Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac surgery wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
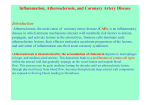
Section 7 500 Deaths in thousands Cardiovascular System 806 Problems of Oxygenation: Perfusion 493,623 Males 433,825 Females 400 300 268,503 288,768 200 64,103 69,257 100 41,877 60,713 38,948 34,301 0 A B C A Total CVD (Preliminary) B Cancer C Accidents D E A B D E F D Chronic Lower Respiratory Diseases E Diabetes Mellitus F Alzheimer’s Disease FIG. 34-1 Leading causes of death for all men and women. CVD, Cardiovascular disease. CORONARY ARTERY DISEASE Coronary artery disease is a type of blood vessel disorder that is included in the general category of atherosclerosis. The term atherosclerosis is derived from two Greek words: athere, meaning “fatty mush,” and skleros, meaning “hard.” This combination indicates that atherosclerosis begins as soft deposits of fat that harden with age. Atherosclerosis is often referred to as “hardening of the arteries.” Although this condition can occur in any artery in the body, the atheromas (fatty deposits) have a preference for the coronary arteries. Arteriosclerotic heart disease, cardiovascular heart disease, ischemic heart disease, coronary heart disease, and CAD are all terms used to describe this disease process. Etiology and Pathophysiology Atherosclerosis is the major cause of CAD. It is characterized by a focal deposit of cholesterol and lipids, primarily within the intimal wall of the artery. The genesis of plaque formation is the result of complex interactions between the components of the blood and the elements forming the vascular wall.2 Inflammation and endothelial injury play a central role in the development of atherosclerosis. Intact normal endothelium is more than a simple barrier between the vessel wall and the lumen of the vessel. Normally, it is nonreactive to platelets and leukocytes, as well as coagulation, fibrinolytic, and complement factors. However, the endothelial lin- ing can be injured as a result of tobacco use, hyperlipidemia, hypertension, diabetes, hyperhomocysteinemia, and infection (e.g., Chlamydia pneumoniae, herpes) causing a local inflammatory response3,4 (Fig. 34-2, A). C-reactive protein (CRP), a nonspecific marker of inflammation, is increased in many patients with CAD. Chronic exposure to even minor elevations of CRP can trigger the rupture of plaques and promote the oxidation of low-density lipoprotein (LDL) cholesterol, leading to increased uptake by macrophages in the endothelial lining.5,6 Developmental Stages. CAD is a progressive disease that takes many years to develop. When it becomes symptomatic, the disease process is usually well advanced. The stages of development in atherosclerosis are (1) fatty streak, (2) fibrous plaque resulting from smooth muscle cell proliferation, and (3) complicated lesion. Fatty Streak. Fatty streaks, the earliest lesions of atherosclerosis, are characterized by lipid-filled smooth muscle cells.2 As streaks of fat develop within the smooth muscle cells, a yellow tinge appears. Fatty streaks can be observed in the coronary arteries by age 15 and involve an increasing amount of surface area as the patient ages. It is generally believed that treatment that lowers LDL cholesterol may reverse this process4 (Fig. 34-2, B). Fibrous Plaque. The fibrous plaque stage is the beginning of progressive changes in the endothelium of the arterial wall. These changes can appear in the coronary arteries by age 30 and increase with age. Normally the endothelium repairs itself immediately, but in the person with CAD the endothelium is not rapidly replaced, allowing LDLs and growth factors from platelets to stimulate smooth muscle proliferation and thickening of the arterial wall. Once endothelial injury has occurred, lipoproteins (carrier proteins within the bloodstream) transport cholesterol and other lipids into the arterial intima. The fatty streak is eventually covered by collagen forming a fibrous plaque that appears grayish or whitish.2,4 These plaques can form on one portion of the artery or in a circular fashion involving the entire lumen. The borders can be smooth or irregular with rough, jagged edges.2 The result is a narrowing of the vessel lumen and a reduction in blood flow to the distal tissues (Fig. 34-2, C). Complicated Lesion. The final stage in the development of the atherosclerotic lesion is the most dangerous. As the fibrous plaque grows, continued inflammation can result in plaque instability, ulceration, and rupture.4 Once the integrity of the artery’s inner wall has become compromised, platelets accumulate in large numbers, leading to a thrombus. The thrombus may adhere to the wall of the GENDER DIFFERENCES Coronary Artery Disease Men Women • • • • • • Men tend to manifest CAD 10-15 years earlier than women. Initial cardiac event for men is more often MI than angina. Men have a higher incidence of left ventricular hypertrophy than women. • • • CAD causes more deaths in women than in men. Initial cardiac event for women is more often angina than MI. Women with the long Q-T syndrome have an increased incidence of sudden cardiac death compared to men with the same disorder. Before menopause, women have higher HDL cholesterol levels and lower LDL cholesterol levels than men. After menopause, LDL levels increase. Women complain of palpitations more frequently than men. CAD, Coronary artery disease; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MI, myocardial infarction. Ch34-A03690_805-843.indd 806 8/6/06 9:38:01 AM