Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
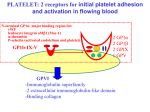
Cardiovascular System Lecture IV RED BLOOD CELL Red blood cells are the most common type of blood cell and are the vertebrate body's principal means of delivering oxygen from the lungs or gills to body tissues via the blood. Red blood cells are also known as RBCs or erythrocytes (from Greek erythros for "red" and kytos for "hollow," nowadays translated as "cell"). A schistocyte is a red blood cell undergoing fragmentation, or a fragmented part of a red blood cell. Blood diseases involving the red blood cells include: Anemias (or anemias) are diseases characterized by low oxygen transport capacity of the blood, because of low red cell count or some abnormality of the red blood cells or the hemoglobin. Iron deficiency anemia is the most common anemia; it occurs when the dietary intake or absorption of iron is insufficient, and hemoglobin, which contains iron, cannot be formed Sickle-cell disease is a genetic disease, which leads to mis-shaped red blood cells. Thalassemia is a genetic disease that results in the production of abnormal hemoglobin molecules. Spherocytosis is a genetic disease that causes a defect in the red blood cell's cytoskeleton, causing the RBCs to be small, sphere-shaped, and fragile instead of donut-shaped and flexible. Pernicious anemia is an autoimmune disease wherein the body lacks intrinsic factor, required to absorb vitamin B12 from food. Vitamin B12 is needed for the production of hemoglobin. Aplastic anemia is caused by the inability of the bone marrow to produce blood cells. Hemolysis is the general term for excessive breakdown of red blood cells. It can have several causes. The malaria parasite spends part of its life-cycle in red blood cells, feeds on their hemoglobin and then breaks them apart, causing fever. Both sickle-cell disease and thalassemia are more common in malaria areas, because these mutations convey some protection against the parasite. Polycythemias (or erythrocytoses) are diseases characterized by a surplus of red blood cells. The increased viscosity of the blood can cause a number of symptoms. In polycythemia vera the increased number of red blood cells results from an abnormality in the bone marrow. Several blood tests involve red blood cells, including the RBC count (the number of red blood cells per volume of blood) and the hematocrit (percentage of blood volume occupied by red blood cells). The blood type needs to be determined to prepare for a blood transfusion or an organ transplantation. WHITE BLOOD CELL White blood cells (also called leukocytes or immune cells) are a component of blood. They help to defend the body against infectious disease and foreign materials as part of the immune system. There are normally between 4x109 and 11x109 white blood cells in a litre of healthy adult blood - about 7 000 to 25 000 white blood cells per drop. In conditions such as leukemia this may rise to as many as 50 000 white blood cells in a single drop of blood. As well as in the blood, white cells are also found in large numbers in the lymphatic system, the spleen, and in other body tissues. There are three major types of white blood cells. Granulocytes Granulocytes are a category of white blood cells, characterized by the fact that all types have differently staining granules in their cytoplasm on light microscopy. There are three types of granulocytes: neutrophils, basophils, and eosinophils (named according to their staining properties). Lymphocytes Lymphocytes are much more common in the lymphatic system, and include the so-called "killer T-cells". The blood has three types of lymphocytes: B cells, T cells and natural killer cells. B cells make antibodies that bind to pathogens to enable their destruction. CD4+ (helper) T cells co-ordinate the immune response (they are what becomes defective in an HIV infection). CD8+ (cytotoxic) T cells and natural killer cells are able to kill cells of the body that are infected by a virus. Monocytes Monocytes share the 'vacuum cleaner' function of neutrophils, but are much longer lived as they have an additional role. They present pieces of pathogens to T cells so that the pathogens may be recognized again and killed, or so that an antibody response may be mounted. Monocytes are also known as macrophages after they leave the bloodstream and enter tissue. Diseases Leukopenia is a disease symptom defined as a lower than normal number of white blood cells in the blood. Leukocytosis refers to an increase in the number of white blood cells in the blood. Leukemia and lymphoma are two types of cancer in which white blood cells multiply out of control. Other tissue cells Histiocytes, found in the lymphatic system and other body tissues, but not normally in blood: Macrophages Dendritic cells Mast cells PLATELETS Platelets or thrombocytes are the blood cell fragments that are involved in the cellular mechanisms that lead to the formation of blood clots. Low levels or dysfunction predisposes for bleeding, while high levels - although usually asymptomatic - may increase the risk of thrombosis. Production Platelets are produced in the bone marrow; the progenitor cell for platelets is the megakaryocyte. This large, multinucleated cell sheds platelets into the circulation. Thrombopoietin (c-mpl ligand) is a hormone, mainly produced by the liver, that stimulates platelet production. It is bound to circulating platelets; if platelet levels are adequate, serum levels remain low. If the platelet count is decreased, more thrombopoietin circulates freely and increases marrow production. Circulation The circulating life of a platelet is 9-10 days. After this it is sequestered in the spleen. Decreased function (or absence) of the spleen may increase platelet counts, while hypersplenism (overactivity of the spleen, e.g. in Gaucher's disease or leukemia) may lead to increased elimination and hence low platelet counts. Function Platelets are activated when brought into contact with collagen (which is exposed when the endothelial blood vessel lining is damaged), thrombin (primarily through PAR-1), ADP, with receptors expressed on white blood cells or the endothelial cells of the blood vessels, among other activators. Once activated, they release a number of different coagulation factors and platelet activating factors, they also provide a catalytic phospholipid surface (with the charge provided by phosphatidylserine and phosphatidylethanolamine) for the tenase and prothrombinase complexes. The platelets adhere to each other via adhesion receptors or integrins, and to the endothelial cells in the wall of the blood vessel forming a haemostatic plug in conjunction with fibrin. The high concentration of myosin and actin filaments in platelets are stimulated to contract during aggregation, further reinforcing the plug. The most common platelet adhesion receptor is glycoprotein (GP) IIb/IIIa this is a calcium dependent receptor for fibrinogen, fibronectin, vitronectin, thrombospondin and von Willebrand factor (vWF). Other receptors include GPIb-V-IX complex (vWF) and GPVI (collagen) Activators There are many known platelet activators. They include 1. Collagen, especially with von Willebrand factor which is exposed when endothelial blood vessel lining is damaged and binds to GPVI on the platelet, 2. thrombin primarily through cleavage of the extracellular domain of PAR1 and PAR4, 3. Thromboxane A2 (TxA2) which binds to TP, 4. ADP through creation of TxA2, and it can be blocked by conversion of ADP to cAMP, 5. Human neutrophil elastase (HNE) cleaves the αIIbβ3 integrin on the platelet surface, 6. P-selectin which binds to PSGL-1 on endothelial cells and white blood cells, and 7. Convulxin (a purified protein from snake venom) which binds to GPVI. Inhibitors Prostacyclin opposes the actions of Thromboxane A2 Nitric oxide Clotting factors II, IX, X, XI, XII Nucleotidases by breaking down ADP Role in disease High and low counts A normal platelet count in a healthy person is between 150 and 400 (x 109/L of blood). Both thrombocytopenia (or thrombopenia) and thrombocytosis may present with coagulation problems. Generally, low platelet counts increase bleeding risks (although there are exceptions, e.g. Immune heparin-induced thrombocytopenia) and thrombocytosis (high counts) may lead to thrombosis (although this is mainly when the elevated count is due to myeloproliferative disorder). Low platelet counts are generally not corrected by transfusion unless the patient is bleeding or the count has fallen below 5 (x 109/L); it is contraindicated in thrombotic thrombocytopenic purpura (TTP) as it fuels the coagulopathy. In patients having surgery, a level below 50 (x 109/L) is associated with abnormal surgical bleeding, and regional anesthetic procedures such as epidurals are avoided for levels below 80-100. Note however that the actual platelet count is only part of the story, since they may not all be functioning normally. For example, aspirin irreversibly prevents platelets from working correctly and so normal hemostasis may not return until the aspirin is ceased and the affected platelets have been replaced by new ones, which may take over a week. Diseases Disorders leading to a reduced platelet count: Thrombocytopenia Idiopathic thrombocytopenic purpura Thrombotic thrombocytopenic purpura Drug-induced thrombocytopenia, e.g. heparin-induced thrombocytopenia (HIT) Gaucher's disease Aplastic anemia Disorders leading to platelet dysfunction or reduced count: HELLP syndrome Hemolytic-uremic syndrome Chemotherapy Disorders featuring an elevated count: Thrombocytosis, including benign essential thrombocytosis (elevated counts, either reactive or as an expression of myeloproliferative disease); may feature dysfunctional platelets Disorders of platelet adhesion or aggregation: Bernard-Soulier syndrome Glanzmann's thrombasthenia Scott's syndrome von Willebrand disease Disorders of platelet metabolism Decreased cyclooxygenase activity, induced or congenital Storage pool defects, acquired or congenital Transfusion Platelets are separated from donated blood using an apheresis blood separator. This is necessary because platelets will not survive at the low temperatures used to store red blood cells, so they must be stored separately using porous storage bags that allow oxygen to flow in and carbon dioxide to flow out. Typical storage is between 20 and 24 °C and continuously agitated to promote gas exchange. Because of the higher risks of bacterial growth at this temperature, platelets are generally only stored for up to 5 days. A bag of platelets can be separated from multiple bags of whole blood or from a single donor connected to the separator for less than two hours. By drawing and returning blood repeatedly, a bag of high quality platelets can be prepared in about 90 minutes. Platelets collected from a single donor can reduce the infection rates of blood-transmitted diseases. People with few platelets or platelets that are dysfunctional may benefit from a platelet transfusion, however patients with autoimmune disorders that affect platelets may not. Neutrophil granulocytes Neutrophil granulocytes, generally referred to as neutrophils, are a class of white blood cells and are part of the immune system. Neutrophils are active phagocytes, capable of only one phagocytic event, expending all of their glucose reserves in an extremely vigorous respiratory burst. Low neutrophil granulocyte counts are termed "neutropenia". This can be congenital (genetic disorder) or due to acquired factors. It can also be a side-effect of medication, including chemotherapy. Eosinophil granulocyte Eosinophil granulocytes, commonly referred to as eosinophils (or less commonly as acidophils), are white blood cells that are responsible for combating infection by parasites in the body. Eosinophils make up about 2.3% of the all white blood cells, and are about 10-12 micrometers in size. Eosinophils play a role in fighting viral infections, which is evident from the abundance of RNAses they contain within their granules. Eosinophils also play a role in the allergic response, and in fibrin removal in inflammation. Eosinophils are considered the main effector cells in asthma pathogenesis and are associated with disease severity. Basophil granulocyte Basophils are the least common of the granulocytes, representing about 1% of circulating leukocytes. Basophils tend to appear in specific kinds of inflammatory reactions, particularly those that cause allergic symptoms. All text of this article available under the terms of the GNU Free Documentation License (see Copyrights for details).