Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
MINISTRY OF HEALTH OF THE REPUBLIC OF UZBEKISTAN
TASHKENT MEDICAL ACADEMY
"CONFIRM"
Vice Rector of TMA
Professor Teshaev O.R.
_______________________
"27" august 2015.
Department: FACULTY AND HOSPITAL SURGERY of
MEDICAL FACULTY
Subject: Hospital Surgery
TECHNOLOGY of TRAINING
on a practical lesson on the topic:
« ESOPHAGEAL DISEASE»
Таshkent 2015
Compiled
Professor Hakimov M.Sh.
Docent Imamov A.A.
Assistant Khalikov S.P.
Technology training approved:
At the faculty meeting protocol №1 of "27" august 2015
Topic: ESOPHAGEAL DISEASE
Model learning technology in the classroom
Time – 6 hour
Form of lesson
Number of students: 8-12 pers.
Practical session in the clinic and workshop using
brain storming and web
- Chair of faculty and hospital surgery; an educational
Venue classes
room, chamber, dressing
- Posters, tables, schemes of classification of disease,
the scheme of treatments, roentgenograms, video
films.
1. introduction
Structure of the
2. The practical part
training sessions
- Super vision of patients
- Implementation of practicals kills
- Discussion of the practical part
3. The theoretical part
- Discussion of the theoretical part
4. assessment
Evaluation of teacher
5. Conclusion teacher. Assessment of Knowledge.
Providing questions relating to the next class (see for
rotation).
The purpose of the training session: Substantiation of a theme with instructions
of the importance for vocational training of students. Acquaintance of students to
gullet diseases, the reasons of their development, features of a clinical current, a
current of the complicated forms, differential diagnostics, optimum methods of
treatment, conducting the postoperative period, rehabilitation of patients.
1. Clinical variants of Learning outcomes:
various forms PTFB.
GPs should know:
2. Methods of diagnosis 1. To give concept about gullet diseases.
and differential diagnosis 2. To explain the reasons and mechanisms of
of complications.
development of complications.
3. Special methods of 3. To give the clinical characteristic and possible
examination of patients
variants of a current of disease.
4. Correctly interpret the 4. To carry out differential diagnostics with other
results of instrumental diseases.
diagnostic studies to 5. To acquaint students with modern and most
substantiate the diagnosis informative methods, inspections of patients
and treatment of rational 6. Demonstration of examples of their surgical
choice.
practice: patients, slides, radiological researches.
5. Features preoperative 7. All material of employment to prepare and present
preparation of these
patients.
6. Nature of surgical
interventions
and
medical treatment, to
know their features.
7. Methods to prevent
complications during and
after surgery.
Methods and
techniques of training
Learning Tools
Forms of learning
Conditions of Learning
Monitoring an
devaluation
to students, in the volume necessary for qualitative
preparation of the general practitioner.
GPs should be able to:
- To execute practical skills - to get certain practical
skills in inspection of patients with esophagus
diseases, to carry out inspections of the given patients
special by methods, to define indications and
contraindications to surgical interventions.
Academic controversy, black box, web, graphic
organizer - a conceptual table
Manuals, training materials, slides, video and audio,
medical history
Individual work, group work, collective
Audience Chamber, training room, operating room,
dressing
Interpreting control: control issues, perform
educational tasks in groups, perform practical skills
CDS
2. Motivation
Suggestion to students of necessity of timely adequate operation before
development of terrible complications, and at their development - acquaintance to
the most informative and modern methods of diagnostics, surgical treatment of
patients, acquaintance to possible complications out of operation and the
operational period, them, preventive maintenance. Development of clinical
thinking of students.Modern view development on a problem of a question from a
position to world medicine and the general practitioner.
3. Intersubject and intrasubject communications
Teaching of the given theme is based on knowledge students of bases of
anatomy, normal and pathological physiology. The knowledge received during
employment will be used at passage of gastroenterology by them, internal illnesses
and other clinical disciplines.
4. The employment maintenance
4.1. Theoretical part
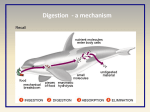
ANATOMICAL AND PHYSIOLOGICAL FEATURES.
Esophagus - a muscular tube that begins as a continuation of the pharynx and
ends cardio. It is located in the midline, but is deflected to the left in the bottom of
the neck and back to the center line near the carina. The lower chest esophagus
again deflected to the left and passes through a hiatal.
There are 3 areas of physiological narrowing of the esophagus. The top is
caused by narrowing of the cricopharyngeal muscle. Average narrowing due to the
intersection of the left main bronchus and aortic arch. The lowest restriction is due
to gastro-esophageal sphincter. This restriction can delay the ingestion of foreign
bodies and corrosive liquids because of their slow passage through these areas.
Cervical esophagus has a length of about 5 cm, and descends between the
trachea and the spine to a level front suprasternal notch. Recurrent laryngeal nerves
are in the right and left furrows between the trachea and the esophagus. On the left
and right sides of the cervical esophagus are the fascia of the carotid arteries and
thyroid lobe. The length of the thoracic esophagus is approximately 20 cm. The top
of the chest esophagus tightly in contact with the rear wall of the trachea and
prespinal fascia. Lower down on the bifurcation of the trachea are the vagus nerves
and esophageal nerve bundle located in close contact with the vertebral bodies. The
thoracic cavity thoracic duct is behind the esophagus, azygos vein between the
right and descending part of the thoracic aorta to the left. Abdominal esophagus
has a length of about 2 cm. This part of the esophagus is under positive pressure
medium abdomen.
Esophageal musculature consists of an external longitudinal and internal
circular layers. Upper esophagus (2-6 cm) contains only the striped muscle fibers.
Below this level, the esophagus is gradually becoming richer smooth muscle fibers.
Clinically, the most important violations of esophageal peristalsis involve only the
smooth muscles of the lower two thirds of the esophagus. The circular muscle
layer of the esophagus is thicker than the outer longitudinal layer. The structure is
similar to the circular muscle helix, resulting in esophageal peristalsis a vermicular
movement, in contrast to the segmental and sequential compression.
Cervical esophagus supplied with blood mainly from the inferior thyroid
artery. Thoracic receives blood supply from the bronchial arteries. Two esophageal
branches depart directly from the aorta. Abdominal esophagus receives blood
supply from the ascending branch of the left gastric artery and from the lower
diaphragmatic arteries. In the initial part of the esophagus artery formed in the
longitudinal beam, which increases the intramural vascular network in the muscle
and that submucosal layers. Esophageal veins empty into the inferior thyroid vein
in bronchial unpaired or hemiazygos, as well as in the crown of Vienna. Venous
plexus submucosal layer of the esophagus and stomach are in close connection
with each other and with the portal venous obstruction of the communication
functions as collateral for the blood flowing in the superior vena cava through the
azygos vein.
The parasympathetic innervation of the pharynx and esophagus is carried out
mainly through the vagus nerves. Cricopharyngeal sphincter and cervical
esophagus receive branches, from both recurrent laryngeal nerves. Damage to
these nerves violate not only the function of the vocal cords, but also the function
of cricopharyngeal sphincter, predisposing to pulmonary aspiration.
Visceral sensory afferent pain fibers esophagus complexed vagal and
sympathetic pathways also anatomically combined with visceral afferent sensory
fibers emanating from the heart. Hence, both bodies have similar symptomatology.
The lymphatic system is located in the submucosal layer of the esophagus,
small enough and consists of a submucosal plexus. Lymph flow runs in the
longitudinal direction. In the upper two thirds of the esophagus lymph moves
mainly in cephalic direction in the lower third - in the caudal.
Classification of diseases of the esophagus
1. Malformations:
1. Congenital esophageal atresia and esophagotracheal fistulas.
2. Congenital esophageal stenosis.
3. Congenital diaphragm membrane of the esophagus.
4. Congenital short esophagus.
5. Congenital esophageal cyst.
6. Anomalies vessels.
2. Damage:
1. Traumatic injuries: external and internal
2. Burns of the esophagus and their consequences
3. Diseases of the esophagus:
1. Diverticula: pulsion and traction
2. Inflammatory diseases: esophagitis
4. Tumors of the esophagus:
1. Benign tumors
2. Malignant tumors
5. Violation of esophageal motility (cardiospasm):
1. Achalasia
2. esophageal spasm.
Malformations of the esophagus
Detectability: found 1 in 7-8 million newborns. The most common complete
esophageal atresia combined tracheobronchial fistula: a proximal end of the
esophagus connected to the distal trachea.
Less common complete esophageal atresia without tracheobronchial fistula.
Clinic: the disease appears at birth. If swallowed newborn saliva, colostrum,
the liquid instantly arises respiratory failure, cyanosis. At full atresia without
esophagotracheal fistulas at the first feeding occurs belching, vomiting.
Diagnosis:
Clinical manifestations
Probing the esophagus,
The contrast study of the esophagus with Gastrographine
Panoramic radiographs of the thoracic and abdominal cavity: signs of
atelectasis areas, signs of pneumonia (aspiration), the absence of gas in the
intestines. Gas in the intestines may be the case if there is a connection of the lower
segment of the esophagus with the trachea (fistula).
Treatment: If there are no signs of atelectasis, pneumonia - simultaneous
operations esophagotracheal fistulas closure and anastomosis of the upper and
lower segments of the esophagus. If the disease is complicated by aspiration
pneumonia, atelectasis in the lungs is carried out following treatment: in the
beginning impose gastrostomy, intensive therapy to improve, and then close the
fistula and make anastomosis between the upper and lower segment of the
esophagus.
When multiple malformations in newborns severely weakened output of the
esophagus to the proximal end of the neck, to avoid the accumulation of saliva in
it, and imposed gastrostomy feeding. After a few months of performing an
anastomosis. If it is impossible to compare the upper and lower segments of the
esophagus perform plastic.
Congenital esophageal stenosis
Typically, a stenosis is located at the level of the aortic constriction. Clinic:
hiatal hernia, esophagitis, achalasia. With a significant narrowing of the esophagus
occurs suprastenotic expansion of the esophagus. Symptoms usually do not appear
until the introduction of solid baby food diet food.
Diagnosis: Clinical manifestations, EGDF-scopy and contrast study of the
esophagus.
Treatment: In most cases, the expansion by dilation of the esophagus or
bougienage. Surgical treatment is carried out in an unsuccessful conservative
treatment.
Congenital diaphragm membrane of the esophagus
The diaphragm consists of connective tissue, covered with keratinizing
epithelium. In this diaphragm often have holes through which can penetrate the
food. Almost always localized in the upper part of the esophagus, much less - an
average of department.
Clinic: the main clinical manifestation is dysphagia, which occurs when
administered in the diet of the child solid food. When large holes in the membrane
of food can fall into the stomach. Such patients are generally all thoroughly chew
than prevent jamming of food in the esophagus. The membrane under the influence
of food debris often inflamed
Diagnosis: Clinical manifestations, a contrast study of the esophagus.
Treatment: the gradual expansion of the esophagus probes of different
diameters. When the diaphragm completely covers the clearance necessary to
remove it under endoscopic control.
Congenital short esophagus
It is believed that the in utero development of the esophagus has been slow,
and part of the stomach, penetrating through the diaphragm forms a lower part of
the esophagus. Congenital short esophagus occurs in Marfan's syndrome, found
familial cases of the disease. Clinic: clinical manifestations are similar to those of
the sliding hiatal hernia - pain in the chest after eating, heartburn, vomiting can be.
Diagnosis: Clinical manifestations, often differentiate congenital short
esophagus from sliding hiatal hernia can only be surgery, EGDF-skopy.
Treatment: symptomatology - surgical, usually in the absence of adhesions
esophagus and the aorta can restore the normal position of the esophagus and
stomach by stretching it.
Congenital esophageal cyst
Cysts are placed intramural, paraesophageal. These are lined with bronchial
cysts, esophageal epithelium.
Clinic: cysts in children can cause cough, dysphagia, respiratory failure,
cyanosis. In adults cysts usually less than 4 cm, 4 cm if the clinical symptoms is
the same as in leiomyomas. Cysts can mediastinitis complicated by infection,
bleeding and malignancy.
Treatment: removal of a cyst in the fibrogastroscopy.
Traumatic injuries to the esophagus
Classification:
Internal (closed) - Damage from the mucosa.
Outdoor (open) by connective membrane or peritoneum. As a rule,
accompanied by damage to the body when the skin wounds of the neck, chest and
abdomen.
Etiological factors:
Iatrogenic diagnostic and therapeutic measures (EGDF, probing, and
nasogastric intubation cardiodiosis GIT), tracheostomy, intubation.
Esophageal injury during operations on the thorax, neck and stomach.
Foreign bodies.
Diseases of the esophagus, leading to perforation of its wall (tumors, ulcers,
burns, etc.).
Ruptures of the esophagus most often occur after vomiting (75%), and cough
stress syndrome Mallory-Weiss - gap esophageal mucosa that is manifested by
bleeding after a severe attack of vomiting. Surgical intervention is required in 10%
of cases; Boerhaave syndrome (syndrome Boerhaven) usually occurs above the
transition of the esophagus into the stomach. The diagnosis proves to be true
presence of air in the left mediastinum. Shown immediate surgery.
Injuries to the neck, chest, abdomen, caused a cold or firearms.
Ruptures of the esophagus closed body injuries.
There are full and partial damage to the esophagus. Incomplete damage to the
gap in the range of one or more shells, but not the entire thickness of the body.
Full damage - the entire depth of the wall of the organ. With the localization
in the cervical region is developing retroesophageal or necrotic abscess of the
neck; thoracic - mediastenit, while damage of the pleura - pleural effusion, the
pericardium - pericarditis, in the abdomen - peritonitis.
Clinic:
1. Pain along the esophagus.
2. Foreign body sensation in the esophagus.
3. Hypersalivation.
4. bloody vomit.
5. Subcutaneous emphysema.
6. Salivation through injury.
Diagnostics. X-rays: Review angiography (emphysema or mediastinal tissue
neck hydropneumothorax, pneumoperitoneum).
Contrast radiography (on the back side, on your stomach) - Define the size of
the defect and its location. EGDF-scopy under anesthesia.
Treatment. Conservative: complete exclusion of enteral nutrition, drug
correction of homeostasis, antibiotics directed action. Surgery: removal of the
defect.
• Radical surgery: the removal of a defect in the wall of the esophagus and
drainage circumesophageal fiber whatever access.
• Palliative operations: depending on the level of damage to perform drainage
cellulitis: the cervical and thoracic level to Th4-Th5 - mediastinotomy neck side. In
the lower third of the thoracic esophagus - the lower transabdominal
mediastinotomy by Savinykh. Gastrostomy performed postoperatively to facilitate
supply of the patient.
Foreign bodies of the esophagus
Various objects caught in the lumen of the esophagus or stomach, and often
unable to manually remove these bodies.
Causes: Foreign bodies can enter the esophagus and stomach during a meal or
as a result of accidental ingestion are in the mouth of various items (pins, needles,
nails). Children often swallow coins, toys, buttons. In the elderly into the
esophagus and the stomach can get dentures. Patients with mental disorders are
swallowed spoons, forks, and other items. As the foreign body can be fish or meat
bones. It is not uncommon stuck in the esophagus of large pieces of meat. Most
often this occurs when the influence of alcohol and the elderly. The development
of the disease - the fixed foreign bodies in the esophagus causing inflammation of
its walls, violate swallowing. Foreign body of the esophagus can lead to
compromise the integrity of its walls, threatening death. In the presence of foreign
bodies, they may be the stomach for a long time does not manifest itself, however,
will eventually lead to various complications such as the formation of gastric
ulcers, its obstruction, bleeding.
Clinic:
1. Fear.
2. constant pain when swallowing or localized: in the throat, in the jugular
fossa, behind the breastbone.
3. Dysphagia caused by a spasm of the muscles of the esophagus and
inflammatory edema of its mucosa.
4. Regurgitation, until the complete obstruction of the esophagus.
Diagnosis: the presence of foreign bodies established on the basis of the story,
and patient complaints. Objective proof of a foreign body of the esophagus or
stomach is obtained by X-ray or endoscopy.
Treatment: Foreign bodies of the esophagus and stomach are removed by
endoscopy. If unsuccessful attempts endoscopic removal of foreign bodies are
removed surgically.
Chemical burns to the esophagus
Corrosives (acid and alkali) cause severe burns to the esophagus. Frequent
suicide attempts among adults and accidents in children, associated with the intake
of vinegar, alkalis or detergents (eg, bleach). The most dangerous strong alkali
used in the home. Less damaging effect have detergents, bleaches and
disinfectants, some medications. Acids cause more damage in the stomach than in
the esophagus. Early appearance burns mouth (or lack thereof), and does not
reflect the extent of dysphagia damaging esophagus. Assessment of damage
requires urgent endoscopy. In the treatment of burns of the esophagus should
immediately appoint corticosteroids and broad spectrum antibiotics. Survivors may
develop strictures and esophageal carcinoma in long-term periods.
Pathogenesis. Acids cause coagulation necrosis of tissue-way vaniem dense
crust that prevents the penetration of substances and reduces the depth of its
penetration into the blood. Alkalis cause necrosis, which contributes to the transfer
and dissemination of alkali in the healthy parts. Alkali burns are characterized by a
deep and widespread lesions of the esophageal wall. Ingesting a substance other
than the local, and has a general toxic effect to the development of multiple organ
failure. There are 4 stages of pathological changes: hyperemia and mucosal edema,
necrosis and ulceration of the mucous membranes, the formation of granulation
tissue, scarring. The degree of morphological changes depending on the
concentration of caustic substance, its quantity, the degree of filling of the
stomach, the timing of first aid, the nature of the received material.
Clinically, there are three degrees of burns of the esophagus:
I - hyperemia and mucosal edema
II - mucosal lesion and submucosa
III - Defeat all the shells of the esophagus
Clinic:
The acute stage (5-10 days): Pain in the mouth, throat, chest, epigastric.
Hypersalivation. Dysphagia. The shock in the next few hours after the injury. Burn
toxemia in a few hours begins to prevail.
Stage imaginary prosperity (7-30 days): as a result of rejection necrotic
esophageal tissue from around the end of the 1st week is somewhat looser.
Complications: esophageal bleeding, perforation of the wall of the esophagus, in
the presence of extensive wound surfaces develops sepsis.
Stage of stricture formation (from 2 to 6 months, sometimes for years). On the
wall of the esophagus varying length sites. Wound surface covered with a scab,
bleed easily. Dysphagia can reach the degree of complete obstruction of the
esophagus. When higher strictures: laryngospasm, cough, dyspnea due to spillage
of food into the airways.
Treatment of burns:
1. Rinse mouth and stomach solutions antidotes.
2. Drinking plenty of fluids (water, milk), followed by vomiting.
3. Required early (the first time) Gastric lavage (liquid volume of age - from 1
to 5 l).
4. Intensive antishock therapy.
5. Sedatives (pipolfenum, suprastin).
6. detoxification therapy.
7. With the development of acute renal failure - methods extracorporal blood
purification (up to hemodialysis).
8. Infusion therapy under the control of diuresis (indication - forced diuresis),
antibiotic therapy.
9. corticosteroid therapy.
10. Drinking fish oil, vegetable oil.
11. In case of burns of 2-3 degrees early (7-8 days), respectively bougienage
of esophageal lumen.
Treatment of complications. Early probing of the esophagus during 1-1.5
months in combination with corticosteroids and Lydasum. At the stage of
formation of strictures the main method of treatment - probing.
Indications: bougienage is shown all patients with post-burn esophageal
strictures (if it is possible to navigate through the restriction of the metal
conductor). Contraindications: mediastinitis, bronchoesophageal fistula.
Types bougienage:
1. "Blind" - through the mouth.
2. On hollow radiopaque metal wire-nick (most often).
3. Under the supervision of esophagoscopy. It is shown when there is of
making it difficult, during the conductor.
4. According to the principle "probing without end" (with gastrostomy in
patients with tortuous and multiple strictures).
5. Retrograde (gastrostomy).
Indications for surgery:
1. Complete obliteration of the lumen of the esophagus.
2. Repeated failed attempts of the bougie passed through the stricture.
3. Recurrence of stricture after bougienage.
4. esophageal-tracheal, esophageal-bronchial fistula.
5. The perforation of the esophagus during probing.
6. More than two years after the burn.
The types of operations:
1. In segmental strictures - partial esophagoplasty.
2. With extensive strictures - total esophagoplasty with anterosternal or
intrasternal location transplant from the small or large intestine.
Esophageal dysmotility
Esophageal achalasia. Achalasia of the esophagus, also called achalasia;
cardiospasm; megaesophagus. Achalasia (cardiospasm) neuromuscular diseases of
the esophagus, violation of passage of food masses in the stomach due to persistent
violations of reflex opening of the cardia in swallowing, changes in motility and
tone of the esophageal wall attenuation. The incidence in relation to other diseases
of the esophagus from 3 to 20%. The first symptoms often occur at the age of 20 to
40 years. More common in women.
Etiology and pathogenesis: etiological factors achalasia - congenital
malformations of the nervous apparatus of the esophagus (intermuscular
degeneration (S. auerbachii) plexus); with the emergence of constitutional
neurasthenia, neurogenic discoordination of esophageal motility; reflex
dysfunction of the esophagus; infectious and toxic lesions of nerve plexus
schischevoda and cardia. Authorizes factor is stress or prolonged emotional stress.
Pathogenesis: the study of intraesophageal pressure in the esophageal-gastric
junction is detected sphincter (physiological cardia). In healthy people, it alone is
able tonic contraction and relaxes after swallowing. The main violation defining
symptoms is the lack of or insufficient relaxation of the cardia relaxation after
swallowing. A variety of reactions cardia (incomplete disclosure when swallowing,
and incomplete disclosure spasm, full achalasia, achalasia and spasm,
hypertonicity source, etc.) Are one source mechanism of violation of the
innervation of the esophageal wall. Cases of achalasia occurring with cardiac
sphincter hypertonicity, can not be regarded as a true "cardiospasm" as the primary
mechanism for violating the permeability of the cardia is not hypertonicity
sphincter relaxation and the absence of his swallowing. Increased pressure in the
physiological cardia here is secondary and due to its reaction to the constant
pressure of the filling content esophagus, scarring and inflammatory changes in the
tissue-foot terminal esophagus and the loss of elasticity.
If achalasia simultaneously change the tone and peristalsis of the esophagus.
Instead of spreading to the stomach peristaltic contractions appear nepropulsivnye
(not ensure passage) waves, they are joined by segmental contraction of the
esophageal wall. Food is long delayed in the esophagus and into the stomach as a
result of the mechanical opening of the cardia under the influence of the
hydrostatic pressure of the liquid column above it. Prolonged stagnation food
masses, saliva and mucus in the esophagus leading to a significant expansion of its
lumen, and the development of esophagitis periesophagitis, which in turn
aggravates motility disorders of the esophagus.
Pathological Anatomy: in severe cases note the expansion in diameter of the
esophagus 15 to 18 cm, its elongation, whereupon he can take an S-shape. Its
capacity reaches 2.3 liters instead of 50-100 ml in healthy people. The distal
portion of the esophagus narrowed sharply, it detected dystrophy ganglion cells
and fibers intramural nerve plexus until their death. The muscle layer was observed
degeneration of muscle fibers, the proliferation of connective tissue, particularly in
the wall narrowed segment fibrosis endoneurium, vasodilation, the appearance
around the infiltration of lymphoid and plasma cells. In all layers of the esophageal
wall and surrounding tissues show signs of inflammation. Esophageal mucosa
hyperemic, edematous, sometimes ulcerated. More pronounced changes in the
vicinity of the narrowed area of the esophagus.
Clinic and diagnostics: for achalasia is characterized by a triad of symptoms:
dysphagia, regurgitation, pain. Dysphagia - basic and, in most cases the first
symptom of the disease. In some patients it occurs suddenly, as though among full
health, while others develop gradually. Strengthening of dysphagia in most patients
say after a nervous excitement, during a hasty meal, while taking a dense, dry and
poorly chewed food. Sometimes there is a paradoxical dysphagia: dense food
passes into the stomach is better than the liquid and semi-liquid. A number of
patients with achalasia, dysphagia depends on the temperature of food: bad passes
or does not pass the food warm and cold pass, or vice versa. Patients gradually
adapted to facilitate the passage of food into the stomach through a number of
techniques (walking, gymnastics, swallowing air and saliva, drinking large
amounts of warm water, and others.). Expressed cachexia when achalasia are rare.
Regurgitation with a small expansion of the esophagus occurs after a few
mouthfuls of food, with a significant expansion of the esophagus is a rare, but
abundant and caused severe spastic contractions of the esophagus that occur when
it is full. Regurgitation in the supine position and with a strong torso caused by
mechanical pressure on the contents of the esophagus sphincter
pharyngoesophageal and stretching.
Night regurgitation associated with some decrease in tone
pharyngoesophageal sphincter. Chest pain when achalasia have varied. They may
be associated with spasm of the esophageal muscles and eliminated taking
nitroglycerin, amyl nitrite, and atropine. However, the majority of patients pain
occur overflow esophagus and disappear after regurgitation or passage of food into
the stomach. In some patients, there are attacks of spontaneous pain in the chest on
the type of pain crises. Such pain is more often observed in the initial period of the
disease, sometimes before the onset of dysphagia and regurgitation, which can not
always be removed by atropine or nitroglycerin, which suggests their association
with progressive dystrophic process in the intramural plexus of the esophagus. Pain
on an empty stomach or after vomiting often caused by esophagitis and removed
meal. Belching air, nausea, excessive salivation, burning along the esophagus, bad
breath and are conditioned esophagitis. In patients with both acute and gradual
onset symptoms progress over time: enhanced dysphagia, regurgitation often
occurs. Many patients are embarrassed of their lack, become withdrawn, painfully
touchy.
The most common complication of the disease is stagnant esophagitis, which
occurs when a long delay food masses in the esophagus. In mild cases, it appears
hyperemia and edema of the mucosa, more severe - presence of coarse and uneven
folds, erosions, ulcers, which are usually located slightly above the narrowed area.
In the future may develop bleeding, perforation of the esophagus, periezofagit.
Chronic esophagitis can cause cancer of the esophagus and cardia. Complications
of achalasia are often repeated aspiration pneumonia, lung abscess, pulmonary
fibrosis. Most often, they occur in children. We describe the complications caused
by compression of the esophagus advanced recurrent nerve, the right main
bronchus, superior vena cava, the vagus nerve, and others.
B.V. Peterovskiy identifies four stages of the disease:
Stage I - functional intermittent spasm of the cardia, the expansion of the
esophagus is not observed;
Stage II - stable spasm of the cardia with soft extension of the esophagus,
Stage III - scarring of muscle layers of the cardia with a pronounced
expansion of the esophagus,
Stage IV pronounced stenosis of the cardia with dilation of the esophagus,
often S-shaped with esophagitis.
The main methods of diagnosis of achalasia are rentgenologic study,
esophagoscopy, esophagotonokimography, pharmacological tests.
At chest X-ray in patients with achalasia identify additional bulging of the
right contour of the mediastinum, the liquid level in the projection of the posterior
mediastinum, the absence of a gas bubble stomach. The main radiological signs of
achalasia - narrowing of the terminal part of the esophagus with a clear, smooth
and elastic loops ("inverted flame candle", "mouse tail") folds of the mucous
membrane in the area of narrowing saved. The first sip of barium can freely flow
into the stomach and then the contrast mass lingers long in the esophagus. Over
barium suspension define a layer of liquid and food debris. Expansion of the
esophagus above the constriction it is expressed to different degrees. A number of
patients note elongation and curvature of the esophagus.
Peristalsis of the esophagus in all patients dramatically impaired: the
reduction eased to have spastic character and lack of amplitude. With the
development of esophagitis seen changes in the relief of the mucous membrane of
the esophagus: grain, thickening and tortuosity of the folds.
Esophagoscopy allows you to confirm the diagnosis of achalasia, identify its
complications and to conduct a differential diagnosis with other diseases associated
with dysphagia. Endoscopic picture depends on the duration of the disease. At the
beginning of the disease esophagus expanded slightly, as the disease progresses the
lumen increasingly expanding and some patients become crimped.
The mucosa shows signs of inflammation: fold thickened arteries and veins
dilated, often visible areas of hyperemia, erosion, leukoplakia, ulcerations. Usually,
the end of esophagoscopy manages to push through the narrowed area, confirming
mainly the functional nature of the changes in the esophagus. The mucosa in the
constriction is not changed often.
Esophagotonokimographic study - the main method for early diagnosis of
achalasia of the esophagus, as a violation of the contractile ability of the esophagus
and cardia physiological occur much earlier than the clinical symptoms of the
disease. The study was conducted by a special multi-channel probe with rubber
bulb, or "open" catheters, registering reductions and changes within the esophagus,
esophageal pressure.
Normally, after swallowing the esophagus extends peristaltic wave, card at
this moment is opened and the pressure is reduced. After passing through the
peristaltic wave cardia is closed again. If there is no reflex achalasia cardia
sphincter relaxation during swallowing, and intraluminal pressure remains on the
former numbers. Another characteristic feature is the motility disorders of the
esophagus: swallowing of various shapes and spastic contraction, a large number
of local - secondary contractions of the esophagus, which indicates esophagitis. In
all patients, along with spastic contractions noted a large number of propulsive
peristaltic contractions of the esophagus. In doubtful cases, to confirm the
diagnosis of achalasia using pharmacological tests. Nitroglycerin, amyl nitrite in
patients with achalasia of the esophagus and lower the tone of the physiological
cardiac sphincter, which facilitates the passage of the contents of the esophagus to
the stomach. Introduction cholinotropic drugs (acetylcholine, carbachol, Meholah)
stimulates the muscular layer of the esophageal wall and the cardiac sphincter. At
cardioesophageal cancer and organic stenosis of the esophagus both samples are
negative.
Treatment: conservative therapy for achalasia is used only in the initial stages
of the disease, as well as used as a supplement to cardiodiosis and in preparing
patients for surgery. Food should be mechanically and thermally gentle, rich in
protein, vitamins. Power fractional, the last meal 3-4 hours before bedtime.
Reduction of dysphagia in I-II stages of the disease can be achieved by the use of
drugs nitro - nitroglycerin, amyl nitrite. With symptoms of congestive esophagitis
use a weak solution of washing esophagus antiseptics. The therapeutic effect was
observed after physical therapy electrophoresis (iontophoresis) with novocaine,
deep diathermy in the region of the cardia, the long-wave diathermy, etc.
The main treatment for achalasia - cardiodiosis which is forced tension and
partial laceration of muscles of the distal portion of the esophagus and cardia.
Cardiodiosis may be carried out at any stage. Contraindication to its use are: portal
hypertension with esophageal varices, expressed esophagitis, blood diseases,
accompanied by bleeding disorders.
The most widely currently received pneumatic cardiodilatator which includes
radiopaque rubber tube probe at the end of which is fixed a dumbbell shaped
balloon. The diameter of the cylinder 25 to 45 mm. The pressure in the system
creates a pear and control gauge. At the beginning of treatment used extenders
smaller and establish pressure of 180-200 mm Hg, then use a larger diameter
cylinders and gradually increase them to pressure 300-320 mmHg. Duration of
treatment stretching cardia 30-60, the gap between sessions 2-4 days. Usually
during stretching patients experience mild chest pain in the epigastric region. After
the procedure, patients prescribed bed rest and hunger for 2-3 hours until the
disappearance of pain.
The effectiveness of dilatation is judged not only by the subjective feelings of
the patient, but also according to X-ray and esophagotonokimographic research.
During cardiodiosis in the next few hours after the possible complications (rupture
of the esophagus with the development of mediastinitis, acute esophageal-gastric
bleeding), requiring urgent action.
The early complications include dilation and insufficiency of the cardia with
the development of severe reflux esophagitis. As soon as possible after
cardiodiosis excellent and good results say nearly 95% of the patients, but after a
few years in 30-70% of patients with a recurrence requiring repeat treatment.
Surgical treatment of achalasia is symptomatic and aims to eliminate obstruction of
the gastroesophageal junction.
The indications for it are:
1. inability to hold cardiodiosis,
2. The lack of therapeutic effect after repeated courses cardiodiosis,
3. The early diagnosis of esophageal ruptures occurring during the expansion
of the cardia,
4. expressed peptic stricture developed after distension of the cardia and not
amenable to conservative therapy and probing,
5. The dramatic expansion, S-shaped curvature of the esophagus combined
with scar changes in the cardia.
Undergo surgery 15-20% of patients with achalasia. Currently, of all proposed
operations are used only by those that are based on the idea cardiomyotomy.
Extramucosal cardioplastic by Geller made of abdominal access, producing a
longitudinal incision muscle membrane terminal esophagus on the front and back
walls for 8-10 cm. The operation combined with Geller’s esophagofundoraphia or
Nissen fundoplication for the prevention of peptic esophagitis. The results of
operations for achalasia depends on the degree of preoperative esophageal changes
(change of tone and motility, severity of inflammation), as well as carefully
executed plastic surgery.
The ratio of the frequency of cardiodiosis and cardiomyotomy is 3: 1, but may
change as a result of the widespread introduction of advanced techniques of
performance of these procedures - endoscopic and laparoscopic myotomy
cardiodiosis devoid of drawbacks of open surgery.
Esophagism
Esophagism (diffuse) - a disease of the esophagus caused by spastic
contractions of its walls during normal function of the cardia. Most often occurs in
men and mostly in middle-aged and elderly. 6% of all functional disorders of the
esophagus.
The etiology of a number of patients due to esophageal spasm viscero-visceral
reflexes, and combined with other diseases (peptic ulcer disease, tumors of the
esophagus and stomach, cholecystitis, peptic esophagitis, hiatal hernia,
atherosclerosis, angina, etc.). Because of this he was called reflex (secondary)
esophageal spasm.
There are also idiopathic (primary) esophageal spasm, are caused by
dysfunction of the nervous system and innervation of the esophagus. Pathological
anatomy: macroscopic changes in the esophagus is missing or there are signs of
esophagitis, sometimes noted muscle membrane thickening of esophageal wall.
Microscopic examination revealed significant degenerative changes in the
branches of the vagus nerve innervating the esophagus. The nature of the nerve
trunks and plexuses of the esophagus when esophagospasm achalasia and different,
which confirms the independence of these diseases.
Clinic and diagnosis: clinical picture is dominated by pain behind the
breastbone that appear during the passage of food through the esophagus, have
different intensities, may radiate to the back, jaw, neck, arms and other. Sometimes
there is pain meal, then they can be difficult differentiate from pain caused by
angina. For esophageal spasm characterized by impermanence dysphagia and often
its paradoxical character, which allows to differentiate this disease from cancer,
esophageal stricture and achalasia, where the worst passes dense food and water it
brings relief. During severe spastic contractions of the esophagus can be a
regurgitation of small amounts of the newly ingested food into his mouth. It is
never abundant, eaten a few hours before regurgitation or the day before.
X-rays reveal changes in the esophagus as a "rosary", "pseudodiverticulum",
"corkscrew". The diameter of the esophagus above and below the narrowed area is
not changed, the esophageal wall resilient longitudinal mucosal folds, uneven and
irregular peristalsis. Repeated radiographic studies usually stored one and the same
type of motility disorders.
Esophagoscopy with this disease and little information is only relevant to
exclude organic diseases of the esophagus, it is often difficult because of the strong
chest pain occurring during the study. Esophageal mucosa is not changed or there
are signs of inflammation.
Eszophagotonokimographic study reveals spastic contraction of the esophagus
in the form of waves of different shape and amplitude, both recorded and
peristaltic contractions. Constantly determined reflex relaxation of the cardiac
sphincter (cardia disclosure). Pharmacological test with acetylcholine and
carbachol negative. Patients with esophageal spasm often find hiatal hernia,
perhaps a combination of disease with esophageal diverticulum.
Complication of esophageal spasm is esophagitis, reflex angina attacks. Longterm course of the disease, dysphagia times it intensified, then disappear almost
completely. In secondary (reflex) dyskinesia esophageal its symptoms usually
disappear when curing the underlying disease. Ability to work, as a rule, are not
compromised.
Treatment: it should be directed to the normalization of esophageal motility.
Complex treatment of patients with idiopathic (primary) esophagism include the
appointment of a sparing diet, antispasmodic and sedative medications, vitamins,
physiotherapy. In the absence of a positive effect from conservative therapy
produces esophagomyotomy (similar to operation Geller) to the level of the aortic
arch.
Lack of cardia (chalasia)
The disease is associated with impaired closing function physiologists-cal
cardiac sphincter, which can lead to gastro-esophageal reflux disease, and the
development of functional and organic changes in the esophagus. The lower
esophageal sphincter has a "one-sided cross." To move the contents of the
esophagus through a card is sufficient pressure of 4 mm Hg. v. in the opposite
direction movement is possible only when the pressure to 80 mm Hg. Art.
Normally, the pressure in the physiological cardia higher than the bottom of the
esophagus and stomach, and is equal to an average of 22-28 mm Hg. Art. It is
caused by tonic contraction of circular muscle fibers, preventing gastro-esophageal
reflux.
Most importantly, the subdiaphragmatic portion of the physiological cardia,
which prevents reflux with significant differential pressure in the chest and
abdomen. Normal anatomical location of the esophagus with respect to the
diaphragm is very important for the proper functioning of the locking mechanism
of the physiological cardia. Ingress of gastric contents into the esophagus and
prevent the presence of "mucous outlet" in the gastroesophageal junction, acute
angle-branch block, the valve of Gubarev - mucosal folds at the junction of the
esophagus with the stomach, the reflex reflex cardia when subcardial irritation of
the stomach with food and . The most frequently (50% of patients) incompetence
of cardia, leading to reflux esophagitis and peptic ulcer of the esophagus observed
in hiatal hernia.
Gastroesophageal reflux disease
Under gastroesophageal reflux disease (GERD) refers to cases of pathological
casting stomach contents into the esophagus regardless arise with morphological
changes in the esophagus or not. The majority of patients from repeated casting
esophageal mucosa inflamed, developing reflux esophagitis (RE). GERD - the
most common gastroenterological diseases. ER frequency in the population is
about 2-4%. Endoscopic examination of the upper gastrointestinal disease is found
in 6-12% of cases, most often in patients older than 50 years.
The classification of reflux esophagitis (RE):
I. Primary
Primary disorders of the nervous and peptide (gastrin, histamine, motilin, and
others.) Regulation of motility of the esophagus and stomach.
II. Secondary
At hiatal hernia, pyloric stenosis, cholecystitis, large tumors in the abdomen
ascites, pregnancy after gastric resection, in scleroderma and other diseases.
III. By severity (endoscopic classification of Savary and Miller, 1978)
Stage 1 - redness and swelling of the mucous membrane of the distal
esophagus, erosion of the sensible.
Stage 2 - drain erosion, captures up to 50% of the mucosal surface of the
distal esophagus
Stage 3 - erosion and / or ulceration in almost all (50%) or the whole surface
of the mucosa of the distal esophagus
4th stage - deep ulcers, esophageal stenosis, the cylindrical epithelium of the
mucous metaplasia, its distal (Barrett's esophagitis).
Syndrome of Berret esophagitis - cylindrical metaplasia (replacement of
stratified squamous epithelium) of the distal esophageal mucosa. It is considered a
precancerous condition of the esophagus. GERD refers to diseases with a primary
violation of esophageal motility and stomach. It helps to reduce the appearance of
the tone of the lower esophageal sphincter (LES), which is revealed in almost 3/4
of patients (normal, he has thrown into the esophagus prevents gastric contents).
Reduced LES tone may be due to a breach of its nervous regulation of smooth
muscle fibers and defeat. Reduce or increase LES tone may bioactive substances
and peptides.
Pathogenic factors of GERD - increase intragastric pressure, weakening the
ability of the esophagus to the stomach return hit him the contents, slowing gastric
emptying, increased production of hydrochloric acid, weakening the protective
properties of the epithelium of the esophagus and others.
Some importance in recent years began to attach the esophagus colonization
particular microorganism - Helicobacter (Helicobacter pylori), which worsens
during GERD. Contribute to the emergence of GERD. In addition, working
posture, forcing to the torso, overweight, pregnancy, smoking and alcohol
consumption, medication (calcium channel blockers, anticholinergics,
theophylline, beta-blockers), frequent consumption of chocolate, coffee, some fruit
juices, pepper and other spices.
Symptoms of GERD - heartburn and epigastric pain, or in the lower part of
the sternum, arising during a meal or immediately after it, belching air,
regurgitation. In 25-40% of patients have dysphagia, which often indicates a
connection of peptic stricture of the esophagus, but can be simply a manifestation
associated dyskinetic disorders.
By extraesophageal manifestations of GERD and OM refers getting
esophageal contents into the bronchi with the emergence of bronchospastic
syndrome. GERD may also lead to the development of recurrent aspiration
pneumonia and bronchitis, laryngitis, pharyngitis, destruction of tooth enamel.
Tactics of treatment. The treatment starts with a general events, referred to as
a lifestyle change. We recommend frequent and smaller meals, eating at least 3
hours before bedtime, the vertical position of the body after eating, with the
exception of coffee, chocolate, pepper, spicy food, alcohol, smoking cessation
medication, drugs, predisposing to gastroesophageal reflux disease (nitrates, Mcholinoblocers, antidepressants, sedatives, aminophylline), abstaining from
physical exercise associated with torso. Patients also are advised to 15-20 cm to lift
the head end of the bed.
Assign an antacid (Maalox, and others) that increase gastric pH, increase the
tone of the LES, reduce the amount of reflux quickly cropped pain and heartburn.
However, the use of antacids together with common actions makes only 20% of
patients with GERD.
An important place in the treatment given to drugs, normalizing
gastrointestinal motility (prokinetic). Widely used dopamine receptor blockers metoclopramide and domperidone. It should be borne in mind that drugs of metoclopramid, providing central action, capable of causing extrapyramidal disorders,
especially in children and the elderly. Such patients are not recommended to
assign.
Cisapride (koordinaks) does not affect the dopaminergic receptors. It
stimulates the release of acetylcholine in the intermuscular neural plexus digestive
tract by activating serotonin 5HT4 receptors. Increases tone NPC improves
oesophageal clearance, normalizes gastric emptying. In the treatment of GERD
sufferers cisapride highly effective at a daily dose of 30-40 mg. Usefulness potent
antisecretory agents (histamine H2 receptor blockers and proton pump) is
supported by data, according to which erosion of the esophageal mucosa majority
of patients heal only when during the day manages to maintain the pH in the
esophagus over 4. At the same dose of histamine H2 receptor 2 times higher (600
mg or ranitidine 80 mg famotidine per day). Proton pump blockers are currently
considered the most potent antisecretory drugs. Omeprazole 40mg achieves
esophageal erosions heal in 85-90% of patients, including patients who do not
respond to therapy with histamine H2 receptor blockers.
If necessary, long-term maintenance receiving proton pump blockers
(omeprazole, lansoprazole, pantoprazole) is required to conduct a course of
eradication antibiotic therapy in case of pyloric helicobacter in gastric mucosa.
Such treatment can prevent the progression of atrophic gastritis in a long-term use
of proton pump blockers. In repeated gastrointestinal bleeding of peptic esophageal
strictures, Barrett's syndrome formation, combined with dysplasia of the
esophagus, as well as the ineffectiveness of conservative therapy surgical
treatment. Perform the Nissen fundoplication.
Operation is enveloping the abdominal wall esophagus fundus. The stomach is
fixed to the diaphragm around the esophageal opening multiple seams. Good
results were achieved in more than 90% operated.
Diverticula of the esophagus
Diverticulum of the esophagus - esophageal diverticulum limited wall. There
are pulsion and traction diverticula. Pulsion diverticula are formed as a result of
esophageal diverticulum wall under high pressure intraesophageal arising during
its contraction. Development factional diverticula associated with inflammation in
the surrounding tissues, and scarring, which pulled the wall of the esophagus
toward the affected organ (mediastinal lymphadenitis, chronic mediastinitis,
pleurisy).
Traction mechanism is observed in the early development of a diverticulum,
then join pulsion factors, resulting in a diverticulum becomes pulsion-traction. The
diverticula are divided depending on the location on pharyngoesophageal
(Zenker's) epibronchiale (bifurcation, esophageal) epiphrenal (epidiaphragmal).
There are true diverticula, the wall of which contains all the layers of the wall
of the esophagus, and are solely responsible, in the wall of which there is no
muscle layer. The vast majority of acquired diverticula, congenital diverticula are
rare. When motility disorders of the esophagus (esophageal spasm) observed
pseudodiverticulum arising only at esophageal reduction, relaxation of the
esophagus when they disappear. The diverticula are rare under the age of 30 years
and often after 50 years; among patients with male-dominated. Most diverticula are
often in the thoracic esophagus.
Pathological anatomy: pharyngoesophageal (Zenker's) diverticula develop
slowly formed in the back of the throat, just above the entrance into the esophagus,
often in the Lanier- Gakkerman triangle where muscular coat of the pharynx shows
weak muscle bundles inferior pharyngeal constrictor muscle, at least - in the
Laymer triangle bounded above m.cricopharyngeus, and on the sides - the
longitudinal muscle fibers esophageal wall.
The main importance in the formation of a Zenker's diverticula achalasia
cricopharyngeal muscles (violation of the disclosure of the upper esophageal
sphincter in response to swallowing). Diverticula go down between the rear wall of
the esophagus and the spine, can be displaced by the side of the neck muscles.
Their magnitude is different, they have a wide mouth. Diverticular wall contains
muscle fibers are generally not adherent to the surrounding tissues, its inner surface
is covered with a mucous membrane of the pharynx, it may be on the surface of
erosion or scarring.
Most epibronchial diverticula are located on the front or left side wall of the
esophagus, they rarely exceed a diameter of 1-2 cm. The bottom of the
diverticulum is usually directed upwards and adherent to adjacent organs, the wall
has a structure of the esophageal wall. Cavity diverticulum widely reported with
the esophageal lumen. When diverticulitis its shell inflamed mucosa may be
eroded. Epiphrenal diverticula most patients are placed on the front or the right
side wall of the esophagus, have rounded or slightly elongated shape. Their
diameter is larger than epibronchial diverticula in the neck there is often a slight
taper. Even with the larger sizes in the diverticula are rarely observed delay and the
expansion of the food mass. The wall has a structure of the wall of the esophagus,
the muscular shell can be poorly expressed or absent. The mucosa in most patients
is not changed. Finger diverticula with neighboring authorities are not usually
marked.
Clinic and diagnostics: small pharyngoesophageal diverticulum manifested
feeling tickling, scratching throat, dry cough, foreign body sensation in the throat,
excessive salivation, sometimes spastic dysphagia. As the diverticulum filling it
with food may be accompanied by a gurgling noise when swallowing, lead to the
development of dysphagia varying degrees of severity, to the appearance of
protrusions on the neck during abduction of the head backwards. Flexing has a soft
consistency, decreases with pressure, after taking water on percussion over it is
possible to determine splashing. Possible spontaneous regurgitation of undigested
food from the lumen of the diverticulum at a certain position of the patient,
difficulty breathing due to compression of the trachea, the occurrence of
hoarseness in the compression of the recurrent laryngeal nerve. When eating in
patients may develop "a phenomenon of the blockade", which appears red face,
feeling short of breath, dizziness, fainting, disappearing after vomiting during long
delays in food diverticulum appears putrid breath. Most patients with disturbed
nutrition that causes them to depletion.
Epibronchial diverticula often characterizes asymptomatic possible effects of
dysphagia, pain in the chest or back. In chronic diverticulitis - a breakthrough in
the trachea, aspiration, developing pneumonia, lung abscess.
Epiphrenal diverticula as most patients are asymptomatic, but may manifest
pain behind the lower part of the sternum, aerophagia, nausea, vomiting, shortness
of breath reflex, heartbeat, bronchospasm symptoms of compression of the
esophagus and cardiospasm. The disease is slow, with no significant progression.
Zenker's diverticulum may be complicated by the development of
diverticulitis, which in turn can cause cellulitis neck, mediastinitis, development of
esophageal fistula, sepsis. Regurgitation and aspiration of content diverticulum
lead to chronic bronchitis, repeated pneumonia, lung abscess. There may be
bleeding from eroded mucosa diverticulum, polyps develop in it, its walls
malignancy.
If a long delay in mass food epibronchial and epiphrenal diverticula can occur
complications of diverticulitis, mediastinal abscess with a breakthrough in the
bronchus, esophagus, pericardium, and other organs of the mediastinum, massive
bleeding Chronic diverticulitis predisposes to cancer. Pharyngoesophageal
diverticula can sometimes be detected by inspection and palpation of the neck.
The main method of diagnosis of esophageal diverticula is a contrast X-ray
examination, to establish the existence of a diverticulum, neck width, the length of
the delay in its barium, the degree of cross-esophageal diverticulum signs of
development in the polyp and cancer, the formation of esophageal-bronchial
fistulas and esophageal -mediastinal. Endoscopy allows you to establish the
presence of diverticula, discover ulceration of its mucous membranes, bleeding,
diagnose polyps or cancer in the diverticulum. Conduct research to be very careful
because of the possibility of perforation of a diverticulum.
Treatment at small sizes diverticula, without complications, absolute
contraindications to surgery should be conservative therapy to prevent delays in the
diverticulum food masses and reducing the possibility of diverticulitis. Food
should be a full, mechanically, chemically and thermally gentle. Patients
recommend eating good food chopped. After the meal, you should drink a few sips
of water, take the position that promotes emptying diverticulum. For large amounts
of diverticula sometimes necessary washing cavity diverticulum.
Indications for surgical treatment of esophageal diverticula: complications
(perforation, penetration, bleeding, stenosis, esophageal cancer, the development of
fistulas), large diverticula complicated with at least a short-term delay in their food
of the masses, the long delay in the diverticulum of food, regardless of its size.
Depending on the location of the diverticulum choose surgical approach: the
pharyngoesophageal - cervical, when epibronchial - sided transthoracic at
epiphrenal - left-sided transthoracic. Apply diverticulectomy: isolated from the
surrounding tissues diverticulum neck to produce myotomy, dissected it and
sutured hole in the wall of the esophagus. With a significant muscle defect or
atrophy of the muscle fibers of the esophagus produce plastic restoration of its wall
flap of the diaphragm, the pleura. Intussusception is used only at small sizes
diverticula. The mortality rate after surgery is 1-1.5%.
Benign tumors and cysts of the esophagus
Benign tumors of the esophagus are rare. Pathological anatomy: the tumor in
relation to the wall of the esophagus may be intraluminal (polypoid), and
intramural (intramural). On histological structure of the tumor is divided into
epithelial (adenomatous polyps, papillomas) and non-epithelial (leiomyoma,
rhabdomyomas, fibroma, lipoma, hemangioma, neuromas, chondroma, myxoma,
etc..). Intraluminal tumor usually located in the proximal or distal esophageal
intramural - in the lower two-thirds of it. From intramural benign tumors of the
esophagus is the most common type of uterine leiomyoma, develops from smooth
muscle fibers.
Clinic and diagnosis: benign esophageal tumors grow slowly for a long time
do not cause clinical symptoms and are discovered by chance during X-ray
examination of the gastrointestinal tract.
Clinical manifestations of them depend on the level of localization, the
magnitude, and complications (ulceration, inflammation, pressure on adjacent.
Bodies). The most common symptom - a periodic, slowly increasing over the
years, dysphagia. Most often it is observed in intraluminal large tumors on the long
leg. When intramural tumors circularly handling esophagus, dysphagia may be
permanent, sometimes patients report pain, feeling of pressure in the chest or
overflow, dyspeptic symptoms. When tumors of the cervical esophagus, with long
stem, regurgitation may occur tumor development and asphyxia. If a polyp or
ulceration of esophageal mucosa damage, stretched over a large intramural tumor
may bleed. Cysts of the esophagus may fester. Due to the compression of the
tumor of the mediastinum (trachea, bronchi, heart, vagus nerves) may experience
cough, dyspnea, cyanosis, palpitations, pain in the heart, arrhythmias and other
disorders. Perhaps the malignant transformation of benign tumors of the
esophagus.
The diagnosis of a benign tumor of the esophagus is put on the analysis of the
clinical picture of the disease, these X-ray examination and esophagoscopy.
For benign tumors of the esophagus characterized by the following
radiological signs: a clear smooth contours filling defect, which is located on one
of the walls of the esophagus, the preservation of the relief of the mucosa and the
elasticity of the walls of the esophagus in the area of the defect, clear the angle
between the wall of the esophagus and the edge of the tumor (a symptom of "cap").
When cinematic study of benign-education of the esophagus when swallowing
moves upward together with the wall of the esophagus.
To exclude external compression of the esophagus neoplasm originating from
the mediastinum, or abnormally large blood vessel located using
pneumomediastinography and aortography. All patients with benign tumors of the
esophagus shows esophagoscopy to clarify the nature of education, its localization
and extension, the state of the mucous membrane Esophagoscopy reveals
intraluminal tumor, inspect its foundation, ensure no rigidity walls of the
esophagus. Ulceration of the mucous membrane in the intramural benign tumors
and cysts of the esophagus is rare. A biopsy can be performed only if the
destruction of the mucous membrane and intraluminal tumors.
Treatment: benign tumors due to the possibility of bleeding, malignancy,
compression of the surrounding organs, surgical treatment. Tumors of the small
size on a thin stalk can be removed by using special esophagoscope and
electrocoagulation. When intraluminal tumors produce on a broad basis to the site
of excision of the esophageal wall. When intramural tumors and cysts of the
esophagus is almost always manage to produce their enucleation without damaging
the mucosa. Long-term results of operations are good.
Esophageal carcinoma
Esophageal cancer - the most common disease of the body is 80-90% of all
diseases of the esophagus. Among all malignant tumors of the esophagus cancer is
the eighth, and malignant tumors of the digestive tract - 3rd place after cancer of
the stomach and rectum. Most commonly affects the middle third of the thoracic
esophagus (40-60%), at least part of the tumor is localized in the upper thoracic
(10-15%) and lower thoracic (20-25%) departments.
Grossly, there are three forms of cancer:
1. scirrhous or infiltrative cancer, when the tumor infiltrates the wall of the
esophagus uniformly and without distinct border passes in normal tissue;
2. Ulcerative or medullary cancer - growing into the lumen of the esophagus,
easily breaks early metastasizes to regional lymph nodes and distant;
3-knotted or warty papillomatous cancer - has exofit growth, easily breaks and
bleeds; mixed forms of the tumor.
On histological structure it develops in 96% of squamous cell carcinoma,
adenocarcinoma, or much less undifferentiated carcinoma. The incidence - the
occurrence of esophageal cancer associated with the peculiarities of power, as well
as alcohol and tobacco smoking. Among the indigenous peoples of the North,
Siberia and Far East widespread use of very hot "brick" tea, frozen fish and meat,
hard pellets that are sometimes in the winter, too, are stored in frozen form. Such a
diet with irregular nutrition, as well as the abuse of alcohol or lead to permanent
injury to the esophagus and predisposition to cancer. There is a zone of high
incidence of esophageal cancer. It covers northern Iran, Central Asia, Kazakhstan,
Yakutia, some regions of China and Mongolia. In addition to these areas, there is a
very high incidence in several countries in South Africa. Increased incidence of
esophageal cancer in France and Brazil. India and the United States among the
black population. In most European countries, the tumor is relatively rare (men - 4-
7, 1-2 women per 100 000 population). In areas with a high incidence of
esophageal cancer is 5-10 times more common in persons of the indigenous
nationality, than the non-indigenous population. Such significant differences may
be related to the peculiarities of the nature of power, but we can not exclude the
influence of genetic factors. Risk factors for esophageal cancer is recognized
systematic contact with carcinogens, chronic radiation exposure, excessive
mechanical, thermal, chemical irritation of the esophagus cicatricial narrowing of
the esophagus chemical burns after his achalasia, hiatal hernia, reflux esophagitis.
Precancerous diseases: Repeatedly repeated exposure to harmful factors leads
to microtraumas or thermal damage to the esophageal mucosa, causing chronic
esophagitis and support. Chronic esophagitis create conditions for realization of the
toxic effect of carcinogenic substances contained in tobacco smoke and enters the
food composition, often accompanied by epithelial dysplasia of esophagus mucosa.
By precancerous diseases also include peptic ulcer of the esophagus, polyps and
papillomas of the esophagus scar stricture, dysphagia sideropenic (PlummerVinson syndrome).
Diagnosis: "Alarms" suggest the possibility of cancer of the esophagus are:
dysphagia any severity that occurred regardless of mechanical, thermal or chemical
injury of the esophagus; sense passage bolus, pain or discomfort along the
esophagus resulting from the ingestion; recurrent regurgitation or vomiting,
especially with blood; unjustly appeared hoarseness; racking cough that occurs
when fluid intake. Instrumental methods of research are crucial in detecting cancer
of the esophagus.
X-ray examination of the esophagus detected: violation of the structure of the
mucous relief; filling defect detection; the shadow of the tumor site; the absence of
esophageal peristalsis. Features X-ray study increase with double-contrast
esophageal study under pneumomediastinum. Esophagoscopy must be performed
at the slightest suspicion of esophageal pathology. This is a direct method of
diagnosis of the tumor. Set the level of destruction, the shape of the tumor, the
degree of narrowing of the esophagus, the presence of decay or bleeding from the
tumor. During esophagoscopy taken material for cytological and histological
examination. The informativeness of these methods is very high.
Staging of esophageal cancer is performed by generally accepted international
classification of esophageal cancer, which provides characterization of the tumor
system TNM.
The clinical picture. The clinical symptoms of esophageal cancer can be
divided into three groups: primary or local symptoms associated lesion esophageal
wall; secondary symptoms resulting from proliferation of tumor to adjacent organs
and tissues; common symptoms caused by intoxication and malnutrition.
The primary symptoms include dysphagia, chest pain, a feeling of fullness in
the chest, regurgitation of food (regurgitation), reinforced salivation. Almost all of
these symptoms indicate a sufficiently large propagation of the pathological
process of the esophagus.
Typical symptoms of cancer of the esophagus caused by the phenomenon of
obstruction. The most striking of these is dysphagia - difficulty in the passage of
food through the esophagus. Dysphagia caused by narrowing of the lumen of the
body of a growing tumor (mechanical dysphagia), but sometimes it depends on the
spasm in the overlying esophagus (dysphagia reflex). In most cases, dysphagia is
growing gradually.
At first it appears barely noticeable delays when passing through the
esophagus solid food. The patient feels as if a lump of solid food on its way
through the esophagus. The narrowing progresses, and soon the patient has to drink
a sip of water solid food or stop taking dishes. Later, after a few weeks or months
stops flowing semi-liquid food, and then the liquid. This consistent development of
dysphagia is not always observed. Sometimes, as a result of the collapse of the
tumor or medical treatment of esophageal patency partially or fully restored.
Improving the condition does not last long, and soon begins to progress again
dysphagia.
There are 5 degrees of dysphagia:
I degree - takes any food, but swallowing solid food experience discomfort
(burning, scratching, sometimes pain);
II degree - solid food lingers in the esophagus and passes with difficulty, it is
necessary to wash down solids with water;
III degree - solid food does not pass. When you try to swallow it appears
regurgitation. Patients fed liquid and semi-liquid food;
IV degree - the esophagus to pass only liquid;
V degree - the complete obstruction of the esophagus. Patients unable to
swallow a sip of water, does not pass even saliva.
Important to diagnose symptoms are: esophageal regurgitation of food and
vomiting. Regurgitation often caused by a spasm, it occurs immediately after a
meal. Esophageal vomiting seen in patients with severe stenosis, some time after
the meal. Regurgitation, along with other dyspepsia (belching, heartburn, nausea)
in some patients may appear the first symptom disease. In some cases, quite early
there salivating (hypersalivation), but more often it occurs at high-grade stenosis.
Hypersalivation treated as a protective reflex that facilitates food to overcome
obstacles.
Along with the listed symptoms esophageal cancer may be accompanied by
unpleasant or smelly breath, which is dependent on tumor lysis and putrefaction
above contraction and felt by the patient or detected by others.
Secondary symptoms are late manifestations of cancer of the esophagus. They
testify about the complications of the disease, due to which the process of the
esophageal wall. Secondary symptoms - a hoarseness, Horner's triad (cramps,
pseudoptosis, endophthalmitis), increase local lymphatic sites, bradycardia, cough,
change of voice sonority, vomiting, shortness of breath, choking with stridor.
Because of the common symptoms inherent malignant neoplasms of internal
organs, cancer of the esophagus observed a progressive loss of body weight, up to
cachexia, increasing general weakness, fatigue, anemia.
Treatment. Treatment options for esophageal cancer depends on the tumor
location, stage of the process, the presence of comorbidities good results of
surgical treatment can be expected in stage I of the disease, at least in the II and III
stages. However, esophageal cancer is rarely diagnosed early, most patients seek
help after six months after the first symptoms of the disease.
Inoperable patients come in for two reasons:
1) tumor sprouting adjacent organs - aorta, trachea, lung, metastasis to lymph
nodes of the second, third order and other organs (liver, lungs); the possibility of
removal of the tumor (resectability) in most patients become completely clear only
during the operation;
2) the presence of concomitant diseases of the heart, lungs, kidneys, liver and
other organs in the stage of decompensation.
In cancer of the cervical and thoracic esophagus tumor grows quickly into the
surrounding organs and early metastasizes. Cancer this localization more
successfully treated using radiation therapy. In cancer of the esophagus produce
middle chest surgery by Dobromyslov-Terek. From transpleural access remove the
thoracic esophagus and impose a gastrostomy. Subsequently (after 3-6 months)
creating an artificial esophagus of the colon or small intestine. In strong young
men can do the resection of the esophagus with anastomosis between the
imposition of the remaining part of the esophagus and the displaced in the right
pleural cavity of the stomach (the operation of Lewis). In cancer of the lower
thoracic esophagus operation of choice is resection of the esophagus with
simultaneous imposition of intrathoracic esophagogastric anastomosis at the aortic
arch, or at the level of her.
Good results from the combination of radiation and surgical treatment.
Preoperative radiotherapy is carried out in dose of 30-50 Gy (3000-5000 rad).
Acting on the primary lesion and possible foci of metastases-tion, radiation therapy
is designed to migrate from a tumor in questionable resectable resectable, to
eliminate accompanying inflammatory changes. Surgery is produced in 2-3 weeks
after the end of radiotherapy.
At unoperative tumor with contraindications to radical surgery produce
palliative intervention to restore patency of the esophagus, improve nutrition of the
patient. Palliative operations include: palliative resection of the tumor
recanalization with Mylar prosthesis (arthroplasty), the imposition of gastrostomy.
Radiation treatment is used as in the radical, and in palliative treatment of cancer
of the esophagus. The most favorable results were obtained using a high energy
source (gamma-therapy, braking radiation and fast electrons) that provide
settlement to the esophageal tumor high-dose radiation.
When squamous cell carcinoma of the upper third of the esophagus after the
imposition of gastrostomy patients underwent radical radiotherapy at a total dose
of 60-70 Gy (6000-7000 rad) at a daily dose of 1.5-2 Gy (150-200 rad). When
squamous cell carcinoma of the middle third of the esophagus patients impose a
gastrostomy tube, and then carry out palliative radiotherapy at a dose of 20-40 Gy
(2000-4000 rad) whose main goal is the removal of dysphagia, pain and slow the
progression of cancer. Treatment provides rapid clinical effect due to the removal
of perifocal inflammation and reduce tumor size. When esophageal
adenocarcinoma radiotherapy is ineffective. Radiation therapy is contraindicated in
severe diseases of the cardiovascular and respiratory systems, parenchymal organs,
central nervous system, the decay of the tumor, bleeding.
If you can not perform surgery or radiation therapy for cancer of the
esophagus can be used as a palliative chemotherapy (a combination of antimetabolites of pyrimidine series - 5-fluorouracil, or methotrexate and fluorofur
colhamini). Chemotherapy is a cancer of the esophagus to the present poor results
due to the low sensitivity of the tumor to the known anticancer drugs.
All patients with an inoperable form of cancer of the esophagus demonstrated
symptomatic therapy aimed at pain relief, elimination of malnutrition. Five-year
survival after radical surgery is less than 10%.
4.2. New pedagogical technologies used on given employment.
«THE BLACK BOX» METHOD USE
The method provides joint activity and active participation in employment of
each student, the teacher works with all group.
Each student gets a question from «a black box». (Variants of questions are
applied.) students should prove the answer in detail.
On considering of each answer 3 minutes are given to the student. Then
answers are discussed, addition on an etiology and a pathogenesis, a clinical
current is given. In the end of a method the teacher makes comments on
correctness of the answer, its validity, a degree of activity of students.
The given technique promotes development of speech of the student,
formation of bases of critical thinking since in this case the student learns to defend
the opinion, to analyze answers of classmates - participants of this competition.
Variants of summaries:
At the patient who has transferred in the past combustion of an esophagus,
has developed disturbance of swallowing of firm nutrition. Such implication
testifies to what pathology.
USE OF THE METHOD "WEB"
Steps:
1. Preliminary time for preparation of questions on the passed employment
is given to students.
2. Participants sit on a circle.
3. The hank of threads is given to one of participants, and it asks the
prepared question (on which it should know the full answer), keeping the end of a
thread and throwing a hank to any student.
4. The student who has received a hank, answers a question (thus the
participant who has set it, makes comments on the answer) and passes on question
baton further. Participants continue to ask questions and to answer them while all
won't appear in a web.
5. As soon as all students will stop to ask questions, the student holding a
hank, returns to its participant from whom has received a question, thus asking the
question etc., before full "unwinding" of a ball.
The note: to Warn students that it is necessary to be attentive to each answer
as they don't know to whom will throw a hank.
4.3. Analytical part
Situational problems:
At the patient who has transferred in the past a combustion of an esophagus, has
developed disturbance of swallowing of firm nutrition.
I. Such implication testifies To what pathology:
a. Esophagus stricture *
b. Duodenum peptic ulcer
c. Stomach peptic ulcer
d. Stenosis pyloric duodenum parts
e. Carcinoma of the stomach
II. What method of research is necessary for spending for diagnosis
specification:
a. Roentgenography with a barium passage *
b. Ultrasonic research
c. Angiography
d. Computer tomography
5. Practical part
Task performance on practical skills (to spend the differential diagnosis and
to prove the definitive diagnosis to prescribe a corresponding diet and planned
treatment).
1. TO SPEND THE DIFFERENTIAL DIAGNOSIS AND TO PROVE THE
DEFINITIVE DIAGNOSIS.
The purpose: to train to spend the differential diagnosis and to prove the
definitive diagnosis.
Action
Completely has
Hasn't
№
correctly
executed
executed
1
To list diseases, clinical symptoms
0
25
which are similar to the given disease
2
To carry out differential diagnostics
0
35
of the basic clinical syndromes
3
On the basis of complaints, the
0
40
anamnesis, the objective data and
results of laboratory-tool researches,
and also differential diagnostics to
expose the definitive diagnosis
Result
0
100
1. TO APPOINT THE CORRESPONDING DIET AND PLANNED
TREATMENT.
The purpose: Treatments of illness and to achieve remission
Action
Completely
Hasn't
№
has correctly
executed
executed
1
Studying of the characteristic of
0
10
medical tables on Pevsner
2
Correct choice of a dietary table
0
10
3
4
5
6
according to the diagnosis
Estimation of full value of a diet
According to the diagnosis, weight of
disease and a stage appointment of
the basic therapy
According to the diagnosis, weight of
disease and a stage appointment of
symptomatic therapy
Preventiveactions
Result
0
0
20
20
0
20
0
0
20
100
6. Forms of control of knowledge, skills and abilities
- The oral;
- The written;
- The decision of situational problems;
- Demonstration of the mastered practical skills.
7. Criteria of an estimation of current control
№ Progress
Estimation
Level of knowledge of the student
in %
1
96-100%
Perfectly
“5”
2
91-95%
Perfectly
“5”
3
86- 90%
Perfectly
“5”
4
81-85%
Well
“4”
The full right answers on questions. Sums up
and makes decisions, creatively thinks,
independently analyzes. Situational problems
solves correctly, with the creative approach, with
a full substantiation of the answer.
Actively, creatively participates in
interactive games, correctly makes well-founded
decisions and sums up, analyzes.
The full right answer on questions.
Creatively thinks, independently analyzes.
Situational problems solves correctly, with the
creative approach, with an answer substantiation.
Actively, creatively participates in
interactive games, correctly makes decisions.
The put questions are shined completely, but
there are 1-2 discrepancies in the answer.
Independently analyzes. Discrepancies at the
decision of situational problems, but at the
correct approach.
Actively participates in interactive games,
makes correct decisions.
The put questions are shined completely, but
there are 2-3 discrepancies, errors. Puts into
practice, understands a question essence, tells
5
76-80%
Well
“4”
6
71-75%
Well
“4”
7
66-70%
Well
“3”
8
61-65%
Well
“3”
9
55-60%
Well
“3”
10
50-54%
Unsatisfactory
“2”
11
46-49%
Unsatisfactory
“2”
12
41-45%
Unsatisfactory
“2”
13
36-40%
14
31-35%
Unsatisfactory
“2”
Unsatisfactory
“2”
confidently, has exact representations.
Situational problems are solved correctly, but an
answer substantiation insufficiently full.
Actively participates in interactive games,
correctly makes decisions.
Correct, but incomplete illumination of a
question. Understands a question essence, tells
confidently, has exact representations. Actively
participates in interactive games. On situational
problems gives incomplete decisions.
Correct, but incomplete illumination of a
question. Understands a question essence, tells
confidently, has exact representations. On
situational problems gives incomplete decisions.
The right answer on half of put questions.
Understands a question essence, tells
confidently, has exact representations only on
theme individual questions. Situational problems
are solved truly, but there is no answer
substantiation.
The right answer on half of put questions.
Tells uncertainly, has exact representations only
on theme individual questions. Commits errors at
the decision of the situational.
The answer with errors on half of put
questions. Tells uncertainly, has partial
representations on a theme. Situational problems
are solved incorrectly.
The right answer on 1/3 put questions.
Situational problems are solved incorrectly at the
wrong approach.
The right answer on 1/4 put questions.
Situational problems are solved incorrectly at the
wrong approach.
Illumination of 1/5 put questions with errors.
Gives incomplete and partially wrong answers to
questions.
Illumination of 1/10 parts of questions at the
incorrect approach.
On questions doesn't give answers.
8. A chronological card of employment.
№ Employment stages
1
2
3
4
5
6
7
Parenthesis of the teacher (theme
substantiation)
Discussion of a theme of practical
employment, estimation of initial knowledge
of students with use of new pedagogical
technologies (small groups, situational
problems, business games, slides, video
films, etc.)
Discussion summarizing
Granting to students of visual aids and a
summer residence of explanatory’s to them
Independent work of students on mastering
of practical skills
Finding-out of degree of achievement of the
purpose of employment on the basis of the
mastered theoretical knowledge both by
results of practical work and taking into
account it an estimation of activity of group
The conclusion of the teacher on the given
employment. An estimation of knowledge of
students on 100 mark system and its
announcement. A summer residence of the
task for following employment (the
complete set of questions)
Employment forms
Duration
in minute
15
Poll, explanation
75
15
30
45
Oral poll, written
poll, tests, check of
results of practical
work, discussion
75
The
information,
questions
for
independent
preparation
15
9. Control questions
1. List kinds of combustions of an esophagus.
2. The reasons of development of a stricture of an esophagus.
3. The reasons of development of an esophagitis.
4. The reasons of development of a diverticulum of an esophagus.
5. Types of a diverticulum of an esophagus
6. Features of treatment of a diverticulum of an esophagus.
10. The recommended literature
I. Basis:
1. Хирургик касаликлар. Ш.И.Каримов, Тошкент, 2005.
2. Хирургические болезни. Ш.И. Каримов, Ташкент, 2005.
3. Chirurgik kasalliklar. Sh.I. Karimov. Toshkent, 2011.
4. Хирургик касаликлар. Ш.И.Каримов, Н.Х.Шамирзаев, Тошкент, 1995.
5. Хирургические болезни. Под ред.М.И.Кузина., Медицина, 2002.
6. Методическое пособие по госпитальной хирургии. Назыров Ф.Г. с
соав.Ташкент 2004г.
7. Клиническая хирургия. Под ред. Панцырева Ю.М. М. «Медицина»,
1988
8. Воробьев А. Справочник практического врача в 3х томах. 1990
9. Конден Р., Нейхус Л. Клиническая хирургия Москва. Практика 1998
10. Назиров Ф.Г., Денисов И.И., Улугбеков Э.Г. Справочникпутеводитель практикующего врача. Москва, 2000.
11. Петровский Б.В. ред. Руководство по хирургии (в 12 томах) М.
Медицина 1959-1966.
II. Additional:
12. Астапенко В.Г. Практическое руководство по хирургическим
болезням. Минск, 2004.
13. Савельев В.С. 50 лекции по хирургии. Москва 2004.
14. Диагностический справочник хирурга – Астафуров В.Н. 2003.
15. Лапароскопическая и торакоскопическая хирургия – Константин
Франтзайдес. 2000.
16. Здравый смысл в неотложной абдоминальной хирургии – Моше
Шайн.2003г
17. Неотложная абдоминальная хирургия – Майстренко Н.А.2002г
18. Абдоминальная хирургия – Григорян Р.А. В 2-х томах.2006г
19. Internet addresses on an employment theme: www.rmj.net,
www.consilium-medicum.com,
www.mediasphera.ru,
www.laparoscopy.ru,
www.ehpb.com,
www.
medmore.ru,
www.gastroportal.ru,
www.medilexicom.com, www.encicloperdia.com, www. omoc.su.