Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Orphan drug wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug interaction wikipedia , lookup
Psychopharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
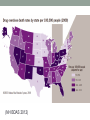
INTRODUCTION TO ADDICTION Benjamin R. Nordstrom, M.D., Ph.D. Assistant Professor of Psychiatry Geisel School of Medicine at Dartmouth Director of Addiction Services Dartmouth Hitchcock Medical Center Learning Objectives • Relate the disease model of addiction • Describe the three common variants of relapse • Describe how operant and classical conditioning relate to addiction • Understand how buprenorphine and methadone affect operant conditioning and treat addiction Drug use is common… • In 2011, 22.5 million people (8.7% of the U.S. population) were current users of illicit drugs. (SAMHSA 2012) • 8 % of the population met criteria for substance abuse or dependence (ibid) • 3% of the population will meet criteria for drug abuse or dependence at some point in their lives (Grant 1996) Drug use is common- cont’d • Painkillers are second only to cannabis in number of people meeting abuse or dependence criteria (1.8 million vs. 4.2 million) (SAMHSA 2012) • Between 2004 and 2011, the number with pain reliever dependence or abuse increased from 1.4 million to 1.8 million (ibid) Past Month Use of Selected Illicit Drugs among Persons Aged 12 or Older: 2002-2011 (SAMHSA 2012) Past Month Nonmedical Use of Types of Psychotherapeutic Drugs among Persons Aged 12 or Older: 2002-2011 (SAMHSA 2012) Past Year Initiates of Specific Illicit Drugs among Persons Aged 12 or Older: 2011 (SAMHSA 2012) Other Stats • U.S. has 4.6 % of the world’s population yet consumes 80% worlds opioids (Pain Physician 2010: 13:401-435 • The average mg/person use of opioids has increased 399% from 1997 to 2007 (ONDCP 2011) • Opioids account for 75% of prescription drugs being abused (ibid) • Retail pharmacies filled nearly 50% more Rxs for opioids in 2009 compared to 2000 (FDA via BDAS 2012) Source Where Pain Relievers Were Obtained for Most Recent Nonmedical Use among Past Year Users Aged 12 or Older: 2010-2011 (SAMHSA 2012) (NH BDAS 2012) (NH BDAS 2012) (NH BDAS 2012) (NSDUH 2008-2009 via NHBDAS 2012) (NH BDAS 2012) Addiction • Drug use starts out because it is pleasurable and/or helps avoid pain • Drug use pursued in such a way that negative consequences follow • Drug use persists in the face of negative consequences and the desire to quit (i.e. after it no longer “makes sense”) DSM IV: Substance Abuse Maladaptive pattern with significant impairment/distress For 12 months, at least 1 of the following criteria: Failure to fulfill major role obligations Use in physically hazardous situations Legal problems Recurrent social/interpersonal problems Never met Dependence Criteria DSM IV: Substance Dependence Maladaptive pattern of drug use for >12 months Must satisfy 3 of the following 7 criteria: • Tolerance • Withdrawal • More use than intended (loss of control) • Unsuccessful efforts to quit • Significant time spent in procurement, use, recovery • Functional impairment (social, occupational, recreational) • Continued use in the face of adverse health effects Classical Conditioning • Also called “associative learning” • Pavlov’s dogs • Conditioned stimulus + Unconditioned Stimulus Unconditioned Response • Conditioned stimulus Conditioned Response • Allows previously neutral stimuli to be imbued with hedonic salience Operant Conditioning • Reinforcement increases the frequency of a behavior • Positive reinforcement • the behavior makes a good feeling start • Negative reinforcement • the behavior makes a bad feeling stop Natural Rewards • Eating • Drinking • Sex • Certain behaviors • Nurturing • Aggression Cycle of Addiction Drug Euphoria + Brain Reward Neuroadaptations Drug Craving But not all users become addicted… • 17-22% (snorting vs. smoked) of people who try cocaine will go on to develop a dependence syndrome to it • 23% of people who try heroin will become addicted. • 9-10% of people who try cannabis will become addicted to it. • 15% of people who try alcohol will become alcoholics, • 32% of people who try cigarettes will become nicotine dependent. (Anthony, Warner et al. 1994) Routes of Administration Oral Intranasal Intravenous Intrapulmonary Intrapulmonary By-passes the venous system (Science 278:45-47, 1997) Disease Model of Addiction • It has identifiable symptoms. • It has a predictable course. • It has a treatment that is as successful as that of many chronic diseases (e.g diabetes, hypertension, asthma). • All addictive substances act an one area of the brain (the ventrotegmental tract or reward system) Disease model cont’d • Prolonged drug or alcohol use causes pervasive changes in brain function that persist long after the drug taking stops. • The addicted brain is distinctly different from the non-addicted brain as manifested in brain metabolic activity, receptor availability, gene expression and responsiveness to environmental cues. Relapse • Cue-induced relapse • Stress-induced relapse • Drug-induced relapse Cue induced relapse • Train a rat to self-administer drugs in a cage with a checkered floor • Extinguish the response • Reintroduce the rat to a checkered floor and it again attempts to self-administer drug • Human analogue: “People, places and things.” Stress-induced relapse • Train a rat to self-administer drugs • Extinguish the response • Give the rat a powerful foot shock and it will attempt to self-administer drug • Human analogue: “HALT” • (Hungry, Angry, Lonely, Tired) Drug-induced Relapse • Train a rat to self-administer drug • Extinguish the response • Give it drug unexpectedly and it will attempt to self-administer • Human analogue, “One is too many, and a thousand isn’t enough.” Opioid addiction • Tolerance develops quickly • Use gets perpetuated by…. • Positive reinforcement • Get euphoria (high) • Negative reinforcement • Get withdrawal when wears off • Withdrawal is pretty unpleasant Methadone Works on the same receptor (mu opioid receptors) as heroin and other abused opioids Can use it to taper people down Build a “chemical staircase” for them to walk down Can use it to maintain people as well Put on same dose of methadone as heroin Stops withdrawal Ratchet up dose to way past how much heroin they used Price it out of reach Stops positive and negative reinforcement Buprenorphine Pharmacodynamics • High affinity for the mu opioid receptor • Competes with other opioids and blocks their effects • Slow dissociation from the mu opioid receptor • Prolonged therapeutic effect for opioid dependence treatment • Long half life (20-44 hours) • Prevents negative reinforcement Efficacy: Full Agonist (Methadone) Partial Agonist (Buprenorphine), Antagonist (Naloxone) 100 Full Agonist (Methadone) 90 80 70 % Efficacy 60 Partial Agonist (Buprenorphine) 50 40 30 20 Antagonist (Naloxone) 10 0 -10 -9 -8 -7 Log Dose of Opioid -6 -5 -4 Mu opioid partial agonist • Ceiling effect imparts safety • Less respiratory depression • Less risk of overdose • Less physical dependence capacity Zubieta et al., 2000 Buprenorphine Maintenance/Detoxification • 52-week study, week 1 inpatient • Take home doses potentially allowed after 6 months • Outcome measures included - Treatment retention - Urine toxicology: three times per week, supervised - ASI scores Remaining in treatment (nr) Buprenorphine Maintenance/Detoxification: Retention 20 15 10 Detox/placebo 5 Buprenorphine 0 0 50 100 150 200 250 Treatment duration (days) 300 350 (Kakko et al., 2003) Buprenorphine Detox vs. Maintenance: Mortality Mortality Detox/Placebo Buprenorphine Cox regression 4/20 (20%) 0/20 (0%) c2=5.9; p=0.015 (Kakko et al., 2003) Buprenorphine Maintenance/Detoxification Kakko 2003 demonstrates: • Efficacy of maintenance treatment • Poor outcomes associated with detoxification (despite extensive psychosocial treatment after inpatient detoxification) Buprenorphine, Methadone, LAAM: Treatment Retention Percent Retained 100 80 73% Hi Meth (100mg/d) 60 58% Bup (32mg TIW) 40 53% LAAM (equiv 100mg/d) 20 20% Lo Meth (20mg/d) 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Study Week Adapted from Johnson, et al., 2000 Buprenorphine, Methadone, LAAM: Opioid Urine Results 100 Mean % Negative 80 LAAM (equiv 100mg/d) 60 Bup (32mg TIW) Hi Meth (100mg/d) 40 Lo Meth (20mg/d) 20 0 1 3 5 7 9 11 Study Week 13 15 17 Adapted from Johnson, et al., 2000 What is right for whom? Methadone Buprenorphine • Chronic pain • Jobs/ travel • Unable to manage • Live far from a methadone medication or infrequent visits • Need intense, “in-house” psychosocial interventions • Have failed buprenorphine program • No confounding issues THANKS!!!! • [email protected] • 603-653-1860