Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
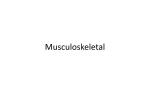
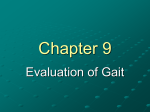
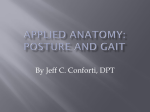
UNIT 2 – BIOMECHANICS OF THE LOWER LIMB Dr M J Dolan Department of Orthopaedic & Trauma Surgery University of Dundee Dr T Drew Department of Orthopaedic & Trauma Surgery University of Dundee SECOND EDITION Edited by Dr T Drew Department of Orthopaedic & Trauma Surgery University of Dundee Illustrations by Mr I Christie Published by Distance Learning Section Department of Orthopaedic & Trauma Surgery University of Dundee Second Edition published 2005: ISBN 1-903562-47-3 ISBN 978-1-903562-47-5 First Edition published 1994: ISBN 1-899476-50-4 Copyright © 2005 University of Dundee. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, and recording or otherwise, without prior permission from the publisher. The University of Dundee is a Scottish Registered Charity, No SC01509. UNIT 2 – BIOMECHANICS OF THE LOWER LIMB CONTENTS 1. HIP JOINT 1.1 Range of Motion 1.2 Hip Joint Loading During Standing 1.3 Hip Joint Forces During Daily Activities 2. KNEE JOINT 2.1 Motion of the Knee 2.2 Range of Motion 2.3 Function of the Patella 2.4 Function of the Menisci 2.5 Knee Joint Forces During Daily Activities 3. ANKLE AND FOOT 3.1 Ankle Joint 3.2 Ankle Joint Motion 3.3 The Foot 3.4 Subtalar Joint 3.5 The Arched Structure of the Foot 4. MOMENTS ABOUT JOINTS 4.1 Gait Analysis 4.2 Gait Cycle 4.3 Range of Joint Movement 4.4 Ground Reaction Forces 4.5 Joint Forces and Moments SUMMARY SAQ ANSWERS END OF UNIT EXERCISE UNIT 2 – BIOMECHANICS OF THE LOWER LIMB OBJECTIVES On completing your study of this unit you should be able to: 1. Describe the structure of the hip joint. 2. Define the terms: ball-and-socket joint and circumduction. 3. Describe the motion and range of motion of the hip joint. 4. Explain why the force at the hip joint is increased so greatly during unilateral stance compared with bilateral stance. 5. Describe the structure of the knee joint. 6. Describe the motion and range of motion of the knee joint. 7. Explain the function of the patella. 8. Explain the function of the menisci. 9. Describe the structure of the ankle and foot. 10. Describe the motion and range of motion of the ankle joint. 11. Describe the motion and range of motion of the subtalar joint. 12. Explain the function of the plantar fascia. 13. Discuss the relative stability of the lower limb joints. 14. Define the terms: gait, reciprocal gait and gait analysis. 15. List the equipment used in a gait laboratory. 16. Briefly describe the use of a motion analysis system. 17. Briefly describe the use of a force plate. 18. Describe the gait cycle. 19. List the phases and events of the gait cycle. 20. Draw a typical graph of the motion of the lower limb joints during reciprocal gait. 21. Explain the term: ground reaction force. 22. Draw a typical butterfly diagram and a graph of the vertical ground reaction force against time. 23. Describe the moments acting at the joints of the lower limb during reciprocal gait. UNIT 2 - BIOMECHANICS OF THE LOWER LIMB In this unit we will be looking at the major joints of the lower limb and examining the roles they play in walking. Walking is one of the most commonly executed human activities and is also one of the most demanding. Orthopaedic and rehabilitation devices, such as joint replacements, fracture fixation devices and lower limb prostheses and orthoses, must be able to withstand the demands placed on them during walking. A knowledge of these demands is therefore important to orthopaedic surgeons, prosthetists, orthotists and the designers of orthopaedic and rehabilitation devices. In particular, they must consider the range of joint motion required, the magnitudes of the joint forces and moments, and the interface pressures between the device and the patient, to ensure that the patient regains as much function as possible and that the device does not break during use. femoral head innominate bone thigh femoral neck femoral shaft femur patella fibula tibia leg foot metatarsals phalanges FIGURE 1. THE LOWER LIMB. The lower limb (Figure 1) consists of three segments: the thigh, the leg and the foot. The thigh is formed by the femur, the leg by the tibia and fibula and the foot by the tarsals, metatarsals and phalanges. Three major joints allow these segments to move relative to one another and the pelvic girdle. They are the hip, knee and ankle joints. These joints are synovial joints, held together by muscles and ligaments. When considering the joints of the lower limb it is important to remember that the joints are designed both for movement and for weight bearing. SAQ 1 (a) Name the three segments of the lower limb. (b) Name the three major joints of the lower limb. (c) State the two functions of the joints of the lower limb. Unit 2 - Biomechanics of the Lower Limb 1 1. HIP JOINT The hip joint is a ball-and-socket shaped synovial joint. A ball-and-socket joint consists of the ball-shaped end of one bone fitted into a cup-shaped depression of another bone (Figure 2B). In the hip joint, the ball consists of the head of the femur which fits into the socket-shaped acetabulum of the pelvic girdle (Figure 2A). This ball-and-socket shape allows the hip joint to rotate in three directions: flexion and extension, abduction and adduction, and internal and external rotation. The ball-andsocket shape also allows the hip joint to circumduct, whereby the femur moves in a circle relative to the pelvis. This movement is called circumduction (Figure 2C). HIP JOINT BALL-AND-SOCKET CIRCUMDUCTION abduction acetabulum head of femur adduction (B) external rotation internal rotation flexion extension circumduction (C) (A) FIGURE 2. (A) THE HIP JOINT (B) BALL-AND-SOCKET JOINT MOTIONS (C) CIRCUMDUCTION. The hip joint is a synovial joint, as are the other very mobile joints of the body which allow the major movements of the skeletal system. In synovial joints the surfaces of the bones that form the joint are covered in articular cartilage; a low friction material. Synovial joints are enclosed in a sleeve of tough fibrous tissue, the joint capsule, which forms the synovial cavity (Figure 3). The synovial cavity is filled with synovial fluid which lubricates the joint and provides nutrients to the articular cartilage. The synovial fluid resembles egg white; it is this resemblance that gives synovial fluid its name derived from the Latin for egg, ovum. The synovial fluid is produced by the synovial membrane which lines the inner surface of the capsule. bone joint capsule synovial fluid in synovial cavity articular cartilage synovial membrane bone FIGURE 3. A SYNOVIAL JOINT. Unit 2 - Biomechanics of the Lower Limb 2 SYNOVIAL JOINT The hip joint is surrounded by a very strong articular joint capsule and several ligaments. These are surrounded by several large, strong muscles. This arrangement is intrinsically stable and allows for the wide range of movement required for common daily activities such as walking, sitting and squatting. The stability of the hip joint derives from its shape, the joint capsule and the surrounding ligaments and muscles. Because of this stability dislocations of the hip are very rare in adults, and are usually only seen after serious road traffic accidents when very large impact forces are applied. SAQ 2 (a) What type of joint is the hip joint? (b) What are the two functions of synovial fluid? (c) Why is the hip joint intrinsically stable? 1.1 Range of Motion The hip joint has a wide range of movement in all three planes (Figure 4). The range of motion is greatest in the sagittal plane, where flexion and extension occur. Flexion ranges from 0 to about 140 degrees and extension from 0 to 15 degrees. In the frontal plane, abduction and adduction occur. Abduction ranges from 0 to 30 degrees and adduction ranges from 0 to 25 degrees. In the transverse plane, external and internal rotation occur. External rotation ranges from 0 to 90 degrees and internal rotation ranges from 0 to 70 degrees when the hip is flexed. Less external and internal rotation is possible when the hip is extended due to the restrictions of soft tissues. The hip joint can also be circumducted. 5° extension 25° adduction 35° flexion 30° abduction 90° external rotation 70° internal rotation FIGURE 4. RANGE OF MOTION OF THE HIP JOINT. To perform common daily activities, such as walking, standing up and sitting down, ascending and descending stairs, and stooping to pick up an object from the floor at least 120º of flexion-extension and 20 degrees of abduction-adduction and rotation are required. For example, standing up and sitting down in a chair requires about 110º of flexion-extension, 20º of abduction-adduction and 15 degrees of rotation. In walking, the most significant motion is in the sagittal plane with about 35 degrees of flexion and 5º of extension. Only about 12º of the motion is required in the other two planes. Unit 2 - Biomechanics of the Lower Limb 3 5° 110° 40° 120° FIGURE 5. MAXIMUM HIP FLEXION-EXTENSION ANGLES DURING STANDING UP, WALKING AND LIFTING. SAQ 3 (a) In which plane does the greatest range of motion of the hip joint occur? (b) Typically, what range of motion is required at the hip joint to stand up and sit down? 1.2 Hip Joint Force During Standing The force acting at the hip joint during standing can be calculated using simple mechanics. In this section we will calculate the hip joint force during standing on both feet (bilateral stance) and during standing on one foot (unilateral stance) (Figure 6). The latter case illustrates the importance of muscle activity in determining the magnitude and direction of joint forces. In both cases we will consider only the forces acting in the frontal plane. (A) (B) FIGURE 6. (A) BILATERAL STANCE (B) UNILATERAL STANCE. 1.2.1 Bilateral stance During bilateral stance (Figure 6A) there are normally no muscles active at the hip joint. Therefore to calculate the hip joint force we only need to consider the external forces Unit 2 - Biomechanics of the Lower Limb 4 present. There are only three external forces acting on the pelvis: the weight of the upper body acting downwards and two reaction forces, one at each hip joint, acting upwards (Figure 7). WHAT d = 14 cm d = 14 cm R1 R2 FIGURE 7. FORCES ACTING ON THE PELVIS IN BILATERAL STANCE. The weight of the upper body (the Head, Arms and Trunk - HAT). The upper body makes up approximately 70% of total body weight, W. The remaining body weight is made up by the two lower limbs at 15% each. Thus, for an individual weighing 800 N the upper body weight, WHAT, can be calculated as follows: WHAT = W × 70% = 800 × 0.70 = 560 N 100% The width between the two hip joints can be measured. In this case we will use 28 cm. The weight distribution is symmetrical thus the moment arm, d, about each hip is 14 cm. To calculate the force acting at the left hip, RLEFT, we apply the second condition of static equilibrium - the sum of all the moments is zero (Figure 8). d WHAT RLEFT right hip joint 2d FIGURE 8. MOMENTS ABOUT THE RIGHT HIP JOINT CENTRE. Summing the moments about the right hip joint centre (anti-clockwise is defined as positive): RLEFT × 2d – WHAT × d = 0 Rearranging the equation for RLEFT: Unit 2 - Biomechanics of the Lower Limb 5 RLEFT = WHAT d WHAT 560 = = = 280 N 2d 2 2 Thus the force acting at the left hip joint is 280 N. We can find the force acting at the right hip joint using the same method but instead of summing the moments about the right hip joint the moments are summed about the left hip joint. Alternatively we can use the first condition of static equilibrium - the sum of all the forces is zero (Figure 9). WHAT RRIGHT RLEFT FIGURE 9. FORCES ACTING ON THE PELVIS. Summing all the forces (up is defined as positive): RRIGHT + RLEFT – WHAT = 0 Rearranging the equation for RRIGHT: RRIGHT = WHAT – RLEFT = 560 – 280 = 280 N Thus the force acting at the right hip joint is 280 N. As you would expect this is the same as the force acting at the left hip joint. From this analysis we can conclude that during normal bilateral standing the forces acting at the hip joints are vertical and equal to half the upper body weight. 1.2.2 Unilateral stance During unilateral stance (Figure 6B) abductor muscle activity is required to stabilise the position of the body. To calculate the hip joint force we will consider the forces acting on the lower limb. There are four forces: the weight of the lower limb acting downwards, the abductor muscle force, the joint force at the hip, and the ground reaction force acting vertically upwards on the foot. To simplify the problem the abductor muscles are grouped with a single insertion point on the greater trochanter of the femur. Activity: Stand on both feet and palpate the flesh between your greater trochanter and pelvis. Whilst still palpating this area shift your weight on to that side so that you are standing on one foot. You should be able to feel the underlying hip abductor muscles (the glutei) contract to stabilise your position. All the forces are shown in Figure 10 along with various dimensions of the lower limb. A two-dimensional rectangular reference frame is used; the x-axis is defined as horizontal going from the lateral to the medial sides of the lower limb, the y-axis is defined as going vertically upwards, and for convenience the origin is at ground level directly below the insertion of the abductor muscle group. Unit 2 - Biomechanics of the Lower Limb 6 y A Jy J Ay Jx Ax 14 cm 11 cm 9 cm mg x G FIGURE 10. FREE BODY DIAGRAM OF LOWER LIMB DURING UNILATERAL STANCE. The direction of the abductor muscle force, A, is known but not its magnitude. It is acting at an angle of 70° to the horizontal. To simplify the calculations we will divide it into its two components: one acts along the x-axis, Ax, and one along the y-axis, Ay. The joint force, J, also has two components: one acts horizontally and laterally along the x-axis, Jx; and one acts vertically downwards along the y-axis, Jy. The ground reaction force is equal and opposite to the total body weight (Newton’s third law - to every action there is an equal and opposite reaction). Thus for an individual weighing 800 N the ground reaction force will also be 800 N. Each lower limb makes up approximately 15% of total body weight, W. Thus, for an individual weighing 800 N the weight of one of their lower limbs, WLL, can be calculated as follows: WLL = W × 15% = 800 × 0.15 = 120 N 100% One of the unknown forces, the vertical component muscle force, acts through the insertion point of the abductor muscles. Thus we can calculate the other unknown force of the vertical component of the joint force, Jy, by summing all the moments about this point (see Figure 11). Unit 2 - Biomechanics of the Lower Limb 7 dJ = 6 cm Jy dW = 11 cm WLL G = 800 N dG = 20 cm FIGURE 11. MOMENTS ABOUT THE INSERTION POINT OF THE ABDUCTOR MUSCLES. Summing the moments about the insertion point of the abductor muscles (anticlockwise is defined as positive): -JydJ – WLLdW + GdG = 0 Rearranging the equation for Jy: JydJ = GdG - WLLdW Jy = Gd G − WLL d W 800 × 0.2 − 120 × 0.11 160 − 13.2 146.8 = = 2446.67 N = = dJ 0.06 0.06 0.06 We can find the vertical component of the muscle force by summing all the forces in the vertical direction (Figure 12). Ay Jy = 2446.67 WLL = 120 N G = 800 N FIGURE 12. VERTICAL FORCES ACTING ON LOWER LIMB. Summing all the forces (up is defined as positive): Ay – Jy – WLL + G = 0 Rearranging the equation for RRIGHT: Ay = Jy + WLL – G = 2446.67 + 120 – 800 = 1766.67 N Unit 2 - Biomechanics of the Lower Limb 8 Ay = A sin 70° A 70° Ax = A cos 70° FIGURE 13. ABDUCTOR MUSCLE FORCE. The magnitude of the abductor muscle force can be calculated using trigonometry (Figure 13): Ay = A sin 70° Rearranging for A: A= Ay sin 70° = 1766.67 = 1880.05 N 0.939693 Thus the abductor muscle force acting to stabilise unilateral standing is around 1880 N. This is approximately equal to 3.4 times the subject’s upper body weight (560 N). SAQ 4 - Express the magnitude of abductor muscle force as a ratio of the subject’s total body weight. Using trigonometry we can also calculate the horizontal component of the abductor muscle force: Ax = A cos 70° = 1880.05 × 0.342020 = 643 N We can now find the last remaining unknown force, the horizontal component of the joint force, by summing the horizontal forces (Figure 14): Rearranging for Jx: Jx = Ax = 643 N Ax Jx FIGURE 14. HORIZONTAL FORCES ACTING ON LOWER LIMB. We now have values for the two components of the joint force. We can therefore calculate the magnitude and direction of the joint force using trigonometry (Figure 15). Unit 2 - Biomechanics of the Lower Limb 9 Jx J θ Jy FIGURE 15. HIP JOINT FORCE. To calculate the magnitude we can use Pythagoras’ theorem: J 2 = J 2x + J 2y J = J 2x + J 2y = 643.015 × 643.015 + 2446.67 × 2446.67 = 2529.76 N To calculate the direction: tan θ = Jy Jx Rearranging: ⎛ Jy θ = tan-1 ⎜⎜ ⎝ Jx ⎞ ⎟ = tan-1 ⎛⎜ 2446.67 ⎞⎟ = 75° ⎟ ⎝ 643.015 ⎠ ⎠ The hip joint force during unilateral stance was calculated as having a magnitude of around 2530 N and as acting at about 75° to the horizontal. Its magnitude is approximately 3.2 times body weight. This force is considerably larger than the hip joint force during bilateral stance which was calculated as being around 0.5 times the upper body weight. This increase in hip joint force is only partially accounted for by the fact that during unilateral stance only one hip is supporting the whole upper body rather than the two in bilateral stance. Most of the increase is due to the contraction of the hip abductor muscles which is required to stabilise the hip. The contraction of the hip abductor muscles effectively pulls the sides of the hip joint together greatly increasing the force at the hip joint. This interpretation is supported by the fact that the abductor muscle force was calculated as having a magnitude of around 3.4 times the upper body weight and as acting at about 70º to the horizontal. SAQ 5 (a) How does the abductor muscle activity affect the hip joint force during unilateral stance compared to bilateral stance? (b) Express the magnitude of the hip joint forces during bilateral and unilateral stance as ratios of the subject’s total body weight. 1.3 Hip Joint Forces During Daily Activity In the previous section we calculated that the hip joint forces during static bilateral and unilateral stance. Because the weight of the subject is so important in determining the magnitude of joint forces they are usually expressed as a ratio of the subject’s total body weight. This makes the results much more easier to understand. Thus from the previous example we have magnitudes of 0.4 body weight during bilateral stance, and 3.2 body weight during unilateral stance. We could expect similar results from subjects of very Unit 2 - Biomechanics of the Lower Limb 10 different body weights, despite the fact that the actual force magnitudes in newtons will vary greatly. During most daily activities the hip joint force is usually greater than body weight. For example during walking you could expect hip joint forces as high as 3 to 7 body weight depending on the speed of walking - the faster you walk the higher the force. Note: Many authors use the abbreviation BW for body weight. For example they may say that the average force was equal to 5.5 BW. This means that the average force was equal to 5.5 times the subject's total body weight. 2. KNEE JOINT The knee joint is the largest and perhaps most complex joint in the human body (Figure 16). It is composed of two articulations: the tibiofemoral (between the proximal surface of the tibia and the distal surface of the femur) and the patellofemoral (between the patella and the distal surface of femur). The movement of the knee joint is accounted for mostly by the tibiofemoral articulation with the patellofemoral articulation acting in concert to assist this movement. femur tibiofemoral articulation meniscus KNEE JOINT patellofemoral articulation patella articular cartilage tibia FIGURE 16. THE KNEE JOINT. The proximal surface of the tibia is flat and covered with the menisci (Figure 17). The menisci are two crescent shaped pieces of fibrocartilage that are attached to the tibia by short tough ligaments. The menisci make the flat top of the tibia slightly concave which aids stability. They also act as load distributors and shock absorbers. anterior cruciate ligament lateral meniscus medial meniscus posterior cruciate ligament FIGURE 17. VIEW OF TIBIAL PLATEAU FROM ABOVE SHOWING THE POSITION OF THE MENISCI. Unit 2 - Biomechanics of the Lower Limb 11 MENISCI The distal end of the femur is formed by two circular-shaped condyles - the femoral condyles. The femoral condyles are covered by articular cartilage. The smooth anterior depression between the femoral condyles is called the trochlea. This develops into the deep posterior depression between the femoral condyles called the intercondylar notch. The cruciate ligaments, that help to bind the femur to the tibia, are lodged in the intercondylar notch. FEMORAL CONDYLES The patella (knee cap) is the largest sesamoid bone (that is a bone found in a tendon) in the body. It is located in the tendon of the quadriceps femoris muscle. The posterior surface of the patella has two smooth articular surfaces either side of a slight central ridge. The two articular surfaces articulate with the respective femoral condyle. The ridge guides the patella along the groove between the femoral condyles as the knee joint flexes and extends. PATELLA Note the fibula does not form part of the knee joint, however, it does act as an anchor for the biceps femoris muscle and lateral collateral ligament. SAQ 6 (a) Name the two articulations that comprise the knee joint. (b) What type of bone is the patella? Unlike the hip joint, the shape of the bones that form the knee joint are such that they contribute very little to its stability. Instead, the stability of the knee joint is derived mainly from its ligaments (Figure 18). Within the joint the anterior and posterior cruciate ligaments cross each other in the centre of the joint. They limit forward and backward sliding of the femur on the tibia and limit hyperextension. The joint is surrounded by a tough fibrous joint capsule which is thickened around the posterior on the medial and lateral sides. Outside the capsule on either side lie the medial and lateral collateral ligaments which prevent abduction and adduction respectively. The quadriceps muscle also aids stability as do the menisci, especially during rotation. CRUCIATE LIGAMENTS COLLATERAL LIGAMENTS anterior cruciate ligament lateral collateral ligament medial collateral ligament lateral meniscus medial meniscus posterior cruciate ligament lateral collateral ligament (A) (B) FIGURE 18. THE LIGAMENTS OF THE KNEE JOINT (A) ANTERIOR VIEW (B) POSTERIOR VIEW. SAQ 7 - What gives the knee joint its stability? 2.1 Motion of the Knee The knee joint is generally considered to behave like a hinge joint. However, although the knee joint can be adequately described as a hinge joint it does demonstrate subtle variations. Unit 2 - Biomechanics of the Lower Limb 12 HINGE JOINT A hinge always rotates about the same axis (Figure 19A). This is not true for the knee joint - its axis of rotation changes as it flexes and extends. If the sagittal plane is considered then the centre of rotation of the knee joint moves in an approximate semicircle as shown in Figure 19B. This semicircular pattern arises because the femoral condyles are not perfectly circular and because of the restrictions imposed by the knee ligaments. Deformities of the knee joint surfaces cause the centre of rotation to follow more complex patterns. centre of rotation axis of rotation (A) (B) FIGURE 19. (A) HINGE JOINT (B) ROTATION OF KNEE JOINT. When the rotation of the knee joint is studied in all three dimensions and not just in the sagittal plane it becomes apparent that it is not a hinge joint with a moving axis of rotation. It has a screw-home mechanism, whereby it follows a spiral motion. As the knee flexes the tibia rotates internally and as the knee extends the tibia rotates externally (Figure 20). This spiral motion is a consequence of the different sizes of the lateral and medial femoral condyles (in a normal knee the medial condyle is about 1.7 cm longer than the lateral condyle). extension flexion and internal rotation flexion external rotation extension and external rotation internal rotation FIGURE 20. SCREW-HOME MECHANISM OF THE KNEE JOINT. In addition to rotation, the knee joint also allows a limited amount of abduction and adduction, and internal and external rotation. Unit 2 - Biomechanics of the Lower Limb 13 SCREW-HOME MECHANISM SAQ 8 (a) Describe how the knee joint’s centre of rotation changes in the sagittal plane as it flexes and extends. (b) What does the screw-home mechanism describe? 2.2 Range of Motion The range of joint motion in the knee joint can be attributed to the tibiofemoral articulation. This essentially hinged synovial joint allows the greatest motion to occur in the sagittal plane, although motion in the other two planes does occur. rotation 0° at full extension extension <5° (B) (A) internal rotation 30° flexion 140° external rotation 45° at 90° flexion FIGURE 21. RANGE OF MOTION OF THE KNEE JOINT (A) SAGITTAL PLANE (B) TRANSVERSE PLANE. In the sagittal plane, flexion and extension occur. The range of motion is from a few degrees of extension to about 140 degrees of flexion (Figure 21A). In the frontal plane, abduction and adduction occur; the range of motion in this plane is dependent upon how much the knee is flexed. It is at its maximum at about 30 degrees flexion but is still only a few degrees. In the transverse plane, internal and external rotation occur (Figure 21B). This motion is also dependent on how much the knee is flexed. At full extension, rotation is almost completely restricted by the interlocking femoral and tibial condyles. The range of motion increases with flexion, reaching a maximum at about 90 degrees flexion where external rotation ranges from 0 to about 45 degrees and internal rotation ranges from 0 to 30 degrees. Beyond 90 degrees of flexion the range of rotation decreases. Activity: Whilst sitting down, extend your knee joint and holding your thigh firmly try to abduct and adduct your knee, and then to internally and externally rotate your knee. Flex your knee joint to about 90 degrees and do the same. Is there any difference in the range of motion? To perform common daily activities, such as walking, standing up and sitting down, ascending and descending stairs, and squatting down to lift an object from the floor, requires a range of knee joint motion in the sagittal plane from full extension to about 115 degrees of flexion and about 10 degrees of rotation in the transverse plane. Unit 2 - Biomechanics of the Lower Limb 14 SAQ 9 (a) In which plane does the majority of knee motion occur? (b) How is the range of motion in the transverse plane dependent on the amount of flexion and extension? (c) During standing up how will the amount of motion in the sagittal plane be affected when the height of the chair is lowered? 2.3 Function of the Patella The most important function of the patella is to increase the lever arm of the quadriceps femoris muscle. It assists knee extension by increasing the lever arm of the quadriceps muscle force by displacing the quadriceps tendon. This function is illustrated in Figure 22 below, it shows a close-up of the knee joint whilst standing with the knee flexed. The quadriceps femoris provides the effort force required to maintain the knee joint’s position, overcoming the resistive force, the ground reaction force, produced by the weight of the body acting behind the knee. F R FIGURE 22. LEVER ARM PRODUCED BY THE PATELLA. The lever arm of the quadriceps femoris muscle (the effort lever) is dependent on the position of the patella which is in turn dependent on the amount of knee flexionextension. At full extension the quadriceps tendon is displaced anteriorly, lengthening the effort lever arm considerably. As the knee flexes the contribution of the patella to the length of the lever arm decreases as the patella sinks into the intercondylar notch. At full flexion, the patella is located in the intercondylar notch where it contributes little to the effort arm (Figure 23). FIGURE 23. THE CHANGE IN THE POSITION OF THE PATELLA AS THE KNEE FLEXES REDUCES THE PATELLA'S CONTRIBUTION TO THE EFFORT ARM. Unit 2 - Biomechanics of the Lower Limb 15 Activity: If you flex your knee beyond 90 degrees you should be able to feel the smooth anterior depression between the femoral condyles (the trochlea) just above the patella. If you slowly extend your knee you should be able to feel the patella rise up the trochlea. If the patella is removed (patellectomy), the lever arm is reduced (Figure 24). To compensate for this the force produced by the quadriceps muscle must increase considerably (by up to 30% at full extension) in order to provide the required turning moment. FIGURE 24. REDUCTION IN LEVER ARM AFTER A PATELLECTOMY. Clinical note: Severe fractures of the patella are treated by patellectomy (removal of the patella) when the fragments can not be accurately reassembled. If an irregular surface is left it will cause osteoarthritis in later life. SAQ 10 (a) Classify the lever system shown in Figure 22. (b) Is the quadriceps femoris muscle working at a mechanical advantage or a mechanical disadvantage? 2.4 Function of the Menisci The menisci act as force distributors and shock absorbers between the femur and the tibia. The menisci distribute the force over nearly the entire surface of the tibial plateau (Figure 25A). Since the force is distributed over a large area the stress in the articular cartilage and underlying bone tissue is small (remember stress is equal to the force divided by area). If the menisci are removed the force is no longer distributed but is concentrated in the area of contact between the tibia and femur (Figure 25B). This increases the stress in the joint tissues and will increase the likelihood of wear and joint damage. In fact there is approximately a three fold increase in stress when the menisci are removed. Unit 2 - Biomechanics of the Lower Limb 16 (A) (B) FIGURE 25. (A) WITH THE MENISCI INTACT THE FORCE IS WELL DISTRIBUTED MINIMISING THE STRESS (B) WITH THE MENISCI REMOVED THE STRESS IS INCREASED DRAMATICALLY. Clinical note: If the menisci are damaged they have no capacity to heal because there is only a blood supply to their outer edges. Tears in the menisci can obstruct the motion of the knee and cause it to jam. Injured knees with part or all of the menisci removed (a meniscectomy) may still function adequately but the articulating surfaces are more likely to be damaged and there is a significantly increased likelihood of the development of degenerative osteoarthritis. For this reason, if possible the menisci are preserved after injury. SAQ 11 (a) What are the two main functions of the menisci? (b) When the menisci are removed how does this affect the stress in the joint tissues? 2.5 Knee Joint Forces During Daily Activities As with the hip the knee joint forces are dependent on the weight of the subject and the amount of muscle activity. Generally, when there is little or no muscle activity the tibiofemoral joint force will be higher than the hip joint force since the knee must also support the weight of the thigh. However, when there is muscle activity the contribution of the weight of the thigh to the joint force becomes small in comparison to the large forces generated by the muscles. Typical peak joint forces are given in the table below for the tibiofemoral joint and the patellofemoral joint during various daily activities. Note that the joint forces presented are the peak joint forces during an activity. These peak joint forces are generally not sustained for very long. Also note that the patellofemoral joint forces are generally lower than the tibiofemoral joint forces. Tibiofemoral joint force (body weight) Patellofemoral joint force (body weight) Walking 3 to 5 0.5 to 1 Stair ascent 4 to 5 3 to 4 Stair descent 3 to 4 3 to 4 Standing up 3 to 7 3 to 4 SAQ 12 - What is the range of peak hip and knee joint forces during walking? Give a brief explanation for the difference between them. Unit 2 - Biomechanics of the Lower Limb 17 3. ANKLE AND FOOT 3.1 Ankle Joint The ankle joint is essential a hinge synovial joint formed by the distal ends of the tibia and fibula and the talus (Figure 26). It consists of three articulations: tibiotalar (between the tibia and the talus), the fibulotalar (between the fibula and the talus) and the distal tibiofibular (between the distal ends of the tibia and fibula). tibia fibula distal tibiofibular articulation tibiotalar articulation fibulotalar articulation talus FIGURE 26. THE ANKLE JOINT. The two distinctive bony prominences on the lateral and medial sides of the ankle joint are called the lateral malleolus and the medial malleolus respectively. The lateral malleolus is the distal end of the fibula and the medial malleolus is the distal end of the tibia. As with the hip joint the arrangement of the bones that form the ankle joint is intrinsically stable. However, because of the high loads that the ankle must withstand, additional stability is necessary. This is provided by the ligaments that surround the joint and to a smaller extent by the surrounding muscles. The three most important ligaments are the anterior inferior talofibular ligament, the medial ligament and the lateral ligament (Figure 27). anterior inferior talofibular ligament lateral ligament medial ligament FIGURE 27. THE LIGAMENTS OF THE ANKLE JOINT. Unit 2 - Biomechanics of the Lower Limb 18 ANKLE JOINT SAQ 13 (a) Name the bones that form the ankle joint. (b) How many articulations are there in the ankle joint? (c) Name the three main ligaments that stabilise the ankle joint? 3.2 Ankle Joint Motion The ankle joint is essentially a hinge joint with motion occurring primarily in the sagittal plane (Figure 28). The axis of rotation corresponds approximately to the line joining the lateral malleolus and the medial malleolus. Flexion of the ankle joint is termed dorsiflexion (toes move upwards) and extension is termed plantarflexion (toes move downwards - planting themselves into the ground). DORSIFLEXION PLANTARFLEXION axis of rotation 15° dorsiflexion 30° plantarflexion FIGURE 28. ANKLE JOINT MOTION. The range of motion varies widely among individuals but is usually around 45 degrees. This is made up of 10 to 20 degrees of dorsiflexion and 25 to 35 degrees of plantarflexion. During walking the ankle joint motion is around 10 to 15 degrees of dorsiflexion and around 15 to 20 degrees plantarflexion. SAQ 14 (a) What is dorsiflexion? (b) What is plantarflexion? Clinical Note: The most common ankle injury is a sprained ankle. It is partial tear of the anterior inferior talofibular ligament resulting from a sudden adduction of the foot whilst the ankle is plantarflexed. 3.3 The Foot The foot is a very complex structure made up of 26 bones, 57 synovial joints, and numerous ligaments and tendons. This complexity is required to fulfil its diverse functional requirements. It needs to adapt to a variety of ground surfaces and still Unit 2 - Biomechanics of the Lower Limb 19 FOOT maintain a stable and secure contact, it is required to distribute and absorb loads to avoid injury, and it must transmit loads between the ground and the rest of the body. The foot can be usefully considered to consist of three parts: the hindfoot, the midfoot and the forefoot (Figure 29). The hindfoot consists of the talus and the calcaneus (os calcis). The midfoot consists of the cuboid, medial, intermediate and lateral cuneiforms and the navicular. The forefoot consists of the metatarsals and phalanges. forefoot midfoot HINDFOOT MIDFOOT FOREFOOT hindfoot os calcis (calcaneus) phalanges metatarsals cuneiforms navicular cuboid talus FIGURE 29. THE BONES OF THE FOOT. SAQ 15 - What are the three parts of the foot called and which bones make up each part? 3.4 Subtalar Joint The subtalar joint is the articulation between the talus and the calcaneus. The joint has an oblique axis positioned at about 42 degrees to the plantar surface and 16 degrees medial to the mid-line of the foot (Figure 30). SUBTALAR JOINT talus os calcis (calcaneus) 42° mid-line of foot 16° (A) (B) FIGURE 30. THE AXIS OF ROTATION OF THE SUBTALAR JOINT. The subtalar joint allows the inversion and eversion of the foot (Figure 31). Inversion is the inward rotation of the foot so that the plantar surface (the underneath surface) faces medially (inwards). Eversion is the outward rotation of the foot so that the plantar surface faces laterally (externally). The subtalar joint can on average be inverted by about 20 degrees and everted by about 5 degrees. During walking the range of motion is around 6 degrees. Unit 2 - Biomechanics of the Lower Limb 20 INVERSION EVERSION (A) (B) 20° inversion 5° eversion FIGURE 31. (A) INVERSION OF THE FOOT (B) EVERSION OF THE FOOT. SAQ 16 (a) Name the bones that form the subtalar joint. (b) What movements occur at the subtalar joint? 3.6 The Arched Structure of the Foot The foot has a two-way arched structure formed from the bones of the foot and kept in place by strong ligaments (Figure 32). There are five longitudinal arches that extend from the calcaneus along the five sets of tarsals and metatarsals. The transverse arch runs across the foot. LONGITUDINAL ARCH TRANSVERSE ARCH medial longitudinal arch lateral longitudinal arch transverse arch FIGURE 32. ARCHES OF THE FOOT. The longitudinal arch is supported by the plantar fascia. The plantar fascia extends from the calcaneus to attach to the plantar aspect of the proximal phalanges. It is a heavy ligamentous structure that may only be elongated slightly when loaded. It functions as a cable between the heel and toes and as a shock absorber. During standing, the bones of the longitudinal arch and the plantar fascia function like a truss (Figure 33). The plantar fascia prevents the vertical force acting downwards at the ankle joint from collapsing the longitudinal arches. Unit 2 - Biomechanics of the Lower Limb 21 PLANTAR FASCIA plantar fascia FIGURE 33. TRUSS-LIKE ACTION OF THE PLANTAR FASCIA. When the toes are dorsiflexed the plantar fascia is put under tension and the two ends of the foot are drawn together raising the longitudinal arches (Figure 34). The bones of the foot are thus held together tightly and function as a single unit rather than as separate bones. FIGURE 34. ACTION OF THE PLANTAR FASCIA AS THE FOREFOOT DORSIFLEXES CAUSING THE LONGITUDINAL ARCH TO RISE. Activity: Place your foot flat on the ground and place your fingers under the medial arch of the foot. When you dorsiflex your toes you should be able to feel the plantar fascia tighten. SAQ 17 - Name the ligamentous structure which supports the longitudinal arches of the foot. Unit 2 - Biomechanics of the Lower Limb 22 4. THE BIOMECHANICS OF RECIPROCAL GAIT One of the principal functions of the lower limb is locomotion (walking and running). Here we will be examining the biomechanics of the gait (the manner or style of locomotion) commonly used for walking, termed reciprocal gait (Figure 35A). In reciprocal gait, the lower limbs are used alternatively to provide support and propulsion. Other gaits are usually only used when reciprocal gait is not possible. For example, someone who has broken their femur may use swing-through gait (Figure 35B). In swing-through gait, crutches are used for support and both legs swing through the crutches landing ahead of the crutches, the crutches are then advanced forward and the process is begun again. A well practised user of swing-through gait can get about twice as fast using it compared to reciprocal gait! RECIPROCAL GAIT (A) (B) FIGURE 35. (A) RECIPROCAL GAIT (B) SWING-THROUGH GAIT. 4.1 Gait Analysis A wide variety of parameters of gait can be studied. The ones chosen by the clinician, physiotherapist, prosthetist, orthotist or bioengineer will be dependent on the pathology of the patient and the aims of the examination. The clinical examination of the gait of a patient is called gait analysis. Gait analysis may be used for a wide variety of purposes. It may be used to determine the surgical intervention required to improve the gait of a child with cerebral palsy. It may be used to quantify the severity of a disorder or to determine the outcome of an operation such as in osteoarthritis and joint replacement. It may also be used to ensure the best alignment of an artificial leg to ensure that the gait of an amputee is as comfortable, as energy efficient and as cosmetically acceptable as possible. Gait analysis can be performed using a variety of techniques. An experienced examiner may simply watch the patient walking back and forth. However, if the patient is elderly or suffering from some disorder they may become tired very quickly. To avoid this a video recording may be used so that the examiner may replay the tape and even slow down the tape to make the observation easier. Both these techniques rely on the Unit 2 - Biomechanics of the Lower Limb 23 GAIT ANALYSIS experience of the examiner and neither gives any quantitative data which may be compared to data collected from able-bodied persons. Nowadays, gait laboratories equipped with motion analysis systems, force plates and electromyography equipment are commonly used. This equipment enables not only gait to be studied but also other common activities of daily living such as standing up and sitting down as well as movements performed in a variety of sporting activities. Most motion analysis systems use cameras that only see special markers which are placed over prominent parts of the patients body (Figure 36). Provided each marker is seen by two or more cameras the motion analysis system is able to calculate the position of each marker in three dimensions and using all the markers the movement of the patient can be reconstructed by computer. This enables the examiner to view the patient from any angle they wish, say from the side and the front at the same time, and to obtain quantitative data (such as the joint angles) which they can compare to a database of data collected from able-bodied persons. GAIT LABORATORIES MOTION ANALYSIS SYSTEMS FIGURE 36. MARKERS PLACED ON A PATIENT. Motion analysis systems are often integrated with force plates, which measure the ground reaction forces (see Section 4.4) and electromyography equipment which measure muscle activity. ELECTROMYOGRAPHY SAQ 18 (a) What is reciprocal gait? (b) What is gait analysis? (c) What type of equipment is contained in a gait laboratory? (d) What is a motion analysis system? 4.2 Gait Cycle To understand and analyse reciprocal gait the walking pattern is usually divided into a gait cycle (Figure 37). The gait cycle is equivalent to one stride which is equal to two Unit 2 - Biomechanics of the Lower Limb 24 GAIT CYCLE steps; one taken by each lower limb. It starts with the initial contact of one foot on the ground, termed heel contact, and ends with the next heel contact of the same foot. left toe off left left heel contact Time left swing phase double support right HEEL CONTACT left toe off left stance phase right single support double support right stance phase left single support right swing phase right heel contact right toe contact right heel contact FIGURE 37. THE GAIT CYCLE. During reciprocal gait each foot is in contact with the ground for part of the gait cycle, termed the stance phase, and for the rest of the cycle it loses contact with the ground, the swing phase. In walking there is a period of time when both feet are in touch with the ground, this is termed double support. As the speed of locomotion is increased the duration of double support decreases until eventually there is no period of double support. This is the transition from walking to running. During running there is a period when neither foot is in contact with the ground. (In a walking race, a competitor must always have at least one foot in contact with the ground, therefore, to achieve a faster speed they adopt a gait pattern which is slightly different from normal walking.) STANCE PHASE SWING PHASE DOUBLE SUPPORT Reciprocal gait is characterised by a number of events which occur sequentially during the gait cycle (Figure 38). These events are useful as landmarks when examining the gait of a person with a disorder which affects their gait. These events are: heel contact, foot flat, mid stance, heel off, toe off, and mid swing. The stance phase lasts from heel contact to toe off, and the swing phase lasts from toe off to the next heel strike. heel contact foot flat mid stance heel off stance phase toe off mid swing heel contact swing phase FIGURE 38. RECIPROCAL GAIT EVENTS (SHADED FOOT). All the events are present in the gait of an able-bodied person. However, one or two events may be missing, or the order that they occur may be changed, in the gait of a person with a disorder. For example, someone who has suffered a mild stroke or has weak dorsiflexor muscles may suffer from foot drop. In foot drop, the foot hangs down during the swing phase, so that the toes will make contact with the ground before the heel (Figure 39). Unit 2 - Biomechanics of the Lower Limb 25 FOOT DROP FIGURE 39. FOOT DROP. SAQ 19 (a) During reciprocal gait what defines the stance phase and the swing phase? (b) What is double support? (c) List the events that occur in reciprocal gait. 4.3 Range of Joint Motion The typical variation of lower limb joint angles during a complete gait cycle are shown in Figure 40. The angles shown are those in the sagittal plane where the majority of the motion occurs during reciprocal gait. The actual variation of the joint angles varies from person to person and also varies with speed, the ground surface (compare walking on sand and on concrete) and type of footwear (compare walking in slippers and in high heeled shoes). flexion 30 20 10 0 -10 -20 Hip 10 20 30 40 50 60 70 80 90 100 external flexion 70 60 50 40 30 20 10 0 0 dorsiflexion plantarflexion Knee 10 20 30 40 50 60 70 80 90 10 0 -10 -20 100 Ankle 0 10 20 30 40 50 60 70 80 90 100 percent of cycle heel contact toe off heel contact FIGURE 40. HIP, KNEE AND ANKLE ANGLES DURING ONE RECIPROCAL GAIT CYCLE. Unit 2 - Biomechanics of the Lower Limb 26 The range of motion at the hip joint varies from around 5 - 10 degrees extension to 30 40 degrees flexion. The peak amount of hip extension occurs shortly before toe off as the leg is left trailing behind. The peak amount of hip flexion occurs shortly after midswing to ensure a long step. The range of motion is greatest at the knee joint, where it varies from a few degrees of extension to around 70 degrees of flexion. The peak amount of knee flexion occurs during the swing phase as the knee is flexed to allow the foot to clear the ground as it swings pass the other limb. The range of motion at the ankle joint is less than at the hip and knee joints. It varies from around 15 degrees of plantarflexion (extension) to 10 degrees of dorsiflexion (flexion). There are two main peaks of plantarflexion; the first occurs at foot flat and the second shortly after toe off. The peak amount of dorsiflexion occurs at around heel off as the foot is left trailing behind the rest of the body. SAQ 20 (a) Which lower limb joint has the greatest range of motion during reciprocal gait? (b) When does the peak amount of dorsiflexion occur during the gait cycle? 4.4 Ground Reaction Forces When the foot is in contact with the ground it exerts a force against the ground. The ground does not give way but exerts an equal and opposite force (Newton’s third law) which is called the ground reaction force. In gait analysis, the ground reaction force is measured using a force plate (also called a force platform) as the patient steps on the plate as they walk along (Figure 41). Note that the top surface of the plate is level with the surrounding floor and that only one foot is placed on the plate. FIGURE 41. A FORCE PLATE. The magnitude and direction of the ground reaction force varies during the stance phase of gait. Figure 42 shows this variation of the ground reaction force in the sagittal plane at different points of the gait cycle, in what has appropriately become known as a butterfly diagram. Unit 2 - Biomechanics of the Lower Limb 27 GROUND REACTION FORCE FORCE PLATE FIGURE 42. GROUND REACTION VECTOR IN THE SAGITTAL PLANE. A typical example of the vertical force measured using two force platforms (one for each foot) is shown in Figure 43. The vertical force is characterised by a double hump, with both peaks being greater than body weight. The first peak is due the deceleration of body mass as the weight is transferred on to the foot and the second due foot pushing off the ground. body weight time heel contact toe off FIGURE 43. VERTICAL GROUND REACTION FORCE AGAINST TIME. SAQ 21 - What is a force plate used to measure? 4.5 Joint Forces and Moments The forces and moments acting at the joints during walking can be calculated using biomechanics and data collected from the standard equipment found in a gait laboratory. The position of the body is measured using a motion analysis system. The external forces and moments acting on the foot are measured using a force plate. The weight of each body segment may be determined from the patient’s own weight and standard anthropometric data. The forces exerted by the muscles and the tension in the ligaments can be estimated using electromyography data and mathematical models. Unit 2 - Biomechanics of the Lower Limb 28 Typical internal joint moments calculated in this manner are shown in Figure 44. The graph shows the internal moments generated by the muscles. There are a number of points of particular interest. At the hip, after heel contact, there is a positive extension moment produced by the hip extensors to prevent the upper body falling forward. At the knee, just after heel contact, there is a small flexion moment as the hamstrings contract to prevent hyperextension of the knee. This changes to an extension moment as the quadriceps contract to prevent the knee from buckling. At the ankle joint the plantarflexion moment increases to a peak just before toe off as the triceps surae contracts to push the foot up and off the ground. extension flexion extension flexion plantarflexion 10 20 30 40 50 60 70 80 90 100 percent of cycle heel contact toe off heel contact FIGURE 44. INTERNAL JOINT MOMENTS OVER THE GAIT CYCLE. SAQ 22 - Why do the hamstrings contract at heel contact? Unit 2 - Biomechanics of the Lower Limb 29 SUMMARY In this unit you have been introduced to the biomechanics of the lower limb. Mechanically the lower limb is well adapted to its functions of weight bearing and locomotion. This is particularly evident at the hip where the joint combines a large range of motion with considerable stability. The knee joint is more complex and less stable than the hip joint, having two articulations and relying on the menisci and ligaments for stability. The knee joint motion is quite complex but is essentially like a hinge with the patella increasing the lever arm of the knee extensor muscles. The ankle joint is also complex, having three articulations, but it is intrinsically stable. Its motion can also be likened to a hinge producing dorsiflexion and plantarflexion. The foot is a very complex structure with quite diverse functional requirements. Within the foot, the subtalar joint allows inversion and eversion and the plantar fascia helps to maintain the five longitudinal arches. Reciprocal gait is the most commonly employed manner of walking. Using gait analysis it is possible to quantify the many features of gait with the aim to improve the treatment of patients with locomotor disorders. Unit 2 - Biomechanics of the Lower Limb 30 SAQ ANSWERS SAQ 1 (a) The three segments of the lower limb are the thigh, leg and foot. (b) The three major joints of the lower limb are the hip, knee and ankle. (c) The two main functions of the joints of the lower limb are movement and weight bearing. SAQ 2 (a) The hip joint is a ball-and-socket type synovial joint. (b) Synovial fluid lubricates the joint and provides nutrients to the articular cartilage. (c) The hip joint is intrinsically stable due to its shape, its strong joint capsule and the surrounding ligaments and muscles. SAQ 3 (a) The greatest range of hip joint motion occurs in the sagittal plane. (b) Typically around 110° of flexion-extension, 20° of abduction-adduction and 15° of rotation is required to stand up and sit down. SAQ 4 The abductor muscle force is 1880 N and the subject's total body weight is 800 N thus the magnitude of the abductor muscle force is equal to 2.4 times the subject's total body weight. SAQ 5 (a) Muscle activity generally increases the magnitude of the joint forces by pulling the two sides of the joint together. During unilateral stance the contraction of the hip joint abductors acts in this way, causing a large increase in the joint force as compared to bilateral stance when there is usually no muscle activity. (b) The magnitude of the hip joint force is equal to 0.4 total body weight during bilateral stance, and 3.2 total body weight during unilateral stance. SAQ 6 (a) The two articulations which comprise the knee joint are the tibiofemoral and the patellofemoral. (b) The patella is a sesamoid bone. SAQ 7 The stability of the knee joint is derived from its ligaments, in particular the cruciate and collateral. Unit 2 - Biomechanics of the Lower Limb 31 SAQ 8 The knee joint's centre of rotation in the sagittal plane follows a semicircular path as it flexed and extended. SAQ 9 (a) The majority of knee joint motion occurs in the sagittal plane. (b) The range of motion in the transverse plane is almost zero at full extension, increases with flexion to a maximum at around 90° of flexion and reduces with further flexion. (c) If the height of the chair is lowered then the range of knee joint motion required in the sagittal plane will be increased since the knee will start at a position of greater flexion. SAQ 10 (a) The lever system shown in Figure 22 it has its fulcrum located between the effort force and resistance force, it is therefore a first class lever. (b) The lever arm for the quadriceps femoris muscle is less than that for the resistance force, it is therefore acting at a mechanical disadvantage. SAQ 11 (a) The two main functions of the menisci are to distribute the force more evenly and to absorb large force peaks. (b) When the menisci are removed the stress in the joint tissues is increased by approximately three times. SAQ 12 During walking, the peak joint forces at the hip range from 3 to 7 body weight and at the knee from 3 to 5 body weight. The peak joint force is generally lower at the knee than at the hip, as the knee must also support the mass of the thigh this phenomenon must be due to higher muscle forces at the hip. SAQ 13 (a) The bones that form the ankle joint are the tibia, fibula and talus. (b) The are three articulations in the ankle joint. (c) The three main ligaments that stabilise the ankle joint are the anterior inferior talofibular, the medial and lateral ligaments. SAQ 14 (a) Dorsiflexion is flexion of the ankle joint - toes move upwards. (b) Plantarflexion is extension of the ankle joint - toes move downwards. SAQ 15 The three parts of the foot are the forefoot, the midfoot and the hindfoot. The forefoot is made up of the metatarsals and phalanges. The midfoot is made up Unit 2 - Biomechanics of the Lower Limb 32 of the cuneiforms, the cuboid and the navicular. The hindfoot is made up of the talus and calcaneus. SAQ 16 (a) The bones that form the subtalar joint are the talus and the calcaneus. (b) Inversion and eversion occur at the subtalar joint. SAQ 17 The ligamentous structure which supports the longitudinal arches of the foot is called the plantar fascia. SAQ 18 (a) Reciprocal gait is the gait most commonly used for walking. During reciprocal gait the lower limbs are used alternatively to provide support and propulsion. (b) Gait analysis is the examination of gait. (c) There are three main pieces of equipment found in a gait laboratory. They are a motion analysis system, force plates and electromyography equipment. (d) A motion analysis system is a device which records the motion of markers placed on a patient, thus allowing the patient's movements to be reconstructed and observed on a computer. SAQ 19 (a) During reciprocal gait the stance phase and the swing phase are both defined by the two events: heel contact and toe off. (b) Double support is the period during the gait cycle when both feet are in contact with the ground. (c) The events that occur in reciprocal gait are: heel contact, foot flat, mid stance, heel off, toe off and mid swing. SAQ 20 (a) The knee joint is the lower limb joint with the greatest range of motion during reciprocal gait. (b) The peak amount of dorsiflexion occurs at around heel off. SAQ 21 A force plate is used to measure the ground reaction force exerted on the foot during the stance phase of gait. SAQ 22 The hamstrings contract slightly at heel contact to prevent the hyperextension of the knee. Unit 2 - Biomechanics of the Lower Limb 33