Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
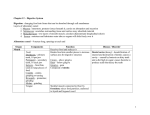
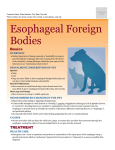
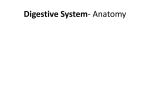
Esophagus Pathology ©2010 Mark Tuttle Achalasia ↓ LES relaxation, ↑LES tone, aperistalsis of the esophagus Atresia Fistula Barrett esophagus Thin, noncanalized cord replaces a segment of esophagus Abnormal cnxn of two epithelium-lined organs or vessels Intestinal metaplasia within the esophageal squamous mucosa. Secondary to GERD Blind outpouching of the GI that is lined by mucosa, communicates with the lumen, and includes all 3 layers of the bowel wall (Lamina propria, submucosa, muscularis externa) Diverticulum above the UES (upper esophageal sphincter) Diverticulum Zenker’s diverticulum Mallory-Weiss Syndrome Melena Hematemesis Mucosal webs Plummer-Vinson Syndrome Rings Longitudinal lacerations near gastroesophageal junction. Often from severe vomiting. Black tar stools upper GI bleed Throwing up blood Obstructive wedge-like fibrovascular connective tissue and overlying epithelium Esophageal webs + iron-deficiency anemia, glossitis, and cheilosis Like webs, but circumferential. A webs: upper (squamous), B webs: lower esophagus Traction diverticulum Diverticulum in the mid esophagus Pyrosis Heartburn Epiphrenic diverticulum Diverticulum just above LES (lower esophageal sphincter) Varices Distention of esophageal veins in portal circulation Hiatal hernia Herniation of visceral material through diaphragm hiatus Dyspepsia Indigestion, pain in upper abdomen Disease Signs & Symptoms Pathogenesis Histology Atresia + fistula - aspiration, - Tracheoesophageal fistulas are more common. - suffocation - Occurs most often at tracheal bifurcation and - pneumonia frequently associated with atresia. - fluid and electrolyte imbalances - Associated anomalies are congenital heart disease Most common Must be corrected early b/c incompatible with life. and neurologic, GU, and other GI anomalies. Stenosis - GERD, radiation, scleroderma, caustic injury - Fibrous thickening of walls - Progressive dysphagia; if severe, obstruction - Usually due to severe injury and resultant scarring Mucosal Webs - Upper esophagus - Ledge-like protrusions from into the lumen - Semicircumferential - Most often encountered in women >40 years old and are of uncertain etiology - Episodic dysphagia when swallowing large amounts of food. Mucosal Rings - Lower esophagus - Concentric Plummer-Vinson - Combination of 1) upper webs, 2) iron deficiency Syndrome anemia with 3) glossitis and 4)cheilosis - Risk of post-cricoid carcinoma Achalasia 1) ↓ LES relaxation - Primary (idiopathic) (most common) 2) ↑LES tone o dysfunction of inhibitory neurons in the distal 3) Aperistalsis of the esophagus esophagus - Manifests in young adulthood o neuronal degeneration of intrinsic or extrinsic - Leads to progressive dysphagia, regurgitation, and (vagal) nerves aspiration - Secondary - Aspiration pneumonia, airway obstruction, candidiasis, o Chagas disease (Trypanosoma cruzi) - Dilated esophagus above LES lower esophageal diverticula and 5% squamous cell o lesions of vagal motor nuclei (i.e. polio) - Diminished myenteric ganglia in carcinoma of the esophagus o diabetic autonomic neuropathy body of esophagus and possibly o Infiltrative disorders (malignancy, sarcoidosis, etc.) in the region of the LES Disease Hiatal Hernia - Cause unknown - Can cause GERD Diverticulae Zenker (Pharyngeoesophageal) Signs & Symptoms - Hernia of part of stomach thru esophageal foramen - Separation/widening of diaphragmatic crura - 1-20% of adult population affected - Incidence increases with age, but also seen in kids - Complications o Ulcerations, bleeding and perforations o Strangulation or obstruction (paraesophageal hernias) o Reflux esophagitis Traction - accumulates food, causing : o regurgitation o dysphagia o a neck mass o aspiration pneumonia - asymptomatic Epiphrenic - nocturnal regurgitation of massive amounts of fluid Lacerations (Mallory-Weiss Syndrome) - Most commonly seen in alcoholics and associated with severe retching or vomiting - Underlying hiatal hernia is a known risk factor - Accounts for 5-10% of the upper GI bleeding episodes - Bleeding usually ceases without surgical intervention, but massive hematemesis may occur - Infection of mucosal defect can lead to inflammatory ulcer or mediastinitis Circulatory Disorders Esophageal Varices Portal hypertension - dilated, tortuous vessels - ↑pressure in plexus gives rise to varices - Usually asymptomatic until rupture With rupture, there is life-threatening, massive hematemesis (but varices only cause <50% of all hematemesis episodes) Half the deaths of patients with advanced cirrhosis of the liver result from a ruptured varix. Death from hemorrhage or triggered hepatic coma Treatment usually requires endoscopic injection of a thrombotic agent (sclerotherapy) or balloon tamponade 40-50% of patients die in the first bleeding episode; similar mortality rate in repeat episodes Pathogenesis Histology - Sliding (axial): 95% of cases o cardia of stomach herniates upward, as if it slid straight up o Bell-shaped dilation of the stomach above the diaphragm bounded by diaphragm - Paraesophageal (rolling or nonaxial): o separate portion of the stomach (usually greater curvature) herniates alongside of the esophagus o Associated w/ previous surgery (operations for sliding hernias) - located immediately above the UES - caused by cricopharyngeal motor dysfunction w/ or w/out GERD and diminished luminal size of the UES - located at the midpoint of the esophagus - caused by scarring from mediastinal lymphadenitis(?), motor dysfunction, or congenital - located above LES - associated with discoordinated peristalsis and LES relaxation - Longitudinal tears at the esophagogastric junction Found astride the or gastric cardia esophagogastric junction or in - Gastric musculature fails to relax properly, leading to the proximal gastric mucosa massive dilation and tearing of the wall - May involve only mucosa, but can penetrate and cause rupture (Boerhaave syndrome) - Most often associated with ALCOHOLIC CIRRHOSIS and develop in 90% of cirrhotic patients - Collateral bypass channels develop where portal and caval systems are in communication. 1) Portal vein hypertension 2) Gastro-esophageal anastamoses a. Coronary Veins in Stomach b. Submucosal Plexus In Distal Esophagus Rupture if >5mm 3) Azygous vein 4) Systemic circulation Varix Inflammatory Disorders Disease Signs & Symptoms Esophagitis - Inflammation of the esophageal mucosa - 5% of adult population in US and Western countries Gastroesophageal - Reflux of gastric into the lower esoph. Reflux Disease - Most important cause of esophagitis (GERD) - Severity of the symptoms does NOT correlate to degree of histologic change - Usually limited to - Symptoms adults >40 yrs o Heartburn o Regurgitation of a sour brash o Dysphagia o Hematemesis, Melena (if severe) - Complications o Ulceration, bleeding, healing o Barrett esophagus o Stricture Barrett Esophagus - Metaplastic change whereby squamous epithelium columnar epithelium due to - Common prolonged injury complication of - Alteration in the differentiation program of long-standing esophageal mucosal stem cells GERD (up to 10%) - 40-60 yr old, - Single most important risk factor for white, M>F esophageal adenocarcinoma - Secondary o 30-40x with > 3cm Barrett change complications of local ulceration - Two requirements for diagnosis with bleeding and 1. Endoscopy: columnar epi ↑the GE jxn stricture 2. Histologic biopsy: intestinal metaplasia Infectious & Chemical Esophagitis - Infectious o Viral: HSV and CMV in immunosuppressed o Fungal (Immunosuppressed or Diabetics) Candidiasis (most common) Mucormycosis and Aspergillosis (rare) - Mucosal irritants o Corrosives & alkalis, cytotoxic drugs, alcohol, hot fluids, heavy smoking - Uremia Pathogenesis - Caused by a variety of physical, chemical, and biologic agents Histology - Cause: mostly action of gastric juices on esophagus o Sliding hiatal hernia o Decreased LES tone Alcohol, chocolate, cigarette smoking, estrogen CNS Depressants e.g. morphine, valium Nasogastric intubation o Inadequate or slowed esophageal clearance o Delayed gastric emptying & ↑ gastric volume o Reduced reparative capacity of esophageal mucosa by extended exposure to gastric juices - Sheets, patches, or a band of red velvety epithelium (gross and endoscopy). - Squamous epithelium replaced by columnar, with either gastric surface and glandular mucus-secreting cells or mixture of gastric and intestinal epithelium. - Look for dysplasia as precursor to malignancy HSV: “Punched out” ulcers HSV: Nuclear inclusions 1. Inflammatory cells in epithelial layer e.g. neutrophils (indicates severity), eosinophils (early), and lymphocytes 2. Basal zone hyperplasia in excess of 20% of epithelial thickness. 3. Elongation of lamina propria and congestion. Neoplasms Disease Squamous Cell Carcinoma - 90% of esophageal cancers worldwide; but equal incidence to adenocarcioma in the US - Adults over 50 yrs - M:F; 2:1-20:1; 4:1 in US - Incidence varies between regions - Blacks throughout the world have a higher risk, 4X in US Adenocarcinoma - Incidence equal to squamous cell carcinoma in the US - >40 with median age 60 - M>W; whites > black. Signs & Symptoms - Clinical Features o Insidious onset with late development of symptoms o Dysphagia, obstruction, cachexia, debilitation o Patients often adjust their diets and fail to report symptoms until more severe - Complications o Hemorrhage and sepsis from ulceration o Aspiration from tracheoesophageal fistula - Prognosis o 5-year survival 9%; 75% for superficial lesions; 25% for surgical resection of advanced lesions o Recurrence local and at distant sites o Lymph node metastasis reduces survival rate o Screening programs are less successful in USA so prognosis is worse Pathogenesis Etiology and Pathogenesis - Dietary, environmental, and genetic - US - Alcohol and tobacco - Other countries - fungi and nitrosamines o Less use of these preservatives in US - Chronic esophagitis dysplasia cancer Histology - Protruded (exophytic) (60%) - Flat (15%): infiltrative o Spreads in wall, thickens wall and arrows lumen - Excavated (25%): necrotic ulceration o deep infiltration sometimes fistulates into trachea (leading to pneumonia) or into aorta (leading to hemorrhage into the mediastinum and pericardium) - Begins in situ - 20% upper third, 50% middle third and 30% lower third - Quite large by time symptoms elaborated - Local circumferential and longitudinal spread by lymphatics - Metastasizes to regional nodes - Dysphagia predominant sign with weight loss, hemorrhage, chest pain and vomiting also noted. - Prognosis - 5 year - <20% overall - >80% with resected superficial tumors - Virtually all arise in Barrett esophagus - 10% lifetime risk in Barret esophagus - Documented genetic alterations o p53 protein over expression in Barrett esophagus o p53 functional inactivation due to point mutations leading to loss of cell cycle control Histology 1) Distal esophagus and may invade cardia 2) Start as flat or raised patches that become either large nodules or infiltrate and ulcerate. 3) Most are mucin producers demonstrating intestinal-type epithelium although some gastric-type is observed. Histology