Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
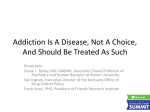
Opioid Overdose and Cardiac Arrest Joseph Yanta, MD Clinical Assistant Professor, Division of Medical Toxicology, Department of Emergency Medicine, UPSOM Assistant Medical Director, Pittsburgh Poison Center Presenter Disclosure Information Joseph H. Yanta, MD Opioid Overdose and Cardiac Arrest Financial Disclosure: No relevant financial relationship exists Session Objectives • Understand the incidence and prevalence of opioid-related death • Understand how outcomes after opioidrelated out-of-hospital cardiac arrest (OOHCA) differ from non-opioid-related OOHCA • Understand other cardiac-related consequences opioids and opioid abuse Game Plan • • • • • • Epidemiology Pathophysiology Prognosis Opioid-induced dysrhythmia Drug adulterants and cardiovascular pathology Challenges in drug testing Definitions • Opiate = alkaloid with opioid receptor binding derived from the poppy plant – Morphine – Codeine – Thebaine • Opioid = an agonist of opioid receptors – Semisynthetic: heroin, hydromorphone, oxycodone, etc. – Synthetic: fentanyl, methadone, tramadol, etc. • Opiate is to opioid as square as rectangle • Narcotic includes opioids as well as all other illegal drugs Opioid Death Epidemiology • 19,000 deaths per year due to prescription opioid overdose Drug overdose death involving opioids, by type of opioid, United States, 2000-2014 – 52 deaths deaths per day • More than 10,500 deaths per year due to heroin – 29 deaths per day • More people die from opioid overdose than either car accidents or gun violence • Available data likely underestimate true number of deaths www.cdc.gov/drugoverdose/data/analysis.html Opioid Death Epidemiology • Pennsylvania had the 8th-highest rate of drug overdose deaths in 2014 – 21.9/100,000 – 2,732 deaths overall • West Virginia had the highest Opioid Death Epidemiology • Allegheny County Data – 2015: 424 opioid overdose deaths • 70% men • 86% white • 28% between ages 25-34 – 37% increase compared to 2014 • 234 deaths so far in 2016 (as of July 31) Opioid Death Pathophysiology • Opioid agonism of m2-opioid receptors results in respiratory depression • Death due to asphyxiation and subsequent cardiovascular collapse and arrest • Complicated by: ischemic liver/kidney injury, rhabdomyolysis, aspiration pneumonitis, pulmonary edema Opioid Overdose and OOHCA • Scant data exist comparing opioid- and nonopioid-related OOHCA • Elmer J, Lynch MJ et al. Recreational Drug Overdose-related Cardiac Arrests: Break on Through to the Other Side. Resuscitation. 2015; 89:177. Opioid Overdose and OOHCA • Patients suffering overdose-related OOHCA (compared to non-overdose-related) are: – Younger – Healthier at baseline • More likely to present with a non-shockable rhythm, i.e. PEA or asystole • More likely to have worse initial neurologic examination • Survival, neurologic outcomes, length of stay do not differ from non-overdose-related subjects – Despite poorer initial neurologic examination Post-Arrest Management • Little data exist to differentiate post-arrest management of the poisoned patient from the non-poisoned patient • Aggressive temperature control (euthermia) is still (probably) beneficial • Consideration for coronary disease in appropriate patients Post-Arrest Challenges • • • • Neuroprognostication Hypothermia drug kinetics Withdrawal syndromes Management of multisystem organ injury – Rhabdomyolysis – Acute liver injury – Acute kidney injury Challenges in Drug Testing • Urine drug immunoassays imply presence of drug, not causation • “Opiate” screen = morphine screen – Heroin metabolized to morphine • Positive screen does not prove causality • Negative screen does not disprove causality • So, the basic urine drug immunoassay screen is USELESS Negative on “Opiate” Urine Drug Immunoassay Methadone Fentanyl (and derivatives) Buprenorphine Oxycodone (often) Hydrocodone (sometimes) Oxymorphone Tramadol Opioid-Associated Dysrhythmia • Propoxyphene – essentially unavailable in the United States – Sodium channel blockade • Methadone – Doses >100 mg/day associated with increased risk of sudden death – Inhibits Ikr resulting in QT prolongation Drug Adulteration • Adulterant = intentional inclusion of xenobiotic in drug sample for dilution, synergistic, or maleficent intent • Contaminant = unintentional inclusion of a xenobiotic, usually as result of poor laboratory technique – E.g. lead, other heavy metals, codeine, MPTP CV-Active Drugs as Adulterants • • • • • Quinine/quinidine Diltiazem Verapamil Lidocaine Caffeine • • • • Procaine Atropine Arsenic Clenbuterol UPMC Medical Toxicology Service via MedCall: 412.647.7000 Thank you for your attention! Questions?