the drug and its cardiovascular effects in healthy individuals. In the study Toyonaga et al., (2000), 13 patients with chronic atrial fibrillattion associated with episodes of bradycardia, they received 100mg cilostazol per day. This study resulted into increased heart rate by an average of 3.3±0.8 beats/minute weeks after 269 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ onset of cilostazol treatment. In a conclusion coinciding with the results of the present study, that cilostazol improves the slow heart rate episodes associated with chronic atrial fibrillation and maintains the heart rate circadian variation and time- domian variability, indicating that cilostazol has therapeutic utility for treatment of slow heart rate associated with atrial fibrillation. premature beats, and non sustained ventricular tachycardia (Toyonaga et al., 2000). The sinus tachycardia following cilostazol administration was also in agreement with (Atrashi et al., 1998) who examined 20 patients with variable types of breadyarrhythmias, and 2 weeks after oral daily administration of cilostazol, the 24- hour total heart beat count increased from 77.429 ± 11.168) to (107.98 ± 3.536), p<0.001. In a conclusion, cilostazol had a beneficial positive chronotropic effect in patients with bradyarrhythmias, especially with bradycardiac atrial fibrillation and sick sinus syndrome. The positive chronotropic effects of cilostazol were in accordance with Kodama et al., (2003) who reported a significant increased mean ± standard error of the mean of total 24 hour QRS count from 57.300±2.8 to74.4±3.2 (p=0.001), and they concluded also that cilostazol significantly increased the ventricular escape rate, and recommend usage of the drug safely to selected patients with third degree atrio-ventricular block over a short term therapy. Results are coinciding with the data from more than 2000 patients who were followed up to six months were presented to the FDA, death from cardiovascular causes occurred in 0.6% of cilostazol treated patients and 0.5% of placebo treated patients. Myocardial infarction occurred in 1.5% of cilosatzol treated patients and 1.1% of placebo- treated patients (Dawson et al., 1998). The accelerated heart rate following cilostazol administration was in the same line of what had been mentioned by (Cheng,1999), and (Cone et al., 1999) in that cilostazol is contraindicated in patients with severe heart failure because of the determintal effects demonstrated by other agents in the same class. CONCLUSION: Cilostazol possesses a propable risk of ventricular tachyarrhythmia, aggravation of congestive heart failure which might alter the risk- to- benefit ratio in certain patients. The ability of cilostazol to increase levels of cAMP could predipose patients to ventricular arrhythmias. RECCOMENDATIONS: Heart rate variability is an important predictor of mortality in patients with heart disease. Based on this fact, it is recommended when cilostazol is a must, to put such patients carefully under monitoring for any anginal signs or symptoms (e.g. chest pain) since treatment with cilostazol may potentiate the heart rate Similarly, in animal studies, cilostazol increased heart rate, myocardial contractile force, ventricular automaticity, and ventricular conduction (Approval of New Drug Application for Pletal, 1999). In human beings, its use has been associated with increased mean heart arte, conductivity in the atrioventricular node, ventricular 270 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ up to the degree of aggravating the symptoms angina pectoris. 5. Bristow M.R.; Port J.D., and Kelly R.A. (2001): Treatment of heart failure: pharmacological methods.In: (Heart Disaease a Textbook of Cariovascular Medicine) 6th. Edition, edited by : Braunwold E.; Zipes D.P, and Lippy P. Philadelphia : W.B. Saunders: 562-599. 6. Cheng J.W. (1999): Cilostazol. Heart Dis., 1(3):182-186. 7. Ciancerelli I.T.; Ciancerelli M.G.; Massimo C.; Marini C., and Carolei A. (2003): Urinary nitric oxide metabolites and lipid peroxidation byproducts in migraine. Cephalalgia, 23:39-42. 8. Dawson D.L.; Culter B.S.; Meissner M.H., and Standness D.E. (1998): Cilostazol has beneficial effects in treatment of intermittent claudication: results from a multicenter, randomized, prospective, double-blind trial. Circulation, 98: 678686. 9. Dibianco R.; Shabetai R.; Kostuk W., and Moran J. (1989): A comparison of oral milrinone, digoxin, and their combination in the treatment of patients with chronic heart failure. N. Engl. J. Med., 320:677-683. 10. Dormandy J.A., and Rutherford R.B. (2000): Management of peripheral disease (PAD). J. Vasc. Surg.,31: S1-S296. 11. Ettinger B.O.; Wu C.F., and Robin E. (1978): Benzyl alcohol associated cardiac rhythm disorders. Am. Heart Journal, 95 (2): 554. 12. Fumio G.; Hideo T.; Shunsaku H.; Akirot., and Yasuo F. (2000): Cilostazol stroke prevention study: A placebo- Controlled Double- Blind Trial for secondary Prevention of Cerebral Infarction. Journal of Stroke and Cerebrovascular Disease, 9(4): 147:157. 13. Gamssari F.; Mohamed H.; John H.; Rollo P.V., and Brant L. (2002): Rapid ventricular tachycardias If any evidences of adverse reactions such as severe tachycardia are observed during cilostazol therapy, the drug should be discontinued immediately and the appropriate corrective measures are taken, such as dosage reduction. Patients with a pre-existing heart disease such as the congestive heart failure, rheumatic, or ischeamic heart, should not receive the drug as the condition may be worsened. Much more studies are needed to determine exactly which populations might be affected and being at a higher risk.The long term chronotropic effect of cilostazol on human, need to be evaluated. REFERENCES: 1. Approval of New Drug Application for Pletal (cilostazol) (1999): Letter to Otsuka American Pharmaceutical, Inc., from Center of Drug Evaluation and Research, Food and Drug Administration, Departement of Health and Human Services; Rockville. 2. Aronow W.S. (2005): Management of peripheral arterial disease. Cardiol. Rev., 13 (2):61-68 3. Atarashi H.; Endoh Y.;Saitoh H., and Kishida H. (1998): Chrontropic effects of cilostazol, a new antithrombotic agent, in patients with bradyarrhythmias. J. Cardiovascu. Pharmacol., 31 (4):534-539 (English abstract). 4. Birk S.; Kruuse C.; Petersen K.; Jonassen o., and Tfelt-Hansen P. (2004): The phosophdiasterase –3 inhibitor cilostazol dilates large cerbral arteries in humans without affecting regional cerebral blood flow. J. cerb. Blood Flow Metab., 24 (12) :13521358 ( English abstract). 271 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ associated with cilostazol use. Tex. Heart Inst. J., 29 (2): 140-142. 14. Kishida M.; Watanabe K.; and Tsuruoka T. (2001): Effects of cilostazol in patients with bradycardiac atrial fibrillation. J. Cardiol, 37(1):2733. (English abstract) 15. Kodama T. K.; Kurata A.; Oshima K.; Yamamoto K., and Uemura s. (2003): Effect of ciolstazol on the ventricular escape rate and neurohumoral factors in patients with third-degree atrioventricular block. Chest, 123(4):1161-1169. (English abstract) 16. Langou R.A.; Van Deyke C., and Tahan S.R. (1980): Cardiovascular manifestation of urethane anaesthetic drug. Am. Heart Journal, 100: (1): 458. 17. Okuda Y.; Kimura Y., and Yamashita K. (1993): Cilostazol. Cardiovasc. Drug Rev., 11:451-465. 18. Paget G., and Barnes B. (1964): Evaluation of drug activaties. Vol. (1):135 Academic Press. 19. Shintani S.; Watanabe K.; Kawamura K.; Mori T.; Toba Y.; Sasbe H., and Mori T. (1985): General pharmacological properties of cilostazol a new antithrombotic drug. Part II: Effect on the peripheral organs. Arzneimittel For Schung,35 (7A): 1163-1172. (English abstract ). 20. Toyonaga S.; Nakatsu T.; Murakami T.; Kusachi K., and Tominaga Y. (2000): Effects of cilostazol on heart rate and its variation in patients with atrial fibrillation associated with bradycardia. J. Cardio-vasc. Pharmacol. Ther., 5(3): 183-191 (English abstract). 21. William R., and Hiatt M. (2001): Medical Treatment of Peripheral Arterial Disease And Circulation. In: New England Journal of Medicine, edited by : Alastair J.J., and Wood M., 344(21):1608-1621. 22. Woo S.K; Kang W.K., and Kwon K.I. (2002): Pharmacokinetic and pharmacodynamic modeling of the antiplatelet and cardiovascular effects of cilostzol in healthy humans. Cli. Pharmacol. Ther., 71(4):246-252. 272 EL-MINIA MED., BULL., VOL. 16, NO. 1, JAN., 2005 Zakaria & Abdel Aziz ___________________________________________________________________________________ التأثيرات القلبية لعقار السيلوستازول المثبط االختيارى إلنزيم الفوسفودياستيراز3- "دراسة تجريبية" محمود سامي زكريا -منال عبد العزيز عبد الظاهر قسم الطب الشرعي و السموم اإلكلينيكية كلية الطب –جامعة المنيا آل ت ر أجريتته هتتلد اسةراتتتي ساآليتتيا الب ت ر استتتلبيي ل ت اسآلل ت واسن اجتتي تتت اتتتاقا استيلوتا زو 0وقة اشااله اسةراتي ل ةة 60خنزير غينت لرتر ويتزت لتواس 400جتا واا اآلتيا هلد اسليوان ه إس بالبي اجاو ه بليث ر نه ر اجاو ي ااروت ات 20خنزير0 واا إ ط ء اسقآل ر سليوان ه اساج ر بصورة اناظاي يوايت تت طريتل اسوتا وبواتتطي األنبوبتي اساقةيي ولسك ساةة بالبي أشهر وبجر ه اا بلي سلجر ه اسقالجيي اساتاخةاي0 ور نتتته اساجاو تتتي األوستتت هتتت اساجاو تتتي اساتتت بطي استتتت سبي واساجاو تتتي اسب نيتتتي اتتتا إ ط ؤه آل ر استيلوتا زو بجر ي 6.2الجا سر ليوات اج ر يواي والابه ف 1ال ات اسرلو اسبنزيل بارريز 0%15أا اساجاو ي اسب سبي فر نه اساجاو ي اسا بطي اساوجبي ليتث اا إ ط ؤه 1ال ات اسرلو اسبنزيل واساتاخةا رالي سلقآل ر است بل0 وبقة نه يي اساجربي اا اخةير ر اسخن زير اساتاخةاي ف اسبلث ت طريل لآلت 1ال ات اخةر اسيوريب ت صوةيوا بارريز %25ولسك ات خال اسلآلت بت ساجوي اسبرياتون بتا اتا ا رتا قل سر ليوات ساةة بالبي ةق ئل0 وف نه يي اساجربي اا لبح اسليوان ه واا اجايع ين ه اسآلل سلةراتي اسب بوسوجيي0 وقة أتوره نا ئج اسبلث ت أت هن ك زي ةة اطرةد وواالي ف تر ي ارب ه اسآلل نايجي ان و آل ر استيلوتتا زو بليتث أصتبله ااتراود اقتة اترب ه اسآللت ات بتيت : 216 246سر ةقيآلي اآل رني ب ساقة اسطبيق 165 : 150وهو سر ةقيآلي وه ظت هرة أوسيتي سهبتوط اسآلل االلاآل ن 0 وات هلا اسبلث نتاخلص أت آل ر استيلوتا زو ق ةرا ل أت يلةث زيت ةة فق سته فت ارب ه اسآلل قة اؤةى إس لةوث هبوط بقالي اسآلل 0 273