Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prescription costs wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Toxicodynamics wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Theralizumab wikipedia , lookup
Effects of long-term benzodiazepine use wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
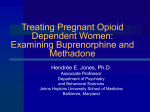
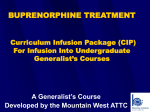
Toxicol Rev 2006; 25 (2): 79-85 1176-2551/06/0002-0079/$39.95/0 REVIEW ARTICLE 2006 Adis Data Information BV. All rights reserved. Does High-Dose Buprenorphine Cause Respiratory Depression? Possible Mechanisms and Therapeutic Consequences Bruno Mégarbane,1,2 Raymond Hreiche,1 Stéphane Pirnay,1,3 Nicolas Marie1 and Frédéric J. Baud1,2 1 INSERM U705, CNRS, UMR 7157, Université Paris 7, Université Paris 5, Hôpital Fernand Widal, Paris, France 2 Assistance Publique – Hôpitaux de Paris, Hôpital Lariboisière, Réanimation Médicale et Toxicologique, Université Paris 7, Paris, France 3 Laboratoire de Toxicologie de la Préfecture de Police, Paris, France Contents Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79 1. Pharmacological Properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80 2. Buprenorphine-Associated Toxic Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81 3. Respiratory Effects of Buprenorphine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82 4. Mechanisms of Interaction with Benzodiazepines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83 5. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84 Abstract Buprenorphine is an opioid agonist-antagonist with a ‘ceiling effect’ for respiratory depression. Compared with methadone, its unique pharmacology offers practical advantages and enhanced safety when prescribed as recommended and supervised by a physician. Buprenorphine has been approved in several countries as an efficient and safe maintenance therapy for heroin addiction. Its use resulted in a salutary effect with a reduction in heroin overdose-related deaths in countries that implemented office-based buprenorphine maintenance. In France, however, where high-dose buprenorphine has been marketed since 1996, several cases of asphyxic deaths were reported among addicts treated with buprenorphine. Death resulted from buprenorphine intravenous misuse or concomitant sedative drug ingestion, such as benzodiazepines. In these situations of abuse, misuse, or in association with elevated doses of psychotropic drugs, buprenorphine may cause severe respiratory depression. Unlike other opiates, the respiratory effects from buprenorphine are not responsive to naloxone. However, the exact mechanism of buprenorphine-induced effects on ventilation is still unknown. The role of norbuprenorphine, the main N-dealkylated buprenorphine metabolite with potent respiratory depressor activity, also remains unclear. Experimental studies investigating the respiratory effects of combinations of high doses of buprenorphine and benzodiazepines suggested that this drug-drug interaction may result from a pharmacodynamic interaction. A pharmacokinetic interaction between buprenorphine and flunitrazepam is also considered. As there are many questions regarding the possible dangers of death or respiratory depression associated with buprenorphine use, we aimed to present a comprehensive critical review of the published clinical and experimental studies on buprenorphine respiratory effects. Heroin addiction remains a major concern worldwide and causes numerous fatalities.[1,2] Treatment of heroin addicts underwent a profound evolution with the development of maintenance therapies including methadone and buprenorphine. The objective of the substitution programmes is to decrease intravenous drug abuse-related mortality and morbidities. Treatments aim to reduce involvement in the illicit drug scene, by shifting the context of heroin use into a medically supervised framework that offers more support and greater possibilities of health promotion and social integration. Countries have chosen different strategies for maintenance and detoxification treatment of opioid dependence. Numerous opioid molecules have been approved, different facilities for 80 Mégarbane et al. prescription and delivery established, and various treatment monitoring systems organised. In October 2002, the US FDA approved buprenorphine for the treatment of opioid dependence. Treatment of heroin addicts was limited to physicians with specialised training or experience and limited to a maximum of 30 patients per physician.[3] Buprenorphine has been used in some European countries for a longer period of time. In France, a high-dosage buprenorphine formulation has been marketed since 1996. While methadone was still prescribed in specialised health centres, buprenorphine was authorised for all registered practitioners and pharmacies.[4] In this country, about 90 000 addicts are treated today with high-dosage buprenorphine versus 25 000 with methadone.[5] The success of the French heroin substitution programme was demonstrated by the decrease of deaths due to heroin overdoses (from 465 in 1996 to 89 in 2003) and the decline of the arrests due to heroin use (from 17 328 to 4025 in the same period).[6,7] The public health benefits experienced in France bring to question the value of the more stringent regulations on prescribing buprenorphine imposed in many other countries throughout the world. Buprenorphine exhibits unique pharmacological properties and has shown to be lacking of significant respiratory effects at therapeutic doses, both in experimental and clinical studies. However, since its availability as a substitution therapy in humans, several cases of severe respiratory depression and death have been reported in drug addicts. Our objective was to review the recent hypothesis on the mechanisms of the respiratory effects of buprenorphine in the light of its pharmacology. 1. Pharmacological Properties Buprenorphine is a semi-synthetic, highly lipophilic opioid derived from thebaine. It is used as an analgesic (usual doses [Temgesic]:1 0.3mg every 6 hours by intravenous or intramuscular routes or 0.4–0.8 mg/day sublingually) and as maintenance therapy (high-dosage [Subutex]: 8–32 mg/day). Regarding its analgesic properties, buprenorphine is 25–50 times more potent than morphine.[8] It is considered a partial mu-opioid receptor agonist and a weak kappa-receptor antagonist. It possesses a high affinity for both receptors (1000 times higher than morphine), resulting in a slow dissociation (K(i) in the subnanomolar range: 6.10–12 and 4.10–12 mol/L, respectively) and a long duration of action.[9] Buprenorphine affinity for the delta receptors is lower (K(i): 4.8.10–10 mol/L). The half-life for dissociation from the mureceptor is 166 minutes, compared with 7 minutes for fentanyl.[10] These properties explain the slower onset and longer duration than morphine. For example, intramuscular administration results in peak respiratory effects at 3 hours and maximal miosis at 6 hours in humans. Like naloxone, buprenorphine is able to antagonise the 1 respiratory depression induced by anaesthetic doses of fentanyl, without preventing opioid pain relief.[11] Like all opioids, side effects include sedation, nausea, vomiting, dizziness, sweating and headaches. Similarly, when discontinued, a typical morphine-like withdrawal syndrome develops with a delayed onset of 2–15 days. Buprenorphine pharmacokinetic properties help explain its remarkable effects. High-dosage buprenorphine undergoes extensive first-pass hepatic metabolism, thus it is administered sublingually with a 60–70% bioavailability. Tissue distribution is wide, with a peak plasma concentration at 90 minutes. Kinetics follow a three-compartment model with a terminal elimination half-life of 27 hours (values ranging from 3 to 44 hours), a distribution volume of 48 L/kg, and a total clearance of 100 mL/ kg/min.[12] Cerebral distribution is important due to its lipophilic properties (octanol/water partition coefficient: 1943 ± 50 and pKa: 8.42 ± 0.03). Buprenorphine is highly (96%) bound to plasma proteins, mainly globulins. Buprenorphine is transformed in the liver to inactive conjugated metabolites. However, its extensive Ndealkylation, catalysed by cytochrome P450 (CYP) 3A4, produces an active metabolite called norbuprenorphine (figure 1).[13] Human pharmacokinetic studies showed low plasma concentrations of norbuprenorphine following buprenorphine administration, but with peaks and elimination half-lives that markedly varied according to the routes of administration and among individuals.[12] Most of buprenorphine (70–90%) is excreted in the faeces. Both Ndealkylated and conjugated metabolites are detected in the urine. Various drugs that induce (antiepileptic drugs) or inhibit (macrolides, azole-based antimycotic drugs and HIV protease inhibitors) the CYP 3A4, may interfere with buprenorphine metabolism. However, their clinical implications remain unknown. The relationship between buprenorphine plasma concentration and response in the opioid-dependence treatment has not been studied.[12] Buprenorphine dosage does not need to be significantly adjusted in patients with renal impairment; however, it is possible that the metabolism of buprenorphine will be altered in patients with severe chronic liver disease including decreased CYP3A activity. Finally, it is well known that buprenorphine is frequently injected by users (around 33%), despite the labelling for sublingual use.[14,15] Thus, routine monitoring of buprenorphine misuse may be warranted, needing the development of effective countermeasures to address diversion and injection in this setting.[16] Consequently, a sublingual preparation (Suboxone) associating buprenorphine and the poorly gastrointestinal-absorbed naloxone (4 : 1 combination) has been marketed, aiming to limit diversion by precipitating withdrawal symptoms, if parenterally self-injected by addicts.[17] The presence of naloxone does not appear to influence the pharmacokinetics of buprenorphine. The use of trade names is for product identification purposes only and does not imply endorsement. 2006 Adis Data Information BV. All rights reserved. Toxicol Rev 2006; 25 (2) Does High-Dose Buprenorphine Cause Respiratory Depression? 81 HO O N H3CO n atio xyl o ydr H A7 ,3 , 5 3A 4 3A CH3 HO 8 C ,2 C CH3 N-d e CH2OH alk CH3 YP yla tio n M1 C HO HO HO O N-dealkylation N N CYP3A5, 3A4, 3A7, 2C8 H3CO O Hydroxylation O NH CYP3A4, 3A5 H3CO H3CO CH3 HO CH3 C HO CH3 CH3 CH3 Buprenorphine C CH3 HO CH3 CH3 M3 Norbuprenorphine dro xyl atio n CH2OH CH3 CH3 Hy CH3 C HO HO OH OH N-dealkylation O O NH N H3CO H3CO CH3 HO CH3 C CH3 CH3 M2 CH3 HO CH3 C CH3 CH3 M4 (or M5) Fig. 1. Molecular structure of buprenorphine and its different metabolic pathways in the liver (reproduced from Chang et al.,[13] with permission). M1–M5 = different metabolites. 2. Buprenorphine-Associated Toxic Deaths Despite limited side effects, >100 cases of buprenorphinerelated fatalities have been reported in France.[18-23] Several other cases were also reported in the Nordic countries (Denmark, Finland, Iceland, Norway and Sweden).[24] Similarly, an increase in buprenorphine-related deaths has been identified since 1999 in the UK.[25] Forensic reports consistently concluded that death resulted from asphyxiation.[18-23] Fatality was usually associated with buprenorphine intravenous misuse (intravenous injection of crushed tablets) or concomitant sedative drug ingestion, such as benzodiazepines. In one case, death was due to a massive oral 2006 Adis Data Information BV. All rights reserved. ingestion.[18] Poisonings are characterised by a high frequency of multiple opiate/opioid association, as well as psychoactive drug co-ingestion. In fatalities, as neither toxic nor lethal concentrations of buprenorphine were available, forensic studies reported either elevated or therapeutic blood concentrations (evaluated from clinical studies in the range of 2–20 ng/mL).[21-23] However, systematic analysis of death causes revealed the difficulties in determining the role of substitution drugs in the death process, as many other factors might be involved, including circumstances surrounding death, past history, differential selection of subjects into either substitution modality and concomitant intake of other drugs.[23] Moreover, as death caused by benzodiazepines in the Toxicol Rev 2006; 25 (2) 82 Mégarbane et al. absence of underlying disease is uncommon,[26] fatalities were attributed in some cases to the association of buprenorphine and benzodiazepines. However, as many addicts regularly use benzodiazepines in association with their maintenance therapies, the mechanism of the deleterious interaction between buprenorphine and benzodiazepines is questionable. The potential for synergistic or additive actions by other psychoactive molecules, including opioids, alcohol and neuroleptics should also be considered. 3. Respiratory Effects of Buprenorphine The exact mechanism of buprenorphine acute toxicity remains misunderstood. Respiratory depression is the suspected aetiology of buprenorphine-related deaths. The majority of opioids induce a dose-dependent respiratory depression in experimental models.[27] In rats, morphine and methadone elicit the rapid onset of dosedependent respiratory acidosis and hypoxia.[28,29] In contrast, doseeffect relationships of buprenorphine suggest either limited effects over a 0.008–3 mg/kg intravenous dose range[30] or a plateau of respiratory effects due to its antagonist effects at higher doses.[27,31,32] These results were confirmed by the absence of significant effects on arterial blood gases after a single 3, 30, or 90 mg/kg buprenorphine infusion, compared with the solvent.[33] A more recent study in volunteers showed that while the analgesic effect of buprenorphine increased significantly when administering a dose from 0.2 to 0.4mg per 70kg, respiratory depression was similar in magnitude and timing for the tested doses.[34] Buprenorphine caused depression of the minute ventilation, which levelled off at doses ≥3 µg/kg to about 50% of baseline. Irrespective of the time at which measurements were obtained, buprenorphine showed a modest non-linear effect on arterial carbon dioxide tension (maximum value measured, 5.5 kPa), with a ceiling effect at doses >1.4 µg/kg.[35] In another volunteer study, the carbon dioxide response curves were depressed in a time-dependent, prolonged and biphasic manner at various times up to 20 hours after administration of epidural buprenorphine 0.15mg.[36] This ‘ceiling effect’ was thought to confer in humans a high safety profile, mild mental status changes, mild to minimal respiratory depression, small but not pinpoint pupils and relatively normal vital signs.[3] In fact, since its availability as a maintenance therapy, respiratory side-effects have been rarely reported, especially in office-based treatment of opioid dependence.[37] In contrast, in situations of abuse, typical features of severe opioid poisoning (coma + miosis + respiratory depression) were described.[6,38,39] However, because of the retrospective data collection in these studies and the lack of systematic laboratory-confirmed poisonings, significant limitations make conclusions cautious, warranting further prospective observational studies. Particularly in regard to the management of buprenorphine overdoses, where contradictory results appeared. Indeed, in one case series, a rapid improvement of the patients using 0.4–0.8mg naloxone was reported,[38] whereas in a placebo-controlled study in volunteers, no effects of 1mg naloxone on mild respiratory depression and non-immediate reversal despite higher doses were observed, once the effects have been produced.[40] The exact mechanism of buprenorphine-induced respiratory effects is unclear. In several fatal cases related to buprenorphine overdoses, high plasma or tissue concentrations of norbuprenorphine were reported, suggesting its role in the onset of death.[18-23] Norbuprenorphine, the main N-dealkylated buprenorphine metabolite, is a very potent respiratory depressor. Significant respiratory depression has been demonstrated following the administration of a single intravenous dose of 3 mg/kg norbuprenorphine in rats.[41-43] However, it is unclear whether norbuprenorphine alone can fully explain buprenorphine-related deaths. Recent experimental data in rats have shown that significant quantities of norbuprenorphine can be detected in the plasma, Mechanism of reversion Mechanism of prevention N N N B N µ δ Respiratory depression N N B µ δ Respiratory depression B B µ δ Respiratory depression Fig. 2. Schematic representation based on binding experiments, of the buprenorphine (B)-related protection and reversion of the norbuprenorphine (N)induced respiratory depression in rats.[42] 2006 Adis Data Information BV. All rights reserved. Toxicol Rev 2006; 25 (2) Does High-Dose Buprenorphine Cause Respiratory Depression? immediately after buprenorphine administration.[44] Different mechanisms for the norbuprenorphine role were proposed, including a transient decrease in respiratory frequency, an early onset of seizures, as well as a sustained muscle rigidity. However, in rats, when buprenorphine and norbuprenorphine were co-administered, buprenorphine completely prevented, as well as reversed norbuprenorphine-induced respiratory effects.[43] Binding experiments suggested a role for mu- and to a lesser extent for deltaopioid receptors in buprenorphine protective effect against norbuprenorphine-induced respiratory depression (figure 2). In animals, significant protective effect was observed even when norbuprenorphine exceeded buprenorphine concentrations in plasma,[43] whereas in the majority of reported human fatalities, buprenorphine exceeded norbuprenorphine concentrations.[18-23] Thus, discrepancy between human and experimental data calls into question the role of norbuprenorphine alone as the mechanism of buprenorphine-associated death in humans. Alteration of opioid receptor expression in the CNS may also influence the respiratory effects of buprenorphine. A recent study in rats using a β-imager clearly established that an acute buprenorphine administration induced a down-regulation of mu-opioid receptors throughout the brain.[45] Whereas a single buprenorphine administration induced no changes in kappa- or delta-opioid receptor binding, repeated administration up-regulated kappa-receptor density and decreased delta-receptor affinity.[46] 4. Mechanisms of Interaction with Benzodiazepines Given the forensic data collected in addicts who died in relation to buprenorphine use, a deleterious interaction between buprenorphine and benzodiazepines was hypothesised to explain acute toxicity. The interaction between benzodiazepines and opioids including buprenorphine and methadone has resulted in respiratory depression in both animal models and humans.[29,47,48] McCormick et al.[29] reported severe and long-lasting respiratory acidosis in rats following the administration of diazepam 20 mg/kg subcutaneously, in association with methadone 5 mg/kg intraperitoneally, corresponding to one-tenth of the median lethal dose (LD50) of each drug. Gueye et al.[33,48] showed that a single intravenous dose of buprenorphine 30 mg/kg in rats did not result in any significant effect on blood gases, while, in combination with an intraperitoneal dose of midazolam 140 mg/kg, it induced a rapid onset of severe and sustained respiratory acidosis. Borron et al.[47] demonstrated, in a blinded randomised study, that flunitrazepam alters buprenorphine lethality in rats, with a 6-fold decrease of its intravenous LD50. However, the deleterious effect of the same dose of flunitrazepam was opioid-specific, as flunitrazepam caused only a 2-fold decrease in methadone LD50, with no significant effect on morphine LD50. The exact mechanism of buprenorphine/benzodiazepine interaction remains to be clarified, resulting either from a pharmacoki 2006 Adis Data Information BV. All rights reserved. 83 Table I. The different possible levels of a pharmacodynamic interaction between opioids (including buprenorphine) and benzodiazepines Interaction at the level of breathing control GABA and opioid receptors are co-expressed in the CNS including the brain stem[54] GABA and opioid receptors are implicated in the phasic and/or tonic activity of the neurons controlling the ventilation[55] There are common intracellular transduction pathways (Gi/o protein) regarding the GABAB and opioid receptors[56] Some benzodiazepines are antagonists of the delta and kappa receptors at high concentrations[57,58] Addition of various central and peripheral physiological effects (A + B) A. Benzodiazepines: command of the respiratory muscles and control of the pharyngeal dilatation, resulting in: (i) upper-airway obstruction in relation to relaxation of pharyngeal muscles; and (ii) diaphragmatic dysfunction[59] B. Opioids: reduction in the response to ventilation in different situations, including: (i) resistance during inspiration; (ii) hypoxia; and (iii) hypercapnia[60] netic or from a pharmacodynamic process. The majority of the studies analysing opioid/benzodiazepine interactions reported synergistic or at least additive hypnotic, analgesic and ventilatorydepressant effects based on pharmacodynamic interactions. Regarding the respiratory effects of the buprenorphine/ benzodiazepine combination, a pharmacokinetic mechanism cannot be excluded. Interestingly, in rodents, diazepam was demonstrated to inhibit the metabolism of methadone, even though such a kinetic interaction is lacking in humans.[49,50] Recent unpublished data obtained in our laboratory showed that buprenorphine significantly altered the kinetics of desmethylflunitrazepam, the metabolite of flunitrazepam, suggesting the likelihood of interaction of buprenorphine with the distribution of flunitrazepam (unpublished data). However in vitro studies failed to demonstrate any significant P450 cytochrome-mediated metabolic interactions between buprenorphine and flunitrazepam.[51,52] Moreover, in a study using cerebral microdialysis in rats, flunitrazepam pre-administration did not alter the distribution kinetics of buprenorphine in the striatum.[53] Thus, the main hypothesis regarding the respiratory effects of the buprenorphine/benzodiazepine combination relies on a pharmacodynamic basis. Different mechanisms of interaction regarding respiratory effects may be hypothesised due to common pathways and sites of action (table I). Opioids and benzodiazepines act in combination with different classes of the opioid and the GABA receptors. All these receptors are co-expressed in the CNS, including in the areas of ventilation control.[54] Both GABA and opioid systems play an important role in both phasic and tonic activity of the neurons that control the ventilation.[55] Interestingly, these receptors use comToxicol Rev 2006; 25 (2) 84 Mégarbane et al. mon intracellular transduction pathways such as the Gi/o protein.[56] Regarding opioid receptors, however, only limited interactions of benzodiazepines have been reported, especially at very high concentrations such as those observed after intrathecal administration.[57,58] Drug-induced coma involving benzodiazepines is characterised by snoring with flow limitation and obstructive apnoea.[59] The mechanism of respiratory insufficiency in nonintubated patients with drug-induced coma involving benzodiazepines is an increase in upper airway resistance and work of breathing. The interaction of sleep and opioid administration produces well known disturbances in the ventilatory pattern, causing profound oxygen destruction.[60] Regarding the buprenorphine/ benzodiazepine interaction, we suggest that buprenorphine may alter the response of the brain-stem respiratory centres to the benzodiazepine-induced increase in the upper-airway resistance. This hypothetic mechanism of interaction has yet to be elucidated and appropriate animal models and techniques, such as plethysmography, should be utilised to further our current understanding. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 5. Conclusion Buprenorphine is an efficient and safe maintenance therapy. Its marketing in several European countries was responsible for a significant decrease in heroin-associated deaths. However, due to diversion, misuse and co-ingestions of various other psychotropic drugs in addicts, the specific ceiling effect observed in clinical studies may be altered, resulting in severe respiratory depression and even death. To date, >100 deaths have been attributed to buprenorphine use in France, the UK and the Nordic European countries. A deleterious interaction between buprenorphine and benzodiazepines was hypothesised, based on experimental studies. It appears that this interaction is more likely to be a pharmacodynamic (additive or synergistic) than a pharmacokinetic interaction. However, the exact mechanism of buprenorphine respiratory toxicity remains to be determined. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. Acknowledgements The authors would like to acknowledge Dr Rebeca Gracia, PharmD, DABAT, from the North Texas Poison Center, Dallas, USA for her helpful review of this manuscript. No source of funds was used to assist in the preparation of this manuscript. The authors are not aware of any potential conflicts of interest directly relevant to the content of this review. 26. 27. 28. 29. References 1. Darke S, Zador D. Fatal heroin ’overdose’: a review. Addiction 1996; 91: 1765-72 2. Warner-Smith M, Darke S, Lynskey M, et al. Heroin overdose: causes and consequences. Addiction 2001; 96: 1113-25 3. Sporer KA. Buprenorphine: a primer for emergency physicians. Ann Emerg Med 2004; 43: 580-4 4. Auriacombe M, Fatseas M, Dubernet J, et al. French field experience with buprenorphine. Am J Addict 2004; 13 Suppl. 1: S17-28 5. Feroni I, Aubisson S, Bouhnik AD, et al. Collaboration between general practitioners and pharmacists in the management of patients on high-dosage bupre 2006 Adis Data Information BV. All rights reserved. 30. 31. 32. 33. norphine treatment: prescribers’ practices [in French]. Presse Med 2005; 34: 1213-9 Gueye PN, Mégarbane B, Borron SW, et al. Trends in opiate and opioid poisonings in addicts in north-east Paris and suburbs, 1995-99. Addiction 2000; 97: 1295-304 Emmanuelli J, Desenclos JC. Harm reduction interventions, behaviors and associated health outcomes in France, 1996-2003. Addiction 2005; 100: 1690-700 Reisine T, Pasternak G. Opioid analgesics and antagonists. In: Hardman J, Limbird L, Molinoff P, et al., editors. Goodman & Gilman’s the pharmacological basis of therapeutics. 9th ed. New York: McGraw-Hill, 1996: 521-55 Huang P, Kehner GB, Cowan A, et al. Comparison of pharmacological activities of buprenorphine and norbuprenorphine: norbuprenorphine is a potent opioid agonist. J Pharmacol Exp Ther 2001; 297: 688-95 Boas RA, Villiger JW. Clinical actions of fentanyl and buprenorphine: the significance of receptor binding. Br J Anaesth 1985; 57: 192-6 Boysen K, Hertel S, Chraemmer-Jorgensen B, et al. Buprenorphine antagonism of ventilatory depression following fentanyl anaesthesia. Acta Anaesthesiol Scand 1988; 32: 490-2 Elkader A, Sproule B. Buprenorphine: clinical pharmacokinetics in the treatment of opioid dependence. Clin Pharmacokinet 2005; 44: 661-80 Chang Y, Moody DE, McCance-Katz EF. Novel metabolites of buprenorphine detected in human liver microsomes and human urine. Drug Metab Dispos 2006; 34: 440-8 Obadia Y, Perrin V, Feroni I, et al. Injecting misuse of buprenorphine among french drug users. Addiction 2001; 96: 267-72 Comer SD, Collins ED, Fischman MW. Intravenous buprenorphine self-administration by detoxified heroin abusers. J Pharmacol Exp Ther 2001; 301: 266-76 Jenkinson RA, Clark NC, Fry CL, et al. Buprenorphine diversion and injection in Melbourne, Australia: an emerging issue? Addiction 2005; 100: 197-205 Robinson GM, Dukes PD, Robinson BJ, et al. The misuse of buprenorphine and a buprenorphine-naloxone combination in Wellington, New Zealand. Drug Alcohol Depend 1993; 33: 81-6 Reynaud M, Tracqui A, Petit G, et al. Six deaths linked to misuse of buprenorphine-benzodiazepine combinations. Am J Psychiatry 1998; 155: 448-9 Tracqui A, Kintz P, Ludes B. Buprenorphine-related deaths among drug addicts in France: a report on 20 fatalities. J Anal Toxicol 1998; 22: 430-4 Gaulier JM, Marquet P, Lacassie E, et al. Fatal intoxication following selfadministration of a massive dose of buprenorphine. J Forensic Sci 2000; 45: 226-8 Kintz P. Deaths involving buprenorphine: a compendium of French cases. Forensic Sci Int 2001; 121: 65-9 Kintz P. A new series of 13 buprenorphine-related deaths. Clin Biochem 2002; 35: 513-6 Pirnay S, Borron SW, Giudicelli CP, et al. A critical review of the causes of death among post-mortem toxicological investigations: analysis of 34 buprenorphineassociated and 35 methadone-associated deaths. Addiction 2004; 99: 978-88 Steentoft A, Teige B, Holmgren P, et al. Fatal poisoning in Nordic drug addicts in 2002. Forensic Sci Int 2006; 160 (2-3): 148-56 Schifano F, Corkery J, Gilvarry E, et al. Buprenorphine mortality, seizures and prescription data in the UK, 1980-2002. Hum Psychopharmacol 2005; 20: 343-8 Serfaty M, Masterton G. Fatal poisonings attributed to benzodiazepines in Britain during the 1980s. Br J Psychiatry 1993; 163: 386-93 Cowan A, Doxey J, Harry E. The animal pharmacology of buprenorphine, an oripavine analgesic agent. Br J Pharmacol 1977; 60: 547-54 Verborgh C, De Coster R, D’Haese J, et al. Effects of chlordiazepoxide on opioidinduced antinociception and respiratory depression in restrained rats. Pharmacol Biochem Behav 1998; 59: 663-70 McCormick GY, White WJ, Zagon IS, et al. Effects of diazepam on arterial blood gas concentrations and pH of adult rats acutely and chronically exposed to methadone. J Pharmacol Exp Ther 1984; 230: 353-9 Ohtani M, Kotaki H, Nishitateno K, et al. Kinetics of respiratory depression in rats induced by buprenorphine and its metabolite, norbuprenorphine. J Pharmacol Exp Ther 1997; 281: 428-33 Walsh SL, Preston KL, Stitzer ML, et al. Clinical pharmacology of buprenorphine: ceiling effects at high doses. Clin Pharmacol Ther 1994; 55: 569-80 Nielsen S, Taylor DA. The effect of buprenorphine and benzodiazepines on respiration in the rat. Drug Alcohol Depend 2005; 79: 95-101 Gueye PN, Borron SW, Risède P, et al. Lack of effect of single high doses of buprenorphine on arterial blood gases in the rat. Toxicol Sci 2001; 62: 148-54 Toxicol Rev 2006; 25 (2) Does High-Dose Buprenorphine Cause Respiratory Depression? 34. Dahan A, Yassen A, Romberg R, et al. Buprenorphine induces ceiling in respiratory depression but not in analgesia. Br J Anaesth 2006; 96: 627-32 35. Dahan A, Yassen A, Bijl H, et al. Comparison of the respiratory effects of intravenous buprenorphine and fentanyl in humans and rats. Br J Anaesth 2005; 94: 825-34 36. Molke Jensen F, Jensen NH, Holk IK, et al. Prolonged and biphasic respiratory depression following epidural buprenorphine. Anaesthesia 1987; 42: 470-5 37. Cicero TJ, Inciardi JA. Potential for abuse of buprenorphine in office-based treatment of opioid dependence. N Engl J Med 2005; 353: 1863-4 38. Rainey HB. Abuse of buprenorphine. N Z Med J 1986; 99: 72 39. Boyd J, Randell T, Luurila H, et al. Serious overdoses involving buprenorphine in Helsinki. Acta Anaesthesiol Scand 2003; 47: 1031-3 40. Gal TJ. Naloxone reversal of buprenorphine-induced respiratory depression. Clin Pharmacol Ther 1989; 45: 66-71 41. Ohtani M, Kotaki H, Uchino K, et al. Pharmacokinetic analysis of enterohepatic circulation of buprenorphine and its active metabolite, norbuprenorphine, in rats. Drug Metab Dispos 1994; 22: 2-7 42. Ohtani M, Kotaki H, Sawada Y, et al. Comparative analysis of buprenorphine- and norbuprenorphine-induced analgesic effects based on pharmacokinetic-pharmacodynamic modeling. J Pharmacol Exp Ther 1995; 272: 505-10 43. Mégarbane B, Marie N, Pirnay S, et al. Buprenorphine is protective against the depressive effects of norbuprenorphine on ventilation. Toxicol Appl Pharmacol 2006; 212: 256-67 85 49. Shah N, Patel V, Donald A. Effect of diazepam, desmethylimipramine, and SKF 525-A on the disposition of levo-methadone in mice after single or double injection. Drug Metab Dispos 1979; 7: 241-2 50. Pond SM, Tong TG, Benovitz NL, et al. Lack of effect of diazepam on methadone metabolism in methadone-maintained addicts. Clin Pharmacol Ther 1982; 31: 139-43 51. Ibrahim RB, Wilson JG, Thorsby ME, et al. Effect of buprenorphine on CYP3A activity in rat and human liver microsomes. Life Sci 2000; 66: 1293-8 52. Kilicarslan T, Sellers EM. Lack of interaction of buprenorphine with flunitrazepam metabolism. Am J Psychiatry 2000; 157: 1164-6 53. Mégarbane B, Pirnay S, Borron SW, et al. Flunitrazepam does not alter cerebral distribution of buprenorphine in the rat. Toxicol Lett 2005; 157: 211-9 54. Kalyuzhny AE, Dooyema J, Wessendorf MW. Opioid- and GABA(A)-receptors are co-expressed by neurons in rat brain. Neuroreport 2000; 11: 2625-8 55. Yamada KA, Norman WP, Hamosh P, et al. Medullary ventral surface GABA receptors affect respiratory and cardiovascular function. Brain Res 1982; 248: 71-8 56. Dan’ura T, Kurokawa T, Yamashita A, et al. Inhibition of rat brain adenylate cyclase activity by benzodiazepine through the effects on Gi and catalytic proteins. Life Sci 1988; 42: 469-75 57. Yanez A, Sabbe MB, Stevens CW, et al. Interaction of midazolam and morphine in the spinal cord of the rat. Neuropharmacology 1990; 29: 359-64 44. Gopal S, Tzeng TB, Cowan A. Characterization of the pharmacokinetics of buprenorphine and norbuprenorphine in rats after intravenous bolus administration of buprenorphine. Eur J Pharm Sci 2002; 15: 287-9 58. Cox RF, Collins MA. The effects of benzodiazepines on human opioid receptor binding and function. Anesth Analg 2001; 93: 354-8 45. Debruyne D, Quentin T, Poisnel G, et al. Acute and chronic administration of clorazepate modifies the cell surface regulation of mu opioid receptors induced by buprenorphine in specific regions of the rat brain. Brain Res 2005; 1052: 222-31 59. Gueye PN, Lofaso F, Borron SW, et al. Mechanism of respiratory insufficiency in pure or mixed drug-induced coma involving benzodiazepines. J Toxicol Clin Toxicol 2002; 40: 35-47 46. Quentin T, Debruyne D, Lelong-Boulouard V, et al. Clorazepate affects cell surface regulation of delta and kappa opioid receptors, thereby altering buprenorphine-induced adaptation in the rat brain. Brain Res 2005; 1063: 84-95 47. Borron SW, Monier C, Risède P, et al. Flunitrazepam variably alters morphine, buprenorphine, and methadone lethality in the rat. Hum Exp Toxicol 2002; 21: 599-605 48. Gueye PN, Borron SW, Risède P, et al. Buprenorphine and midazolam act in combination to depress respiration in rats. Toxicol Sci 2002; 65: 107-14 2006 Adis Data Information BV. All rights reserved. 60. Catley DM, Thornton C, Jordan C, et al. Pronounced, episodic oxygen desaturation in the postoperative period: its association with ventilatory pattern and analgesic regimen. Anesthesiology 1985; 63: 20-8 Correspondence and offprints: Bruno Mégarbane, Réanimation Médicale et Toxicologique, Hôpital Lariboisière, 2 Rue Ambroise Paré, 75010 Paris, France. E-mail: [email protected] Toxicol Rev 2006; 25 (2)