Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
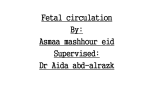
Transition and Normal Newborn Care Monica L. Scrudder, RNC-NIC, BSN, MSN Franciscan Health System Regional Nurse Educator, Nursery Services Objectives • Identify primary features of fetal circulation. • Identify physiological changes that occur at birth in the newborn’s transition to extrauterine homeostasis. • Identify routine care for the newborn in the transition period. • Identify signs and symptoms of common problems in the transition period. • Identify nursing intervention that promote parental bonding. What Is Transition??? The Transition Period • Birth to 6 hours of age • Physiological change from placental support to self-maintenance • Fetus prepares for transition over the course of gestation • Transition depends on gestational age and quality of placental support The Cardiac Puzzle Anatomy and Physiology • Placental Fetal Circulation • Blood follows the path of least resistance • Low pulmonary blood flow (only 8-10% of right ventricular output secondary to high pulmonary vascular resistance The Fetal Circulation Ductus Venosus Foramen Ovale Ductus Arteriosis Fetal Lungs Fetal Metabolism and Hematology • Glucose – Fetal concentrations 70-80% of maternal glucose concentrations • Glycogen – Large glycogen stores provide large energy reserves to sustain newborn through transition period • Brown Fat – Unique to newborn – Metabolized for heat Cardiopulmonary Adaptation at Birth Cardiovascular Adaptations At Birth • Umbilical cord is clamped. • Three major shunts functionally close during transition – Ductus Arteriosis – Foramen Ovale – Ductus Venosus Pulmonary Adaptation At Birth • Stimuli for initiating respiration – Mild hypercapnia, hypoxia and acidosis – Light, noise, touch – Thoracic squeeze during vaginal delivery • Empties approximately 1/3 of fetal lung fluid First Breath • Air enters lungs at 2x normal pressure – 40-80 cm H2O • Pulmonary vessels vasodilate in response to increased oxygen – Pulmonary vascular resistance decreases – Pulmonary blood flow increases Continued Pulmonary Adaptations • Pulmonary vascular resistance (PVR) decreases to reach adult levels at 2-3 weeks of age • Lung compliance improves Measurements • Apgar score – Done at 1 minute and 5 minutes of age – If apgar less than 7 at 5 minutes of age, continue every 5 minutes until greater than 7 for maximum of 20 minutes The Apgar Score Sign 0 1 2 Heart rate Absent Slow (<100 bpm) > 100 bpm Respirations Absent Weak cry, Hypo-ventilation Good, strong cry Muscle Tone Limp Some flexion Active motion Reflex Irritability No response Grimace Cough or sneeze Color Blue or pale Body pink, Extremities blue Completely pink Assessment Findings During Transition • • • • • • • • Head circumference, length, weight Gestational age assessment Skin Head Respiratory assessment Cardiac assessment Gastrointestinal assessment Extremities Medications in Transition • Erythromycin Ointment • Vitamin K (AquaMEPHYTON) • Hepatitis B vaccine/Hepatitis B Immunoglobulin Glucose Needs Feeding Contraindications to Feeding • • • • Cyanosis Shock or asphyxia Increased work of breathing Ongoing oxygen requirement Routine Care Considerations AAP/ACOG/AWHONN Guidelines • • • • • • Proper identification of newborn Initial assessment within 2 hours of birth Develop a plan of care Document observations at least every 30 minutes until stable for 2 hours Prophylactic eye care within 1 hour of birth Primary health care provider – Perform initial physical exam no later than 24 hours of birth – Perform physical exam within 24 hours before discharge • • • Document daily weight Perform metabolic screening Instruct parent in care of infant Guidelines (Cont) • • • • • • Implement emergency measures, including resuscitation, when necessary using such programs as the Neonatal Resuscitation Program Observe parent-infant interactions Identify with parent(s) the appropriate facility for follow-up Inform parent(s) of importance of immunizations Identify high-risk mothers Evaluate home environment Nursing Considerations • Observations must be documented every 2 hours according to the State of Washington. – Follow hospital policy regarding this guideline. • • • • • Vital sign routine Daily weight Physician notification Timing of metabolic screening Specific teaching issues for population Nursing Observations • • • • • • • • Cardiac and Respiratory Status Feeding Temperature Color Tone Activity Output Parent-infant bonding Parent-Infant Bonding • • • • • Bonding Attachment “En face” “Parentese” Red Flags Assess Parenting Styles and Abilities • • • • • • • • Parents’ level of knowledge Family’s communication Parental expectations Infant’s responses to parenting activities Parental feelings about self and infant Parental support Cultural beliefs Potential need for referral Routine Care and Documentation • • • • • • • • • • Documentation of birth Measurements Medications Physical assessment Abduction prevention Bathing/Hygiene Cord Care Feeding assessment Metabolic screening Elimination Discharge Criteria • • • • • • Feedings Discharge weight Metabolic screening Birth certificate worksheet/paternity papers Teaching documented Hearing screening Discharge Teaching • • • • Begins on admission Assess Mother’s readiness to learn Assess Father’s involvement Involve Grandparents, siblings, and other significant people Teaching Documentation • • • • • • • • • • Thermoregulation Holding and Positioning Hygiene Feeding Bulb syringe Choking Elimination Circumcision Care Safety When to Call the Physician References • Askin, DF. (2002) Complications in the Transition from Fetal to Neonatal Life. JOGNN 31(3): 318-27 • Buschbach, D., Schaub-Bordeaux, M. (2002) Newborn Physiological and Developmental Transitions: Integrating Key Components of Perinatal and Neonatal Assessment. Association of Women’s Health, Obstetric and Neonatal Nurses. • Kenner, C., Wright-Lott, J. (2003) Comprehensive Neonatal Nursing: A Physiological Perspective. Philadelphia:Saunders • Sansoucie DA, Cavaliere, TA. (1997) Transition from Fetal to Extrauterine Circulation. Neonatal Network, 16(2):5-12 • Verklan,TM, Walden, M., editors (2004) Core Curriculum for Neonatal Intensive Care Nursing (3rd ed.) St. Louis:Elsevier References (2) • http://www.cayugacc.edu/people/web_pages/greer/biol204/heart 4/heart4.html • http://dic.academic.ru/pictures/enwiki/80/Pate nt_ductus_arteriosus.jpg • http://www.007b.com/breastfeeding_pictures. php • http://pregnancy.about.com/od/newbornbabie s/ig/Newborn-Photo-Gallery/index.01.htm