Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
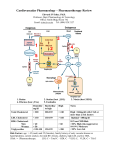
Infark Miokard Akut (IMA) Mohammad Saifur Rohman, dr.SpJP, PhD.FICA Outlines Anatomy of coronary artery Coronary artery disease : atherosclerosis Progression of CAD IMA Diagnosing IMA IMA Treatment Major components Muscle; contractile apparatus Nerve; conducting system and innervation Vessel; Supporting oxygen from the blood Extra cellular matrix Endocardium; valves Pericardium Etc. Coronary Arteries Coronary arteries branch off at base of aorta & supply blood to the electrical conduction system & myocardium. 3 main arteries: RCA LCA Circumflex Coronary Arteries Originates from the aorta just beyond the aortic valve • Coronary blood flow to the myocardium occurs primarily during diastole * To maintain adequate blood flow through the coronaries, mean arterial pressure (MAP) must be at least 60 mmHg • Coronary Arteries • Left main coronary artery (LCA) - Left anterior descending artery (LAD) >descends toward the anterior wall & apex of LV > supplies LV, ventricular septum, chordae, papillary muscle & RV - Left circumflex artery (LXA) > descends toward the lateral wall of LV & apex > supplies LA, lateral & posterior LV surfaces *45% supplies SA node Coronary Arteries LCA Branches into LAD & L Circumflex Left Anterior Descending Anterior wall of LV & anterior 2/3 septum RBB & part of LBB LA Circumflex Supplies AV node in 10% hearts SA node in 45% hearts Posterior surface of LV Coronary Arteries Right main coronary artery (RCA) - descends toward the apex of RV - supplies the RA, RV, & inferior portions of LV Coronary Arteries RCA Supplies SA node in 55% of hearts AV node in 90% hearts RA & RV heart muscle Inferior wall of LV Posterior 1/3 of intraventricular septum In 85% of hearts, RCA provides the posterior descending branch. Atherosclerosis Disease of cardiovascular system affecting vessel wall. It leads to the narrowing of arteries or complete blockage. Its main components are endothelial disfunction, lipid deposition, inflammatory reaction in the vascular wall. Remodeling of vessel wall. The process of atherogenesis – an overview Risk Factors Smoking Hypertension Obesity DIABETES Family history: Man < 55 yo Women < 65 yo CV Prevention Risk factors for CVD Modifiable – Smoking – Dyslipidaemia • raised LDL cholesterol • low HDL cholesterol • raised triglyceride – Raised blood pressure – Diabetes mellitus – Obesity – Dietary factors – Thrombogenic factors – Lack of exercise – Excess alcohol consumption Non-modifiable – – – – Personal history of CVD Family history of CVD Age Gender Levels of risk associated with smoking, hypertension and hypercholesterolaemia Hypertension (SBP 195 mmHg) x3 x9 X4.5 x16 X1.6 Smoking x6 x4 Serum cholesterol level (8.5 mmol/L, 330 mg/dl) (Adapted from Poulter et al, 1993) The development of atherosclerosis The key event – damage to the endothelium caused by excess of lipoproteins, hypertension, diabetes, components of cigarette smoke. Endothelium becomes more permeable to lipoproteins. Lipoproteins move below the endothelial layer (to intima). Endothelium loses its cell-repelent quality. Inflammatory cells move into the vascular wall. Triggers for inflammation in atherosclerosis LDL retained in the intima (in part by binding to proteoglycan) undergoes oxidative modification. Lipid hydroperoxides, lysophospholipides, carbonyl compounds localize in the lipid fraction. Oxygen free-radicals inactivate NO rapidly. NO + superoxide (O2.-) peroxynitrite (ONOO-). NO has no longer vasoprotective function. The process of atherogenesis Lipid entry into the arterial wall is a key process in atherogenesis. Hypercholesterolemia – factor for VCAM-1 and MCP-1 induction. LDL and VLDL are most atherogenic, enter vascular wall more easily. LDL – in plasma are protected against oxidation by vit. E, ubiquinon, plasma antioxidants (b-carotene, vit. C). Out of plasma, LDL phospholipides and fatty acids oxidize. The process of atherogenesis Activated macrophages produce enzymes – lipoxygenases, myeloperoxidase, NADPH oxidase ROS Oxidized LDL are cytotoxic to endothelial cells, mitogenic for macrophages. Oxidized LDL apolipoprotein apoB100 bind to the scavenger receptor. Scavenger receptors are not subjected to regulation by intracellular cholesterol level. Macrophages take up oxidized LDL, overload with lipids. The process of atherogenesis Foam cells ruptured (apoptosis). Lipid release to intima and their acumulation becomes centre of atherosclerotic plaques. • The lipid center and fibrous cap are the main parts of a mature atherosclerotic plaque. • Plaque emerges from the structurally changed vascular wall. • So-called vulnerable plaque ruptures easily. •The thrombus formed at the rupture site. The process of atherogenesis Morphologic stages: Type I – Fatty dots - Foam cells Type II – Fatty streak Type III – Extracellular lipid pool Type IV – Atheroma – Core of lipid Type V – Fibroatheroma – Fibrotic layer Type VI – Complicated – Ulcer, Ca+ Hemorrhage, thrombus, embolism, aneurysm. Stages of Atheroma - Aorta Stage VI III II Morphologic types: Fatty dots F.Atheroma Plaques Complicated Aterosklerosis Acute Coronary Syndrome (ACS) Chest Pain Plaque Rupture Toward Occlusion Spektrum ACS Unstable Angina Pectoris : (EKG normal, Trop T/I (-)) Acute Non ST-Elevation Myocardial Infarction (NSTEMI) : (EKG normal/ST depresi/T inversi dan Trop T/I (+)) Acute ST-Elevation Myocardial Infarction (STEMI) : EKG ST elevasi dan Trop T/I(+) Prevalensi IMA Di Amerika : kejadian IMA lebih 1 Juta/tahun 200,000 – 300,000 pasien IMA meninggal sebelum sampai RS Total : Warga negara Amerika mengalami IMA setiap 29 detik dan meninggal setiap menit. Indonesia ? Tahun 2008: PJN Harapan Kita 7 pasien ACS , 50-60% IMA 10% IMA < 40 thn Penyebab kematian no 2 di UGD RSSA Topol EJ. CV med 2009 Saifur et al. unpublished data, 2008, 2011 Bagaimana Diagnosa ACS ? Nyeri dada ACS? 1. Cardiac or non cardiac 2. Cardiac : Ischemic non Ischemic 3. Ischemic : Coronary non Coronary 4. Angina pektoris stabil atau ACS Nyeri (tidak enak) dada ….. ? Sifat :Berat/ tertindih (pressure, tightness, or heaviness, strangling, constricting, or compression), Panas (burning) ; Masuk angin, Sesak,”maag” Lokasi: Di dada kiri/tengah tidak bisa ditunjuk Penjalaran : ke bahu/lengan, leher, dagu, belakang,epigastrium Lama : 5-30’ Pencetus :aktifitas/stres/dingin Berkurang: Nitrat/Istirahat Tidak khas: Pingsan/kejang/tidak sadar/berdebar ESC guidelines for SAP 2006 ESC AMI ST elevation guidelines 2008 Angina Pectoris A syndrome resulting from myocardial ischemia Demand and supply imbalance Careful history taking; mode of onset, location, quality of pain, duration, precipitating factors, pattern of disappearance, risk factor, etc Stable vs. Unstable Stable : There is no substantial deterioration in symptoms over several weeks. Stability or quiescence of an atherosclerotic plaque; depending on increased oxygen demand Unstable : symptom pattern worsen abruptly without an obvious caused of increased oxygen consumption, decreased supply . Unstable plaque: ACS Stable Angina Pectoris Canadian Class : I Ordinary physical activity does not cause angina II Slight limitation of ordinary activity III Marked limitation of ordinary activity IV Inability to carry on any activity without discomfort Nyeri dada khas ACS Angina awitan baru derajat 3 menurut klasifikasi kanada kardiovaskuler group ( nyeri dada timbul pada aktifitas ringan sehari-hari) Angina saat istirahat > 20 menit Perburukan derajat angina menjadi derajat 3 dalam beberapa hari – 1 bln terakhir (Crescendo angina) Atypical Hati-hati : Angina Equivalent Indigestion, belching, dyspnea DM, wanita, manula (post operative) Didapatkan 5% dari ACS 2% dipulangkan ternyata ACS Braunwalds Heart Disease 8th Ed 2008 DD Chest pain Ischemic Stenosis Aorta Regurgitasi Aorta Hypertrophic Cardiomyopathy Angina pada Hypertensi Hipertensi pulmonal berat 11th ed Hurst’s the heart 2005 DD Chest Pain Non Ischemic Diseksi Aorta Pericarditis Mitral valve prolaps 11th ed Hurst’s the heart 2005 DD Chest Pain Gastro intestinal Esophageal spasm/reflux/rupture Peptic Ulcer Neuromusculoskeletal Costochondritis Herpes zoster Chest wall pain dan tenderness etc 11th ed Hurst’s the heart 2005 DD chest pain Pulmonary Pulmonary emboli Pneumothorax Penumonia with pleural involvement Pleurisy Psychogenic Axiety/depression/cardiac psychosis etc 11th ed Hurst’s the heart 2005 Non Angina Pain Hanya terasa pada sebagian kecil dada kiri/kanan (bisa di tunjuk) Berkahir berjam jam sampai berhari hari. Biasanya tidak berkurang dengan nitrogliserin Mungkin dicetuskan oleh debaran. ESC guidelines for SAP 2006 ESC AMI ST elevation guidelines 2008 EKG Secepat mungkin – 10’ setelah pasien tiba Diulang apabila meragukan adanya kenaikan segmen ST (ST televasi) Bandingkan denga EKG sebelumnya Pasang monitor EKG EKG : Gambaran aktifitas listrik jantung EKG pada ACS EKG dapat menentukan adanya: Old/Recent/Acute infarction Pericarditis Arrhythmias Pembesaran jantung ST-T changes in STEMI The acute phase is marked by ST segment elevations (current of injury pattern) and sometimes tall positive T waves (hyperacute T waves) Within several hour, myocytes death leads to loss of R amplitude and Q wave appeared During the 1-2 days ST remains elevated, T inverted , Q wave deepen Several days later ST segment return to baseline, T remains inverted, Weeks to months following infarct, Q persist Gambaran EKG pada Iskemik/AMI UAP/Acute NSTEMI Acute NSTEMI Acute STEMI- Evolution Systolic Current Theory Diastolic current Theory Leaky K+ Never fully repolarize Relatively more negative than normal Current directed away from infarct area Baseline shift downward Acute STEMI-Q wave ECG subsets and correlated infarctrelated artery Category Anatomy of Occlusion ECG Findings Proximal LAD Proximal to septal perforator ST elevation V1-6, I, avL, and fascicular or bundle branch block Mid LAD Proximal to large diagonal but distal to first septal perforator ST elevation V1-6, I, avL Distal LAD or diagonal Distal to large diagonal or diagonal itself ST elevation V1-4, or I, avL, V5-6 Moderate to large inferior (posterior, lateral, right ventricular) Proximal RCA or left circumflex ST elevation II, III, avF, and any of the following: a. V1, V3R, V4R b. V5-6 c. R>S in V1-2 Small inferior Distal RCA or left circumflex ST elevation II, III, avF only branch Occluded artery Anterior STEMI ECG demonstrates large anterior infarction Inferior STEMI Proximal large RCA occlusion ST elevation in leads II, III, aVF, V5, and V6 with precordial ST depression Inferior STEMI Small inferior distal RCA occlusion ECG changes in leads II, III, and aVF Peningkatan Enzym jantung Troponin T/Troponin I CKMB Pemeriksaan Fisik Sadar-Koma TD: Hypertensi-Normal-Hypoptensi HR: Regular-irregular/ Bradycardia-Tachycardia pulseless RR: Tachypnea-apnea Cor: Regular-iregular, murmur, gallop Pulmo: Normal-Rales- wheezing Ext: dingin/hangat, edema+/-, etc. Komplikasi MI Mechanical Electrical Ischemia Embolic Inflammation Komplikasi Mekanik Ventricular Septal Rupture Mitral Regurgitation Cardiac free wall rupture Large ventricular aneurysms LV pump failure and cardiogenic shock Dynamic LVOT obstruction RV failure Gagal Jantung (Kriteria Framingham) Major Acute pulmonary edema PND or orthopnea Crackles S3 gallop HJR/Increased JVP Cardiomegaly Wt loss >4.5 kg 5d into Rx Minor Night cough Tachycardia >120 Pleural effusion Hepatomegaly Ankle edema Vital capacity decrease >1/3 from max *Two major or one major and two minor* Komplikasi Elektrik SA Dysfunction Atrial Fibrillation First-Second degree AV block Total AV Block Left Bundle Branch Block Right Bundle Branch Block Ventricular Tachycardia Ventricular Fibrillation Komplikasi Ischemik Perluasan Infark Angina Post-infark Komplikasi Emboli Systemic embolism ; stroke, limb ischemia, renal infarction, intestinal ischemia Inflammation Complication Early Pericarditis Late Pericarditis (Dresslers syndrome) Universal Definition of Myocardial Infarction Diagnosa AMI ditegakkan apabila min memenuhi 2 dari kriteria: Gejala Ischemic Perubahan EKG Kenaikan/penurunan Troponin T/I Diagnosis NSTEMI timi risk ../7…. Acute ant STEMI timi risk… /14 Killip… onset j…am Cepat tegakkan diagnosa dan cepat bertindak (dalam hitungan menit) Semakin tinggi resiko semakin agresif terapi yang diberikan Killip Classification Killip I II III IV Characteristic % Mortality rate No evidence of HF Rales, JVD, S3 Pulmonary edema cardiogenic Shock 85 13 1 1 5.1 13.6 32.2 57.8 TIMI Risk NSTEMI : Umur Faktor resiko >3 Angina Aspirin Diketahui CAD (Cath) Enzymes Depresi segmen ST TIMI Risk STEMI Umur Aada/ tidak faktor resiko Killip Class TD sistolik HR Anterior STEMI/LBBB Onset > 4 jam Stratifikasi Resiko High risk Intermediate risk Low risk Angina saat Istirahat Angina > 20 kurang dengan istirahat Angina dengan aktivitas ALO Riwayat CVD LBBB/RBBB baru Ada Q, ST depresi ENZYME (+) Sedikit meningkat ENZYM (-) MR ATAU S3 Baru, HYPOTENSI, BRADIKARDI, TAKIKARDI. VT Usia > 70 tahun ST DEPRESI> 0.5 T inversi EKG TETAP GRACE SCORE Prinsip Terapi Cepat (time responsif), obati penyebab buka sumbatan Terlambat: Fatal Monitor ketat tanda vital sejak awal Antisipasi dini tanda tanda perburukan dan komplikasi Terapi Awal ACS Atasi keadaan kegawat daruratan : asistol, apneu, syock, lung edema, gagal jantung dll. Terapi reperfusi : PCI, Fibrinolitik, heparin Antiischemic Turunkan oksigen demand : Bed rest total, pendekatan psikologis, dll Terapi komorbid; hipertensi, DM, dll Pentingnya Reperfusi Sumbatan total15-30 menit tanpa kolateral IMA Reperfusion selamatkan miorkard Kematian1 bulan: 25-30% 4-6% dengan reperfusi (PCI, fibrinolytic, antithombotic) ESC AMI ST elevation guidelines 2008 Kerusakan Miokard Irreversibel Miokard tidak mengalami regenerasi Terlambat/tidak dibuka Miokard mati Gagal Jantung rawat ulang biaya besar, kualitas hidup kurang baik Obat gagal Jantung hanya mencegah perburukan, tidak memperbaiki miokard yang mati/infark Alternatif terapi : Stem cell The time is muscle Terapi NSTEMI O2 Bed rest Pain killer Nitrate and anti-ischemia Antiplatelet : Aspirin, Clopidogrel Heparin HTN Hyperglicemia Treat the complication etc Tips Obat anti ischemik atau anti nyeri segera di berikan Anti platelet dan heparin dimasukkan secepatnya setelah diagnosis ACS-NSTEMI ditegakkan, jangan di tunda Turunkan kebutuhan/kerja jantung dengan berikan rasa nyaman dan aman pasien dan bed rest total Setengah duduk pada pasien dengan gagal jantung Pikirkan immediate/urgent PCI pada pasien resiko tinggi/hemodinamik tidak stabil/nyeri berkepanjangn/aritmia maligna dll Alat diagnosis dan monitoring Perawat Keluhan berhubungan dengan fungsi dan beban jantung, deteksi dini komplikasi Monitor tanda vital, saturasi, perfusi, EKG, intake- output, balance. dll Kalau perlu ukur CVP, arteri line dll Laboratorium : Enzyme jantung, analisa gas darah, fungsi ginjal, elektrolit, komorbid (infeksi, dm, dll) Intervensi keperawatan Turunkan kebutuhan dan bebang jantung misalnya istirahat fisik dan mental, kondisi hangat, tenang, rasa aman, pemilihan diet : NGT atau bantuan makanan, dilarang mengejan, atasi febris, rasa sakit atau sesak dll Bantu fungsi jantung: Inotropic, IABP, anti iskemik, dll Atasi komorbid/komplikasi: hipertensi, DM, infeksi, gagal jantung, gangguan ginjal, dll Atasi kekurangan atau kelebihan cairan, kalori, oksigen, PH, elektrolit, dll Terapi STEMI O2 Bed rest Pain killer Nitrate and anti-ischemia Antiplatelet : Aspirin, Clopidogrel Fibrinolytic time to neddle : 30 m/PCI HTN Hyperglicemia Treat the complication etc Fibrinolitik Manfaat bila onset < 12 jam, optimal bila onset < 3 jam Bila dikirim ke RS dengan PCI > 90 menit, fibrinolitik Konsep baru : Fibrinolitik di Ambulan menuju RS Perhatikan kontraindikasi fibrinolitik Awasi ketat komplikasi fibrinolitik seperti perdarahan, stroke, syok dll Perhatikan tanda tanda keberhasilan: nyeri hilang, ST elevasi turun >50%, Junctional VES(+), bila gagal rescue PCI Kontra Indikasi Absolut Any prior ICH Known structural cerebral vascular lesion (eg, AVM) Known malignant intracranial neoplasm (primary or metastatic) Ischemic stroke within 3 months EXCEPT acute ischemic stroke within 3 hours Suspected aortic dissection Active bleeding or bleeding diathesis (excluding menses) Significant closed head or facial trauma within 3 months Kontra Indikasi Relatif History of chronic severe, poorly controlled hypertension Severe uncontrolled hypertension on presentation (SBP greater than 180 mm Hg or DBP greater than 110 mm Hg)† History of prior ischemic stroke greater than 3 months, dementia, or known intracranial pathology not covered in contraindications Traumatic or prolonged (greater than 10 minutes) CPR or major surgery (less than 3 weeks) Recent (within 2 to 4 weeks) internal bleeding Noncompressible vascular punctures For streptokinase/anistreplase: prior exposure (more than 5 days ago) or prior allergic reaction to these agents Pregnancy Active peptic ulcer Current use of anticoagulants: the higher the INR, the higher the risk of bleeding Treatment of STEMI Percutaneous Coronary Intervention •Primary PCI : Pasien langsung di lakukan tindakan reperfusi dengan membuka sumbatan di arteri koroner tanpa dilakukan fibrinilotik terlebih dahulu •Rescue PCI : Dilakukan PCI setelah gagal dengan terapi fibrinolitik •Facilitated PCI : Pasien dilakukan fibrinolitik terlebih dahulu meskipun sudah ada rencana PCI •Urgent PCI: As soon as possible •Early PCI : Dalam waktu 24 jam pertama Early/urgent PCI: Resiko tinggi, hemodinamik tidak stabil, aritmia maligna, angina (+) dgn terapi, EF <40%,Gagal jantung, Riwayat PCI, CABG dl 6 bl Tim PCI Target 1. Time to balloon : 90 m 2. Yang dibuka hanya Culprit lesion (pembuluh darah tersumbat yang menyebabkan IMA kali ini) saja 3. Aliran darah yang diintervensi kembali lancar Primary PCI Case A 53 yo man reffered from a private hospital for primary PCI A typical chest after exercise 2 hr prior to admission ECG send by fax PCI appointment via phone Patient directly transfer red to cath lab. Case 2 Mr W. 28 yo, smoker and family history Admit to Nearest private hospital with chief complaint of Heaviness while he was driving a car 30 min prior to admission Case 2 ECG on admission Case 2 ECG on referral hospital (after double antiplatelet tx) CABG Failed PCI with persistent pain or hemodynamic instability in patients with coronary anatomy suitable for surgery. Persistent or recurrent ischemia refractory to medical therapy in patients who have coronary anatomy suitable for surgery, have a significant area of myocardium at risk, and are not candidates for PCI or fibrinolytic therapy. At the time of surgical repair of postinfarction ventricular septal rupture (VSR) or mitral valve insufficiency. CABG Cardiogenic shock in patients less than 75 years old with ST elevation, LBBB, or posterior MI who develop shock within 36 hours of STEMI, have severe multivessel or left main disease, and are suitable for revascularization that can be performed within 18 hours of shock Life-threatening ventricular arrhythmias in the presence of greater than or equal to 50% left mainstenosis and/or triple-vessel disease. Yang sering di lupakan….. Edukasi pasien mengenai : Mengapa bisa sampai sakit….. Pola hidup Kepatuhan untuk merubah pola hidup Faktor resiko di kendalikan, rokok, HT, dll Kepatuhan minum obat Mencegah serangan jantung berikutnya dengan…..merubah pola hidup, atur pola makan, olah raga teratur dan terukur Reperfusi adalah awal dimulainya hidup baru …agar koroner tetap terbuka Simpulan Tegakkan diagnosa dengan cepat dan tepat Terapi dengan cepat dan tepat : Reperfusi Monitor ketat Cegah komplikasi Edukasi untuk prevensi dan rehabilitasi …..…….Kerja keras di awal……