Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
CLIN.
CHEM.
41/11,
1614-1616
(1995)
#{149}
Drug
Monitoring
False-Positive
and False-Negative
Christine
Douglas
Moore,
Lewis,’
and
and
Rates
Jerrold
in Meconium
Indexing
gas chromatography-mass
metabo!ites/solvent
Terms:
clinical
phase
spectrometty/pediatextraction/solid-
chemistry/drug
extraction
Analysis
of meconium
ysis of neonatal
urine
is becoming
increasingly
longer
history
higher
drug
as an alternative
to the analto determine
fetal drug exposure
popular.
Meconium
provides
a
exposure
than
urine
(1), contains
of drug
concentrations
than
urine,
and
is easier
to
collect.
However,
unlike
National
Institute
on Drug
Abuse
urine
testing,
the analysis
of meconium
is not
government
regulated. The actual extraction and analysis procedures
are perceived as having no significant
impact on the results. Our laboratory undertook
two
experimental
protocols to estimate the false-negative
and false-positive rates associated with current meconium
testing procedures
to determine
(a) whether
differences exist between
published
screening
procedures
and (b) whether
the reporting
of screen-only
data
is acceptable.
First,
our
cedures
nium
to
with
some
the
the
screening
we
noassay
compared
determination
determine
Second,
by
(GC-MS),
published
drugs
false-negative
rate
proin meco-
associated
methods.
determined
gas
three
of abused
the
screen-positive
firmed
only
laboratory
for
actual
samples,
number
to determine
the
of immu-
subsequently
chromatography-mass
con-
spectrometry
false-positive
rate
of screen-
data.4
‘US
Drug
Testing
Laboratories,
Chicago,
IL 60612.
2 Rush
Poison
Control
Center,
Hospital,
Author
1653
for
W. Congress
correspondence.
2201
W.
Campbell
Rush-Presbyterian
Pkwy.,
Fax
Park
St.
Dr.,
1614
Experiment
We confirmed
by GC-MS
analysis that 100 meco
nium samples contained drugs after homogenization
i
organic
solvent
and then
solid-phase
or solvent
extrac
tion, and 26 meconium
samples
contained
no drugs.
W
did not screen
the samples
before
GC-MS
analysis.
Al
the samples
were then reextracted
according to thre
published methods.
Method
CHEMISTRY,
Vol.
41. No. 11, 1995
1
In method
la, water (10 mL) and concentrated
HC
(1 mL) were added to meconium
(1 g). The mixture wa
vortex-mixed,
filtered, and centrifuged. The supernatant was analyzed
for opiate and cocaine metabolites
by enzyme-multiplied
immunoassay
technique (EMIT).
In method
ib, methanol
(0.4 mL) was added to meconium (0.1 g), mixed, and left at room temperature
fo
10 mm. The mixture was centrifuged and analyzed b
EMIT
for cannabinoids
(2).
Method
2
To meconium
(1 g), 5 mL
of 0.1 molfL
phosphate
buffer-methanol
(4:1) were added. The mixture
was
centrifuged
and filtered, and the supernatant
was
analyzed
by EMIT
for amphetamines,
cannabinoids,
cocaine, and opiate metabolites.
The screening cute
values for methods
1 and 2 were 50 .tgfL, as recommended
in the literature
(3).
Method
3
Meconium
(1 g) was
homogenized
in glacial acetic
acid (3 mL). Diphenylamine
in acetone (1.67 mgfL;
6
mL) was added, and the resultant
solution
was mixed
and centrifuged.
The top layer was evaporated
to
dryness (a drop of 1% H2S04
was added
to prevent
amphetamine
loss). The sample
was reconstituted
in
Abbott AD5 buffer-methanol
(50:50; 0.7 mL) and centrifuged.
The top lipid
layer
was
aspirated,
and
the
concentrated
extract
was analyzed
for drugs
by fluorescence
polarization
immunoassay
(FPIA)
(4).
For
method
3, the screening cutoff values were 50 pg/kg
for
all compounds.
All screen-positive
rates were subsequently
reconfirmed
by GC-MS
at cutoff
values
of 5
pg/kg
for cocaine
metabolites,
opiates,
and
amphetamines
and 2 pg/kg
for tetrahydrocannabinol
(THC)
metabolites.
Experiment
2
Many
hospital
Nonstandard
CLINICAL
1
Luke’s
Chicago,
IL 60612.
312-421-7249.
abbreviations:
GC-MS, gas chromatography-mass
spectrometry;
EMIT,
enzyme-multiplied
immunoassay
technique;
FPIA,
fluorescence
polarization
immunoassay;
THC,
tetrahydrocannabinol;
and m-OH-BZE,
m-hydroxybenzoylecgonine.
Received
March
20, 1995;
accepted
July
12, 1995.
‘
Drug Testing
Leikin”2
To determine
the number
of false-negative
results
produced
by inefficient
extraction
of drugs from meconium,
three
published
procedures
were
compared
by using
previously
confirmed
positive
and negative
meconium
specimens.
The methods
were
not equivalent
in their
ability to extract
drugs from the matrix.
To determine
the
number
of false positives
reported
by the use of screenonly (unconfirmed)
results,
535 screen-positive
meconium specimens
were subjected
to confirmation
by gas
chromatography-mass
spectrometry.
Fifty-seven
percent of the samples
were confirmed
positive
for one or
more of the drugs
under
investigation,
showing
that a
false-positive
rate as high as 43%
may exist
when
unconfirmed
screening
results
are used.
nc
Toxicology
screening
results.
use
results
The
is
unethical
use
laboratories
to determine
of screen-only
and
highly
rely
on
immunoassay
positive
and negative
data to report any drug
dangerous.
False-positive
esults
may cause
a mother
to lose her child or even
mprisoned
for child endangerment.
False-negative
tults
may result
in denial
of specialized
treatment
aewborns.
be
refor
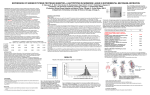
Table
mc
1ethods
Cocaine
(n = 48)
la and lb
months
total meconium
samples),
our
Laboratory
correlated
the
number
of screen-positive
tamples
against
the number
of results
confirmed
by
GC-MS.
The
samples
were
homogenized
in organic
3olvent
and
centrifuged,
and
the
supernatant
was
reextracted.
The final
solvent
was evaporated
to dryaess, reconstituted
in buffer,
and screened
by FPIA.
An aliquot
of any meconium
samples
that
screened
ositively
was reextracted
[solid-phase
method
for coaine and its metabolites; solvent extraction for opiates
5), amphetamines,
and
THC-COOH
(6)]. The drugs
ere confirmed
by selected-ion
monitoring
GC-MS
at
he following
cutoffs:
codeine,
morphine,
amphetamine,
2
(939
ethamphetamine,
cocaine,
and metabolites,
5 ng/g (5
g/kg);
THC
metabolite,
2 ng/g (2 pg/kg).
All GC-MS
alyses
were carried
out in splitless
injection
mode,
to
aximize
sensitivity,
on an HP 5890
gas chromatoaph
connected
to a 597 1A mass
selective
detector
Hewlett Packard, Naperville, IL) and equipped
with a
B-5 MS column
[25 m X 0.02 mm
(i.d.)
X 0.33-.tm
film thickness)]
(J & W Scientific,
Folsom,
CA); the
amer
gas
was
y deuterated
helium.
internal
All compounds
calibrators
were
(Radian
quantified
Corp.,
Aus-
2
3
b
result
Discussion
and
not
substantially
different
in their
ability
to detect
gs of abuse
in meconium
(Table
1). Method
1
etected
only 19.6%
of positive
samples;
all were
canabinoid
positive
as extracted
by method
lb.
In method
la, the inorganic
acid
failed
to extract
ocaine
or opiate
metabolites
from meconium.
Method
was an improvement
on method
1, probably
because
f the incorporation
of an organic solvent vs an inor-
50
100
100
number
Overall
(n = ii i)
Opiates
(n = 14)
n/ab
100; overall
superior
because
noassay
0
19.6
7.1
54.5
100
of positives,
100
111.
extracts
two
analyzed
10
readable
yielded
(EMIT
study
by FPIA
background
noise
in
analyzed
by
FPIA
only
the
prevented
addithe
blindly
1 and
selected
2. The
of EMIT.
Only
lb
eight
gave
a
samples
indicating
specimen.
Overall,
positive
result
with
of positive
rates
with
by method
3 were
because
use
We conclude
that
stantially
affect
the
extraction
procedure
Experiment
an
method
the
3
immu-
From
The
other
the instrument,
yielded
only
one
more
1 and the same
number
2. The
samples
extracted
the
out.
instead
by
a
FPIA),
carried
analyzed
samples
result
by FPIA.
error
messages
on
excessive
in
vs
was
were
of method
differences
chosen
ng/mL
sensitivity
samples,
10 samples
were
according
to methods
were
of
in
in
efficiency
of inherent
comparative
original
126
and
extracted
reported
extraction
technique
tional
of
sample
turbidity,
of EMIT.
the immunoassay
outcome
of the
does.
does
analysis
not subbut the
2
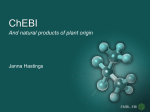
A total of 535 samples
one or more
drugs. No
(57%)
screened
positively for
screened positively for
phencyclidine,
and
of these,
285
(53.3%)
were confirmed
by GC-MS.
The breakdown
of each drug class is
shown
in Table
2. The overall
false-positive
rate
was
samples
46.7%.
Our
1
All specimens
were
first analyzed
by GC-MS
before
hey were
screened
by immunoassay
to validate
the
eliability
of the screening
procedure.
The 26 negative
pecimens
were negative by GC-MS
and immunoanaytically.
However,
the
three
screening
procedures
51.2
48.8
of the
which
and
0
72.9
diluted
form
[the
results
being
(p.gfL) rather
than
ng/g (pg/kg)].
To verify
that
the differences
ons 403, 282, 346; m-OH-BZE
533, 476, 282; THCOOH
572, 515, 413).
Opiates
were
analyzed
as triethylsilyl derivatives
(codeine ions 371, 343, 234;
orphine
429, 430, 401). Amphetamines
were anayzed as heptafluorobutyryl
derivatives (amphetamine
ons 240, 118, 91; methamphetamine
254, 210, 118).
esults
Amphetamines
(n = 6)
43)
=
ganic
acid for the extraction
of drug
metabolites
from
meconium.
Evaporation
and reconstitution
of the extract
in method
3 improved
the sensitivity
of the assay
over methods
1 and 2, which
analyze
the extract
in a
FPIA
method
method
xperiment
(n
100
TX).
Benzoylecgonine,
m-hydroxybenzoylecgonine
(mH-BZE),
and THC-COOH
were analyzed
as the teriary
butyldimethylsilyl
derivatives
(benzoylecgonine
Techfor
been
metabolite
Number
of samples,
n/a. not available.
in,
erivatizing
reagents
were
obtained
from Regis
ologies,
Morton
Grove,
IL).
Other
procedures
-MS confirmation
of drugs
in meconium
have
eported
(7, 8) with
differing
cutoffs.
comparability.
% positive
Method
For
1. Diagnostic
immunoassay
because
is
the
higher
than
amount
very
of
small,
lytical
cutoffs
sensitivity
the
available
especially
in
for
intentionally
for
requirement
meconium
procedures
were
required
for
for
premature
meconium
low
meconium
drug
testing
urinalysis.
The
testing
is
babies;
thus
testing
usually
ana-
be
must
ere
Table
2. Screening
results
for 939 meconium
Positive
screen
THC metabolite
Cocaine metabolite
confirmation
173
228
97
135
Opiates
60
34
Amphetamines
74
19
CLINICAL
CHEMISTRY,
samples.
Positive
Vol. 41, No. 11, 1995
%
positive
56.1
59.2
56.7
25.7
1615
to accommodate
the limited sample
size.
Failure to address this issue would render the procedure
unavailable
to the very infants
who are in most
need of correct diagnoses.
Raising
the immunoassay
metabolize
cutoff concentrations
would result in a decreased
ber of false-positive
screens
but would
also increase
number
of false-negative
rates. False-negative
The goal of the meconium
test is to provide the clinician
with an accurate fetal drug exposure history; therefore,
sensitivity is of primary
importance.
A sensitive screen
assay sacrifices specificity; therefore, a specific con.firinatory procedure
is necessary. Such an approach
does not
lend itself to reporting screen-only results. Healthcare
professionals should be aware
of the possible consequences that may arise from such diagnoses.
designed
are
also
increased
by
the
use
of inefficient
numthe
rates
extraction
procedures
described above. False-positive screens are
not a problem
if confirmed
by a different technique.
Amphetamines.
The greatest discrepancy
between
screen and confirmatory
data occurred with the amphetamine
drug
class.
Various
nonprescription
medications
contain
cross-reacting
substances
such
as
phenylpropanolamine
or pseudoephedrine.
Phenylethylamine,
an endogenous
compound,
with the polyclonal assay and with
tions. Of the
positive
amphetamine
contained
not
pseudoephedrine
amphetamine
or
or
also
GC-MS
interferes
confirma-
screens,
74.3%
phenylethylamine
but
THC
metabolite.
Nonsteroidal
anti-inflammatory
drugs,
particularly ibuprofen, cross-react in immunoreactive systems
with the THC
metabolite
assay and
produce false-positive screens.
Opiates.
Positive
results
for opiates
may
derive
from
prescription medications
containing, e.g., hydrocodone
or hydromorphone
(5).
Cocaine
metabolite(s).
Possibly,
not all unconfirmed
screen-positive
rates
for cocaine
are falsely
positive.
The
cocaine
recent
discovery
metabolite,
of
as
m-OH-BZE,
a contributor
a minor
to
meconium
urinary
im-
munoassay
screens shows that fetal metabolism
does
not reflect adult metabolism
(9). In almost one-fourth
of meconium
samples,
this compound
is the only cocaine
metabolite
present
(10).
Other
drugs
may
not
1616
CLINICAL
CHEMISTRY,
and unidentified
noreactive
Vol. 41, No. 11, 1995
metabolites
may
by the adult model,
contribute
to immu-
responses.
References
1. Varley
J, Ryan
R, Kwong TC. Detection of benzoylecgonine
in
meconium:
a more
sensitive
index
of intrauterine
cocaine
exposure
[Abstract].
Clin
Chem
1992;38:1003.
2. Ostrea
EM. Method
for detecting
maternally
transferred
drug
metabolites
in newborn
infants.
US Patent
5 015 589,
1991.
3. Ostrea
EM. Method
for detecting
maternally
transferred
drug
metabolites
in newborn
infants.
US Patent
5 185 267,
1993.
4. Lewis
methamphetamine.
in the fetus as predicted
DE. Forensically
tional
fetal
Patent
5 326
exposure
to
acceptable
determinations
and other chemical
drugs
of
agents.
gesta-
US
708,
1994.
5. Moore
C, Deitermann
D, Lewis
D, Leikin
J. The
detection
o
hydrocodone
in meconium:
two case studies.
J Anal Toxicol (in press).
6. Moore CM, Lewis DE, Becker
JW, Leilcin
JB. Determination
ol
11-nor--9-tetrahydrocannabino1-9-carboxylic
acid (THC-COOH)
in meconium.
J Anal Toxicol
(in press).
7. Moriya
F, Chan
KM, Noguchi
‘F,
Wu PYK. Testing
for drugs
of abuse
in meconium
of newborn
infants.
J Anal
Toxicol
1994;
18:41-5.
8. Clark
GD,
Rosenzweig
IB, Raisys
VA,
Callahan
CM,
Grant
TM, Streissguth
in meconium.
AP. The analysis of cocaine and benzoylecgonine
J Anal
Toxicol
1992;16:261-3.
9. Steele
BW,
Bandstra
ES,
Wu
NC, Hime GW, Hearn
WL.
m-Hydroxybenzoylecgonine:
an important
contributor
to the immunoreactivity
in
assays
for
benzoylecgonine
in meconium.
J Anal
Toxicol
1993;17:348-52.
10. Lewis
D, Moore
C, Leikin
J. Incorrect
diagnosis
of cocaine
exposed
babies:
a report.
Neonatal
Intensive
Care
1994;7:24-6.