Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
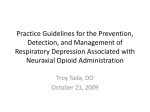
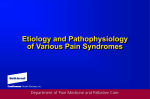
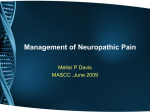
RECENT ADVANCES IN PAIN MANAGEMENT: RECENT ADVANCES IN PAIN MANAGEMENT DR.S.SREENIVASARAO MD,C.C.P.P.M, ASSIST PROFESSOR, DEPT.OF ANAESTHESIA, S.V.R.R.G.G.H.&S.V.M.C, TIRUPATI DR.S.SREENIVASARAO MD,C.C.P.P.M, ASSIST PROFESSOR, DEPT.OF ANAESTHESIA, S.V.R.R.G.G.H.&S.V.M.C, TIRUPATI What to discuss….: What to discuss…. BASICS IN PAIN PHARMACOLOGICAL ADVANCES NONPHARMACOLOGICAL ADVANCES Total care: Total care emotional spiritual physical social ‘‘Pain management continues to be the most difficult problem facing medicine today.’’ Jason R. Bauer and Charles E. Ray, Jr. WHY ………….? WHAT IS PAIN…….: WHAT IS PAIN……. DEFINITION : “ An unpleasant sensory and emotional experience associated with actual or potential damage or described in terms of such damage” - International Association for the Study of Pain, 1979 PAIN IS SUBJECTIVE REACTION TO AN OBJECTIVE STIMULUS WHAT THE PATIENT SAYS –”HURTS” PROPHYLACTIC TREATMENT: PROPHYLACTIC TREATMENT EVERY PERSON TALKS ABOUT P’ TO ATHEROSCLROSIS P’ TO M.I, P’ TO D.M, P’ TO HTN etc BUT NOT P’ TO PAIN …………..? REASONS FOR NOT TO TALK ARE……: REASONS FOR NOT TO TALK ARE…… WE ARE GIVING LEAST IMP TO PAIN OR WE ARE TREATING WHEN IT IS MORE DISTURBING LACK OF AWARENESS REGARDING PAIN CONSEQUENSES TYPES OF PAIN: TYPES OF PAIN DURATION ACUTE CHRONIC MODE OF MECHANISM NOCICEPTIVE NEUROPATHIC NEUROPATHIC PAIN: NEUROPATHIC PAIN ‘Pain arising as a direct consequence of a lesion or disease affecting the somatosensory system’ NEUP.PSIG-2008 ‘Pain caused by a lesion or disease of the somstosensary system’ IASP—2011 Common Neuropathic Pain Situations: Common Neuropathic Pain Situations Amputation - eg . Phantom limb pain Back, leg, and hip problems (Sciatica) CANCER and its treatment Diabetes Trigeminal neuralgia HIV infected or AIDS Herpes zoster virus infection Complex Regional Pain Syndromes Cerebro -Vascular Accident What Does Patient Complain of ? : What Does Patient Complain of ? Burning Numbness Paroxysmal Lancinating Shooting Raw Skin Feeling “ants crawling” “bag of worms” Hallmarks of Neuropathic Pain: Hallmarks of Neuropathic Pain Allodynia : Pain resulting from a stimulus that normally does not evoke pain. - Thermal or mechanical stimuli. Hyperalgesia : Something that is normally painful is now more painful than usual. Exaggerated response to a normally painful stimulus. Pain within area of injury - Primary Hyperalgesia Pain in surrounding undamaged area - Secondary Hyperalgesia PowerPoint Presentation: PAIN PATHWAYS WHAT HAPPENS WHEN TISSUE INJURY OCCURS…. : WHAT HAPPENS WHEN TISSUE INJURY OCCURS …. PRIMARY HYPERALGESIA SECONDARY HYPERALGESIA Central sensitization Peripheral sensitization PowerPoint Presentation: Serotonin, noradrenaline PERIPHERAL SENSITIZATION: PERIPHERAL SENSITIZATION In peripheral sensitization Cell injury arachidonic acid tissue acidity SP,CGRP Seratonin PG Leokotriens kallikrein,brdykinin k,Histamine Vasc.permeabilty Sensitizes nociceptor HTR LTR HYPERLAGESIA,ALLODYNIA PowerPoint Presentation: Peripheral sensitization Constant bombardment of the CNS with noxious input Noxious input processed by the CNS Pathophysiological consequences of acute pain Sensitization of the CNS response, called wind-up Induced sensitivity in the nervous system outlasts the stimulus Central sensitization : Central sensitization Central sensitization leads to a cascade of molecular events, such as Activation of the N-methyl-D- aspartate (NMDA) channel, Increase inintracellular Ca2+, Wind-up/wide dynamic range (WDR) neuron sensitization Central sensitization has several aspects : Increased spontaneous activity of dorsal horn neurons, Increased response to afferent input, Expansion of receptive field size, Reduction in threshold, Prolonged afterdischarges .( LONG TERM POTENTIATION) Reduced inhibitory controle in dorsal horns PowerPoint Presentation: 30% TOPIC OVER PENDING MANAGEMENT: MANAGEMENT LISTEN …..LISTEN….. LISTEN….. ASSESS EXAMINE IF NECESSARY INVESTIGATE CHOOSE THE CORRECT METHOD REASSESS REASSESS REASSESS PAIN ASSESSMENT: PAIN ASSESSMENT ACUTE PAIN ABLE TO COMMUNICATE VAS,NRS etc NOT ABLE TO COMMUNICATE FACES PAIN ASSESSMENT SCALE CHRONIC PAIN MC GILL PAIN QUESTIONNAIRE BRIEF PAIN IMPACT QUESTIONNAIRE(BPIQ ) IN CHILDREN CHEOPS , OPS, CRIES SCALE COMFORT SCALE ,N-PASS SCALE MANAGEMENT: MANAGEMENT PHARMACOLOGICAL >90% NONPHARMACOLOGICAL <10% INTERVENTIONAL NONINTERVENTIONAL WHO LADDER: WHO LADDER Modified WHO Analgesic Ladder: Pain Step 1 ± Nonopioid ± Adjuvant Pain persisting or increasing Step 2 Opioid for mild to moderate pain ± Nonopioid ± Adjuvant Pain persisting or increasing Pain persisting or increasing Step 3 Opioid for moderate to severe pain ± Nonopioid ± Adjuvant Invasive treatments Opioid Delivery Quality of Life Modified WHO Analgesic Ladder Proposed 4 th Step The WHO Ladder Deer, et al., 1999 PHARMACOLOGICAL: PHARMACOLOGICAL NSAIDS , COX-2 INHIBITORS OPIOIDS ANTICONVULSANTS ANTIDEPRESSANTS ANTIARRHYTHMICS ALPHA 2 ADRENERGIC AGONISTS STEROIDS MISCELLANEOUS –VASODILATORS,MUSCLE RELAXANTS, CAPSAICIN,RADIO ISOTOPES, BOTULINAM TOXIN(BOTAX),KETAMINE etc NSAIDS: NSAIDS Salicylates -Aspirin p-amino phenol derivatives - Paracetamol Propionic acid derivatives- Ibuprofen Acetic acid derivativesIndomethacin, Diclofenac,Ketorolac Oxicam derivatives- Piroxicam ,Meloxicom Fenamic acid derivatives- Mefeamic acid Cox-2 inhibitorsCelecoxib ,Valdecoxib Sulphonanilides- Nimmesulide Others- Licofelone PROSTAGLANDIN SYNTHESIS INHIBITORS: PROSTAGLANDIN SYNTHESIS INHIBITORS RISK STRATAGY WITH NSAID: RISK STRATAGY WITH NSAID IF ORAL NSAIDS ARE TAKEN FOR 2 MONTHS RISK OF ENDOSCOPIC ULCER IS 1 IN 5 SYMPTAMATIC ULCER IS 1 IN 70 BLEEDING ULCER IS 1 IN 150 DEATH FROM BLEEDING ULCER 1 IN 1300 TEXT BOOK OF PAIN,WALL&MELZACKS,CHAPTER30 IN NEONATES: IN NEONATES Renal toxicity, Necrotizing enterocolitis Platelet dysfunction, Hemorrhage (particularly intracranial hemorrhage) IN OUR PLACE (SVRRGGH): IN OUR PLACE (SVRRGGH) IN A RETROSPECTIVE STUDY REASONS FOR PERITONITIS(ULCER) ARE >95%--CHRONIC NSAID USE >2% ---TYPHOID >2%---TB ABDOMEN <1%---MALIGNANCY My Nsaid of choice: My Nsaid of choice Cox-2 inhibitors Paracetamol Cox-2 inhibitors: Cox-2 inhibitors Well tolerated compared with the NSAID regimens ( diclofenac 100 mg daily and naproxen 1000 mg daily). Successive Celecoxib Efficacy and Safety Studies (SUCCESS) showed that celecoxib was as effective as the conventional NSAIDs in controlling the pain Caused fewer GI ulcers or ulcer complications (such as perforations or bleeding) 29% less chance of having nausea 22% less chance of abdominal pain Increase risk for heart attack , thrombosis & stroke by a relative increase in thromboxane . PARACETAMOL: PARACETAMOL Central antinociceptive effect & potential mechanisms for this include inhibition of a CNS COX-2 Inhibition of a central cyclooxygenase ‘COX-3’ that is selectively susceptible to paracetamol , Modulation of inhibitory descending serotinergic pathways Prevent PG production at the cellular transcriptional level, independent of cyclooxygenase activity Extremely good safety profile at therapeutic doses Coadministration of paracetamol and alcohol is known to produce the hepatotoxic metabolite N -acetyl-p- benzoquinoneimine Causes none of the side-effects associated with opioids or indeed the gastrointestinal and platelet complications observed with NSAIDs Prevent ulcers by nsaids: Prevent ulcers by nsaids DICONTINUE NSAID WHENEVER POSSIBLE & CONSIDER ALTERNATIVE ANALGESIC(PCT) LOWER THE DOSE OF NSAID SWITCH TO COX-2 INHIBITOR PRECRIBE GASTRO PROTECIVE PROPHYLACTIC THERAPY--PPI OPIOIDS: OPIOIDS OPIOIDS: OPIOIDS Activating opioid receptors in the midbrain & turning on the Descending inhibitory system Activating opiod receptors on the second order pain transmission cells to prevent the Ascending transmission of pain signals Activating opioid receptors at the central terminals of C fibers in the spinal cord Activating opioid receptors in the periphary to inhibit the activation of nociceptors & to inhibit cells that may release inflmmatoy mediators OPIOID ANALGESICS: OPIOID ANALGESICS CLASSIFICATION AGONIST AGONIST -ANTAGONIST MORPHINE PENTAZOCINE CODEINE,OXYCODONE BUTORPHANOL DIHYDROCODEINE NALBUPHINE OXYMORPHONE DEZOCINE PETHIDINE ,METHADONE MEPTAZINAL HYDROMORPHONE FENTANYL PARTIAL AGONIST DIAMORPHINE(HEROIN) BUPRENORPHINE TRAMADOL TAPENTADOL ANTAGONIST NALOXONE NALTREXONE Routes of administration: Routes of administration Oral Intramuscular Intravenous Per rectal-suppositories Subcutaneous-patches Oral Transmucosal-lolly pops Inhalational Nasal spray COMPLICATIONS-OPIOIDS: COMPLICATIONS-OPIOIDS Initial Nausea and vomiting Drowsiness Unsteadiness Continuing: Constipation Nausea and vomiting Inactivity drowsiness Dry mouth Occasional: Urinary retention Myoclonus Itching TRAMODOL: TRAMODOL Opioid analgesic due to its weak binding of OP1,OP2,OP3 receptors Inhibits norepinephrine and serotonin uptake Both non- opioid and opioid mechanisms contribute to the antinociceptive effects of tramadol NO RESPIRATORY DEPRESSION sedation, nausea and constipation TAPENTADOL: TAPENTADOL Centrally acting analgesic with a unique dual mode of action as an agonist at the μ- opioid receptor & as a norepinephrine reuptake inhibitor 18-fold affinity for the μ opioid receptor in as compared to morphine Improved GI tolerability when compared to opioids Dose adjustment is not needed in the presence of renal impairment No Hepatoxicity Potency between Tramadol and Morphine Contraindicated in severe bronchial asthma, paralytic ileus , and patients on MAOI Anticonvulsants: Anticonvulsants Usefull in neuropathic pain Action : Suppress spontaneous neuronal discharge& hyperexcitability Depress the excitatory pathways, Facilitates the inhibitory mechanisms Drugs used : Carbamazepine , sodium valproate Carbamazepine : 100 - 200mg/day increased every third day by 100 mg up to 400 - 800 mg/day Side effects : gastric irritation, sedation, giddiness, ataxia, confusion Anticonvulsants: Anticonvulsants GABAPENTIN &PREGABALIN ACTION- Modulate the cellular Ca influx into nociceptive neurons by binding to vlotage gated Ca channels Preferred in Post Herpetic Neuralgia & Diabetic neuropathy Less side effects Expensive Gabapentin : Start with 200 to 300 mg/day , increase up to 1200 to 1800 mg/ day in divided doses. Pregabalin : Start with 75 mg 12Qh, increase by adding 75mg every 3 to 4 days, upto 300 mg Q12h Antidepressants: Antidepressants Particularly in burning type of pain ACTION Prevention of reuptake of serotonin&Norad Blockade of alfa ,H1 & NMDA receptors Block the effect of Na & Ca channels Enhancing descending inhibitory action in CNS Tricyclic antidepressants-AMITRYPTALINE Start with 10 to 25 mg at night and increase every 3rd day up to 75 to 100 mg if necessary Side effects sedation,constipation,urinary retention, heart block ANTIARRHYTHMICS : ANTIARRHYTHMICS ACTION Suppress hyperexcitability block glutamate-evoked activity in the dorsal horn of the spinal cord. Reduce ectopic discharges of injured nerves DRUG Orally for the treatment of chronic pain mexiletine INDICATIONS Post-stroke chronic pain, CRPS, Sympathetic dysfunction Peripheral diabetic neuropathy. SIDE EFFECTS Dizziness, Gait instability, Nausea and Vomiting LOCAL ANAESTHETICS: LOCAL ANAESTHETICS ACTION—BLOCK THE Na CHANNELS –IMPULSE CONDUCTION ROUTES— ORAL,INFILTRATION,SPINAL,EPIDURAL,SC PATCHES,TOPICAL etc A MAJOR DRAWBACK ANALGESIA TREATMENT IS TACHYPHYLAXIS DRUGS—LIGNOCAINE,BUPIVICAINE TOXIC EFFECTS –CNS & CVS ALPHA 2 ADRENERGIC AGONISTS: ALPHA 2 ADRENERGIC AGONISTS ACTION - BLOCKING THE TRANSMISSION OF NERVE IMPULSES TO THE BRAIN DECREASES THE RELEASE OF ADRENALINE &OTHER HORMONES THAT INCREASE BP ,HR, ANXIETY USED DRUGSCLONIDINE,DEXMEDITOMEDINE,TIZANIDINE SIDE EFFECTS BLURRED VISION DIZZINESS, DRY MOUTH,DRY EYES, SKIN IRRITATION, CONSTIPATION BE CAUTIOUS PTS WITH CONDUCTION BLOCKS,ARRHYTHMIAS,OLD AGE STEROIDS: STEROIDS COMMANLY USED ARE DEXAMETHASONE,TRIAMCINALONE,METHYLPREDNISOLONE.BETAMETHASONE ACTION MEMBRANE STABILISATION, BLOCKADE OF PHOSPHOLIPASE-2 ACTIVITY, PROLONGED SUPPRESSION OF ONGOING NEURONAL DISCHARGE, SUPPRESSION OF SENSITISATION OF DORSAL HORN NEURONS, ANTIOEDEMA ACTIVITY SIDE EFFECTS SUPPRESSION OF HPA AXIS,PEPTIC ULCER DISEASE,OSTEOPOROSIS,SKELETAL MUSCLE MYOPATHY etc Botulinam toxin(botax-a,b): Botulinam toxin( botax-a,b ) ACTION- Inhibition of ach release, Inhibition of the release of glutamate, substanceP , and CGRP Reduced afferent input to the CNS through effects of the toxins on muscle spindles INDICATIONS — Strabismus, Blepharospasm , Hemifacial spasm, Cervical dystonia , Glabellar wrinkles. Headache, Muskuloskeletal Pain BOTAX: BOTAX SIDE EFFECTS- Pain, muscleweakness , Flulike syndrome Autonomic side effects appear to be commonly seen with type B toxin CONTRAINDICATIONS – Pregnancy (category C), Concurrent use of aminoglycoside , Myasthenia gravis,Eaton –Lambert Known sensitivity to the toxins MISCELLANEOUS: MISCELLANEOUS VASODILATORS - RAYNAUD’S PHENOMENON BUERGERS DISEASE,CRPS etc DRUGS ARE NIFEDIPINE,XANTHINOL NICOTINATE,PENTOXYPHYLLINE MUSCLE RELAXANTS ACUTE MUSCLE SPASM, FIBROMYALGIA,NOCTURNAL LEG CRAMPS DRUGS ARE- TIZANIDINE,BACLOFEN,DANTROLENE,DIAZEPAM MISCELLANEOUS: MISCELLANEOUS CAPSAICIN- NOCICEPTIVE, NEUROPATHIC PAIN RADIOISOTOPES -USED IN CANCER METS INTRAVENOUS INFUSION THERAPY -NEUROPATHIC PAIN DRUGS ARELIDOCAINE,KETAMINE,PHENTOLAMINE,MAGNESIUM,ADENOSINE,PAMIDRONATE,ALFENTANYL CHEMOTHERAPY PowerPoint Presentation: >60% TOPIC OVER PENDING INERVENTIONAL: INERVENTIONAL 1 . SPINAL & EPIDURAL OPIOID & STEROID 2. PNS,SCS & DBS 3. NEUROLYSIS-Chemical neurolysis , Radiofrequency thermocoagulation Cryoanalgesia 4.VERTEBROPLASTY & KYPHOPLASTY 5.DRY NEEDLING,INFILTRATION,PROLOTHERAPY,TPI 6.ACCUPUNCTURE 7.RADIOTHERAPY 8.OZONETHERAPY 9. CAUDAL EPIDURAL DECOMPRESSIVE NEUROPLASTY (LYSIS OF ADHESIONS) 10.PERCUTANEOUS MANAGEMENT OF VISCERAL PAIN 11.NEUROSURGICAL PROCEDURES EQUIPMENTS USED ARE….: EQUIPMENTS USED ARE…. FLUOROSCOPIC GUIDED ULTRASOUND GUIDED CT GUIDED MRI GUIDED SPINAL CORD STIMULATION: SPINAL CORD STIMULATION Relieves pain by applying sufficient electrical stimulation to cause paresthesias covering or overlapping the area(s) of pain without discomfort or motor effects MECHANISM OF ACTION- “gate control theory of pain,” PowerPoint Presentation: INDICATIONS - Failed back surgery syndrome, Ischemic pain of peripheral vascular disease Postcordotomy dysesthesias , “Reflex sympathetic dystrophy Phantom limb and stump pain. CONTRAINDICATIONS Coagulopathy , Sepsis, Serious drug behavior problems, Inability to cooperate or to control the device Demand cardiac pacemaker (without ECG monitoringor changing the pacemaker mode to a fixed rate), MRI needs PowerPoint Presentation: COMPLICATIONS Generator failure Electrode fatigue fracture, Electrode migration/ malposition Exposure to electromagnetic fields ( eg , diathermy,security systems) Spinal cord or nerve injury, CSF leak, Infection,Bleeding RADIOFREQUENCY ABLATION: RADIOFREQUENCY ABLATION ACTION Destruction of the nerves that signal pain The effect of RF on tissue depends on the temperature generated: >45°C, irreversible tissue injury occurs; Between 42 and 45°C, temporary neural blockade occurs. INDICATIONS HEAD AND NECK PAIN , SPINE PAIN , NEUROPATHIC PAIN RFA: RFA COMPLICATIONS Neurologic deficits from the intended target or nearby neural structures, Deafferentation pain, neuritis, Burn injury at breaks in the needle insulation, Hematoma,and infection CRYONEUROLYSIS: CRYONEUROLYSIS Temporarily destroys a nerve through the application of extreme cold. The extreme cold degenerates the nerve axons without damaging surrounding connective tissue Larger myelinated fibers cease conduction at 10°C, At 0°C, all nerve fibers entrapped in the ice ball stop conduction. CRYO….: CRYO…. INDICATIONS POSTTHORACOTOMY PAIN, POSTHERNIORRHAPHY PAIN INTERCOSTAL NEURALGIA, PAINFUL NEUROMA CERVICAL AND LUMBAR FACET AND INTERSPINOUS LIGAMENT PAIN COCCYDYNIA, PERINEAL PAIN ILIOINGUINAL, ILIOHYPOGASTRIC, AND GENITOFEMORAL NEUROPATHIES SUPERIOR GLUTEAL NERVE NEURALGIA CRANIAL NEURALGIA, SUPRAORBITAL NERVE NEURALGIA INFRAORBITAL NEUROPATHY, MANDIBULAR NEUROPATHY VERTEBROPLASTY : VERTEBROPLASTY L2 KYPHOPLASTY: KYPHOPLASTY CAUDAL EPIDURAL DECOMPRESSIVE NEUROPLASTY (LYSIS OF ADHESIONS): CAUDAL EPIDURAL DECOMPRESSIVE NEUROPLASTY (LYSIS OF ADHESIONS) Indications Failed back surgical Disc disruption Mets of spine compression fracture Multilevel degenerative arthritis Epidural scarring following infection or meningitis Pain unresponsive to spinal cord stimulation Pain unresponsive to spinal opiods Contraindications Sepsis Coagulopathy Local infection at the site of the procedure Patient refusal PowerPoint Presentation: Immediate complications Bleeding in the epidural space Bending of the tip of the needle Penetration of the Dura Subdural insertion of the catheter Shearing of the catheter Hypotension Late complications Penetration of the Dura Numbness in the dermatomal distribution Temporal anesthesia Permanent paresthesias Bowel and bladder dysfunction Sexual dysfunction Headache Infection at the site of penetration Epidural abscess Arachnoiditis Percutaneous Management of Visceral Pain: Percutaneous Management of Visceral Pain CELIAC PLEXUS BLOCK Distal esophagus, stomach, duodenum, smal intestine, colon, adrenal glands, Kidneys, proximal ureters , pancreas, spleen, liver, biliary system, andmajor blood vessels PowerPoint Presentation: HYPOGASTRIC PLEXUS BLOCK Distal ureters , gonads, sigmoidcolon , vagina, rectum, bladder, perineum, vulva, prostate, uterus, and the major pelvic blood vessels PowerPoint Presentation: DRYNEEDLING, INFILTRATION, PROLOTHERAPY, TPI ACCUPUNCTURE RADIOTHERAPY OZONETHERAPY Neurosurgical Pain Therapies: Neurosurgical Pain Therapies Ablative Neurectomy Sympathectomy Ganglionectomy Rhizotomy Spinal DREZ lesioning Cordotomy Myelotomy Nucleus caudalis DREZ lesioning Trigeminal tractotomy Mesencephalotomy Thalamotomy Cingulotomy Hypophysectomy Augmentative Peripheral nerve stimulation Spinal cord stimulation Thalamus (PVG-PAG) stimulation Motor cortex/deep brain stimulation Intrathecal /epidural drug infusion Intraventricular drug infusion NON INTERVENTIONAL: NON INTERVENTIONAL PHISIOTHERAPY ELECTROTHERAPY COLD THERAPY, HEAT THERAPY, ULTRASOUND, TENS MANIPULATIVE THERAPY MASSAGE, SPINAL TRACTION, PASSIVE STRETCHING, ORTHOSES(CERVICAL COLLARS,LUMBAR SUPPORTS) HYDROTHERAPY NON INTERVENTIONAL: NON INTERVENTIONAL MEDITATION, HYPNOSIS, BIOFEEDBACK, BEHAVIOURAL THERAPY POSTURE PHYSICAL EXERCISES DIET THERAPY How can you treat pain ?: How can you treat pain ? TAKE HOME MESSAGE: TAKE HOME MESSAGE T H A N K Y O U MANY MECHANISMS SO MANY METHODS