Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
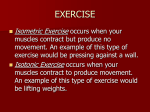
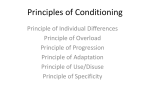
ORIGINAL RESEARCH 䡲 MUSCULOSKELETAL IMAGING Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Fatty Muscle Atrophy: Prevalence in the Hindfoot Muscles on MR Images of Asymptomatic Volunteers and Patients with Foot Pain1 Daniel T. Schmid, MD Juerg Hodler, MD, MBA Bernard Mengiardi, MD Christian W. A. Pfirrmann, MD Norman Espinosa, MD Marco Zanetti, MD Purpose: To determine prevalence and degree of fatty muscle atrophy in plantar foot muscles in asymptomatic volunteers and in patients with foot pain. Materials and Methods: Institutional review board approval and informed consent were obtained. The prevalence and degree of fatty muscle atrophy were evaluated with magnetic resonance imaging in the abductor digiti minimi (ADM), flexor digitorum brevis (FDB), abductor hallucis (AH), and quadratus plantae (QP) muscles in 80 asymptomatic volunteers (mean age, 48 years; range, 23– 84 years) and 80 patients with foot pain (mean age, 48 years; range, 20 – 86 years). Muscles were characterized as normal (grade 0) or as having mild (grade 1) or substantial (grade 2) fatty atrophy by two readers separately. Results of visual grading for both readers were compared by using the Mann-Whitney test. Associations between age and degree of fatty muscle atrophy were assessed by using the Kruskal-Wallis test. Results: Readers 1 and 2 found substantial fatty atrophy of the ADM muscle in four (5%) and five (6%) volunteers, respectively, and in three (4%) and nine (11%) patients, respectively. One reader diagnosed substantial fatty atrophy of the AH muscle in three (4%) volunteers and of the FDB muscle in two (2%) volunteers. Prevalence for the QP muscle varied between 0% and 1%. An association between age and degree of fatty atrophy of the ADM muscle was found for volunteers by both readers and for patients by reader 1 (P ⬍ .01). Conclusion: Prevalence of fatty muscle atrophy of the ADM muscle— classically considered to represent entrapment neuropathy—is between 4% and 11% in both asymptomatic volunteers and patients with foot pain, and it increases with age. 娀 RSNA, 2009 1 From the Departments of Radiology (D.T.S., J.H., B.M., C.W.A.P., M.Z.) and Orthopedic Surgery (N.E.), Orthopedic University Hospital Balgrist, Forchstrasse 340, CH-8008 Zurich, Switzerland. Received January 6, 2009; revision requested March 4; revision received April 21; accepted April 26; final version accepted May 11. Address correspondence to M.Z. (e-mail: [email protected] ). 姝 RSNA, 2009 160 radiology.rsna.org ▪ Radiology: Volume 253: Number 1—October 2009 MUSCULOSKELETAL IMAGING: Prevalence of Fatty Atrophy of Hindfoot Muscles C hronic pain in the hindfoot can be caused by a variety of abnormalities, many of which can be detected with magnetic resonance (MR) imaging. These diagnoses include osteochondral lesions (1), stress fractures (2,3), ligament lesions (4), tendon disorders (5), and rheumatologic disorders (6,7). Nerve entrapment is a cause of chronic hindfoot pain that can easily be overlooked on MR images. Nerve entrapment may be the cause of heel pain in up to 20% of patients (8–11). The most common entrapment disorder in the hindfoot is entrapment of the first branch of the lateral plantar nerve, also called Baxter neuropathy (8). The entrapment is postulated to occur as the nerve passes between the deep fascia of the abductor hallucis (AH) muscle and the medial caudal margin of the medial head of the quadratus plantae (QP) muscle or as the nerve passes just anterior to the medial calcaneal tuberosity. Plantar spur formation at the medial calcaneal tuberosity has been reported to be a possible cause of entrapment (8–11). MR imaging cannot typically be used to prove compressive (entrapment) neuropathies by means of signal intensity abnormalities or morphologic changes of peripheral nerves themselves. Selective muscle edema Advances in Knowledge 䡲 The prevalence of fatty muscle atrophy of the abductor digiti minimi (ADM), flexor digitorum brevis, abductor hallucis, or quadratus plantae muscles in asymptomatic volunteers is low (⬍8%) and is similar to that in patients with foot or ankle pain who are referred for MR imaging. 䡲 The prevalence of fatty atrophy of the ADM muscle in both volunteers and patients (4%–11%) is higher than that of the flexor digitorum brevis (0%–2%), abductor hallucis (1%– 4%), and quadratus plantae (0%–1%) muscles. 䡲 The prevalence of fatty atrophy of the ADM muscle increases with age. and fatty atrophy are indirect signs of entrapment neuropathy on MR images (12). Fatty atrophy of the abductor digiti minimi (ADM) muscle may reflect chronic compression of the inferior calcaneal nerve, which is associated with the clinical diagnosis of Baxter neuropathy. However, there is debate as to whether selective fatty muscle atrophy also occurs unrelated to nerve entrapment. Recht et al (9) found selective fatty atrophy of the ADM muscle in 38 (6%) of 602 patients referred for foot and ankle MR imaging, but only one patient had clinical and electrophysiologic signs of Baxter neuropathy. Another study (13) demonstrated a significant association of ADM muscle atrophy with calcaneal spur formation, plantar fasciitis, and advancing age. Fatty atrophy of intrinsic foot muscles has also been described (14) in patients with diabetic neuropathy. Our hypothesis was that fatty muscle atrophy could be found in asymptomatic volunteers on MR images and does not have to be related to the presence of a specific diagnosis. We evaluated the prevalence and degree of fatty replacement of the muscles around the heel (ie, ADM, flexor digitorum brevis [FDB], AH, and QP muscles) in an asymptomatic population and compared the findings with those in patients with foot pain. Materials and Methods Volunteers Eighty asymptomatic volunteers (38 men, 42 women; mean age, 48 years; range, 23– 84 years) were studied. MR images of these volunteers were acImplications for Patient Care 䡲 The clinical relevance of fatty atrophy of the ADM muscle is uncertain because its prevalence is similar in patients with foot pain and asymptomatic volunteers. 䡲 Radiologists should exercise caution in attributing clinical importance to fatty atrophy of the ADM muscle when it is an incidental finding. Radiology: Volume 253: Number 1—October 2009 ▪ radiology.rsna.org Schmid et al quired between August 2003 and July 2004 for another study (15), which did not focus on muscles. Inclusion criteria were (a) no current pain in the foot or ankle, (b) no prior foot or ankle surgery, (c) no visit to a physician because of foot and ankle complaints, (d) no trauma or injury to the foot or ankle during the previous 2 years, and (e) no known systemic inflammatory disease. At least six men and six women were included for each decade of life between 20 and 70 years. Three men and five women aged between 70 and 84 years were also included. The side imaged (right or left) was selected randomly. The portion of the study in asymptomatic volunteers was approved by the institutional review board. Informed consent was obtained from each volunteer. Our institutional review board does not require approval for the review of patients’ records or images; however, according to a law protecting patients’ rights, patients have to be asked to give permission for anonymized review of their medical data for scientific purposes before the examination. All patients in our study granted permission. Patients Eighty patients (38 men, 42 women; mean age, 48 years; range, 20 – 86 years) who had been referred for MR imaging because of foot pain were in- Published online before print 10.1148/radiol.2531090035 Radiology 2009; 253:160 –166 Abbreviations: ADM ⫽ abductor digiti minimi AH ⫽ abductor hallucis FDB ⫽ flexor digitorum brevis QP ⫽ quadratus plantae Author contributions: Guarantors of integrity of entire study, D.T.S., M.Z.; study concepts/study design or data acquisition or data analysis/interpretation, all authors; manuscript drafting or manuscript revision for important intellectual content, all authors; approval of final version of submitted manuscript, all authors; literature research, D.T.S., J.H., N.E., M.Z.; clinical studies, all authors; statistical analysis, D.T.S., M.Z.; and manuscript editing, all authors Authors stated no financial relationship to disclose. 161 MUSCULOSKELETAL IMAGING: Prevalence of Fatty Atrophy of Hindfoot Muscles cluded. Patients were imaged between December 2007 and June 2008. Patients were consecutively included to match the age and sex of the volunteers. Exclusion criteria were (a) prior foot surgery, (b) known trauma to the foot or ankle, (c) infection (eg, skin ulceration, osteomyelitis), (d) tumors previously diagnosed with another imaging modality or biopsy, and (e) severe congenital malformation. Patients were excluded on the basis of clinical diagnosis and patient history, not MR imaging findings. The primary clinical indications for MR imaging and the main MR imaging findings are listed in Table 1. MR Imaging MR imaging was performed on one of three 1.5-T systems (Magnetom Symphony [n ⫽ 110], Magnetom Espree [n ⫽ 23], or Magnetom Avanto [n ⫽ 27]; Siemens Medical Solutions, Erlangen, Germany) with a circularly polarized sendreceive extremity coil (Siemens Medical Solutions). T1-weighted (repetition time msec/echo time msec, 572/14; section thickness, 3–3.5 mm) and T2-weighted Schmid et al (4139/86; section thickness, 3–3.5 mm) coronal images were used to assess the degree of fatty muscle atrophy and to measure the cross-sectional area of the individual muscles. Volunteers and patients were imaged in the supine position with one foot (randomly chosen in volun- teers, painful foot in patients) in the coil in a neutral position. Image Interpretation All original Digital Imaging and Communications in Medicine data sets were rendered anonymous so that the readers Table 1 Primary Clinical Indications for and Main Findings at MR Imaging in the Patient Group (n ⴝ 80) Characteristic Plantar fasciitis or thickened plantar fascia Tendon disorder Osteoarthritis of one or more hindfoot joints Stress fracture Osteochondral lesions Neoplastic or tumorlike lesions Lesions of ankle ligaments Osteonecrosis Synovitis or spondylarthritis Tarsal tunnel syndrome Normal MR findings Indication* Finding 8 (10) 26 (32) 16 (20) 8 (10) 7 (9) 3 (4) 5 (6) 5 (6) 2 (2) 2 (2) NA 15 (19) 17 (21) 10 (12) 8 (10) 6 (8) 6 (8)† 5 (6) 2 (2) 2 (2) 0 (0) 9 (11) Note.—Data are numbers of patients, with percentages in parentheses. NA ⫽ not applicable. * Data do not sum to 80 because some patients had more than one indication for imaging. † Pigmented villonodular synovitis or scar tissue (n ⫽ 2), ganglion (n ⫽ 3), or osteochondroma (n ⫽ 1). Figure 1 Figure 1: (a– c) Coronal T1-weighted fast spin-echo MR images illustrate different grades of fatty atrophy of ADM muscle: (a) grade 0 (52-year-old male volunteer), (b) grade 1 (70-year-old female volunteer), and (c) grade 2 (44-year-old female patient). 162 radiology.rsna.org ▪ Radiology: Volume 253: Number 1—October 2009 MUSCULOSKELETAL IMAGING: Prevalence of Fatty Atrophy of Hindfoot Muscles Figure 2 Schmid et al would be blinded to whether images belonged to a patient or to a volunteer. Image interpretation and measurements were performed by using open-source software (OsiriX, version 3.2.1; OsiriX Imaging Software, Geneva, Switzerland) (16) on a computer (Mac OS X, version 10.5.4; Apple, Cupertino, Calif). Table 3 Cross-sectional Areas of the Hindfoot Muscles in Volunteers and Patients Muscle and Group ADM Volunteers Patients FDB Volunteers Patients AH Volunteers Patients QP Volunteers Patients Figure 2: Coronal T1-weighted fast spin-echo MR image of a 60-year-old male volunteer at level of cross-sectional area measurement. Osseous insertion of tibiocalcaneal ligament (arrowheads) is visible. Regions of interest (white boundaries) were drawn around ADM, FDB, AH, and QP muscles. Cross-sectional Area (cm2) 2.5 ⫾ 0.6 (0.3–4.1) 2.3 ⫾ 0.6 (0.4–3.5) 1.5 ⫾ 0.5 (0.0–2.8) 1.5 ⫾ 0.6 (0.1–3.7) 2.1 ⫾ 0.7 (0.0–3.7) 2.0 ⫾ 0.8 (0.0–4.1) 0.8 ⫾ 0.4 (0.2–2.1) 0.8 ⫾ 0.6 (0.0–4.3) Note.—Data are means ⫾ standard deviations, with ranges in parentheses. By using analysis of variance, no significant differences were found between patients and volunteers for the area of any of the muscles. A qualitative grading of fatty muscle atrophy was determined by two independent readers (B.M. and J.H., with 5 and 20 years experience in musculoskeletal radiology, respectively). Grading of fatty atrophy was performed separately for the ADM, FDB, AH, and QP muscles. A three-point scale was used to grade the degree of fatty muscle atrophy on coronal T1-weighted images: 0 ⫽ normal muscle, 1 ⫽ mild fatty atrophy with more muscle than fat, and 2 ⫽ substantial fatty atrophy with more fat than muscle or equal parts fat and muscle (Fig 1). The readers were asked to consider the entire muscle volume for grading, not just a single section, and to read as they would during clinical routine. To calibrate the evaluation, each reader had a set of reference images with different grades of fatty muscle atrophy available. Measurement of the crosssectional area of the ADM, FDB, AH, and QP muscles was performed (D.T.S., a 4th year resident) on the T1-weighted coronal MR image at the level where the bony insertion of the tibiocalcaneal ligament at the calcaneus was best visualized (Fig 2). Regions of interest were defined for each muscle at 200% zoom to minimize measurement errors. Measurements were repeated in 32 (20%) of 160 subjects to assess variability. Table 2 Fatty Muscle Atrophy Grading for 80 Volunteers and 80 Patients according to Reader and Interobserver Agreement Muscle and Group ADM Volunteers Patients FDB Volunteers Patients AH Volunteers Patients QP Volunteers Patients Reader 1* Grade 0 Reader 2* Age (y)† Reader 1* Grade 1 Reader 2* Age (y)† Reader 1* Grade 2 Reader 2* Age (y)† Value 65 (81) 57 (71) 66 (83) 56 (70) 45 ⫾ 15 45 ⫾ 15 11 (14) 20 (25) 9 (11) 15 (19) 61 ⫾ 13 58 ⫾ 16 4 (5) 3 (4) 5 (6) 9 (11) 71 ⫾ 9 61 ⫾ 18 0.679 0.556 78 (98) 75 (94) 75 (94) 76 (95) 48 ⫾ 16 48 ⫾ 17 1 (1) 5 (6) 3 (4) 4 (5) 77 ⫾ 5 51 ⫾ 20 1 (1) 0 (0) 2 (2) 0 (0) 69 ⫾ 11 ... 0.560 0.412 75 (94) 69 (86) 74 (93) 73 (91) 48 ⫾ 16 47 ⫾ 16 4 (5) 10 (13) 3 (4) 6 (8) 69 ⫾ 9 59 ⫾ 18 1 (1) 1 (1) 3 (4) 1 (1) 73 ⫾ 11 86 ⫾ 0 0.329 0.386 68 (85) 61 (76) 69 (86) 64 (80) 47 ⫾ 15 47 ⫾ 16 11 (14) 19 (24) 11 (14) 15 (19) 62 ⫾ 14 55 ⫾ 18 1 (1) 0 (0) 0 (0) 1 (1) 76 ⫾ 0 24 ⫾ 0 0.496 0.421 * Data are numbers of subjects, with percentages in parentheses. † Data are means ⫾ standard deviations. Radiology: Volume 253: Number 1—October 2009 ▪ radiology.rsna.org 163 MUSCULOSKELETAL IMAGING: Prevalence of Fatty Atrophy of Hindfoot Muscles Schmid et al Table 4 Findings at Secondary Review of Subjects with Substantial (Grade 2) Fatty Atrophy according to Muscle Finding Plantar fasciitis Calcaneus spur Stress fracture Osteoarthritis or osteochondral lesion Posterior tibial tendon partial rupture Peroneal tendon luxation Spring ligament insufficiency Calcaneus avulsion fracture* Clubfoot deformity* Otherwise normal MR findings ADM (n ⫽ 14) Volunteers Patients FDB (n ⫽ 2) Volunteers Patients AH (n ⫽ 4) Volunteers Patients QP (n ⫽ 2) Volunteers Patients 0 0 1 0 0 1 0 0 0 3 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 1 0 0 0 1 0 0 0 0 0 0 0 0 0 0 5 1 1 1 1 0 1 1 1 1 0 0 0 1 0 0 0 0 0 0 0 0 1 1 0 0 0 0 0 0 0 0 0 1 0 0 0 1 1 0 Note.—Data are numbers of patients. Data may sum to more than the number of findings of substantial atrophy because patients could have more than one finding. * Findings in the same patient. Secondary Review In subjects in whom at least one reader diagnosed substantial fatty muscle atrophy, a secondary review of all MR images and available clinical charts was performed in consensus by a musculoskeletal radiologist (M.Z., 16 years experience) and an orthopedic foot surgeon (N.E., 8 years experience). Diagnoses potentially related to nerve entrapment (eg, masses in or around the lateral plantar nerve, plantar fasciitis) were noted. Statistical Analysis Statistical analysis was performed with software (SPSS, version 16.0.1 for Apple Macintosh; SPSS, Chicago, Ill). Descriptive statistics and analysis of variance were used to evaluate and compare crosssectional areas of the ADM, FDB, AH, and QP muscles between the volunteer and patient groups. The Mann-Whitney test was used to compare the grading of fatty muscle atrophy and mean muscle cross-sectional area between the volunteer and patient groups. The Cohen statistic was used to evaluate interobserver agreement for the grading of fatty muscle atrophy. According to Landis and Koch (17), values smaller than 0.20 indicate poor agreement; 0.21– 0.40, fair agreement; 0.41– 0.60, moderate agreement; 0.61– 0.80, good agreement; and 0.81– 1.00, very good agreement. The KruskalWallis test was used to analyze the association between age and the degree of fatty muscle atrophy. 164 Bonferroni adjustment was applied to adjust for multiple comparisons (age vs fatty muscle atrophy grade and crosssectional muscle diameter vs fatty muscle atrophy grade for two readers and comparison of the cross-sectional muscle areas between volunteers and patients). P values less than .01 were considered to indicate a significant difference. Intraclass correlation coefficients were used to assess measurement variability of the crosssectional area of the ADM, FDB, AH, and QP muscles. Results Substantial (grade 2) fatty muscle atrophy of at least one of the four muscles (ADM, AH, FDB, and QP) was observed by at least one reader in six (8%) of 80 volunteers and in 10 (12%) of 80 patients. For the ADM muscle, grade 2 fatty atrophy was found in four (5%) volunteers and three (4%) patients by reader 1 and in five (6%) volunteers and nine (11%) patients by reader 2. For the FDB muscle, grade 2 fatty atrophy was reported in one (1%) volunteer by reader 1 and in two (2%) volunteers by reader 2 but in none of the patients by either reader. For the AH muscle, grade 2 fatty atrophy was reported in one (1%) volunteer and one (1%) patient by reader 1 and in three (4%) volunteers and one (1%) patient by reader 2. For the QP muscle, grade 2 fatty atrophy was seen in one (1%) volunteer and no patients by reader 1 and in no volunteers and one (1%) patient by reader 2. Interobserver agreement for grading between readers 1 and 2 was good for the ADM in volunteers and moderate for the ADM in patients and for the FDB and the QP in volunteers and patients. Only fair agreement was reached for the AH in volunteers and patients (Table 2). No significant differences in the degree of fatty atrophy of the ADM, FDB, AH, and QP muscles were found between volunteers and patients. However, mild (grade 1) fatty muscle atrophy was noted slightly more frequently in patients than it was in volunteers (Table 2). Grade 2 fatty atrophy of the AH, FDB, and QP muscles occurred only in combination with grade 2 fatty atrophy of the ADM muscle in all but one case. In this patient, selective grade 2 fatty atrophy of the AH muscle was observed in combination with an osteoporotic stress fracture of the middle cuneiform bone. A significant association between age and degree of fatty muscle atrophy was found for the ADM muscle in volunteers (P ⬍ .001 for both readers) and in patients (P ⫽ .007 for reader 1, not significant for reader 2). For the FDB, AH, and QP muscles, P values could not be calculated because of the small number of cases (n ⬍ 5) with grade 2 fatty muscle atrophy. Large variability of cross-sectional area for the ADM, FDB, AH, and QP muscles was found between individuals in both the volunteer and patient groups radiology.rsna.org ▪ Radiology: Volume 253: Number 1—October 2009 MUSCULOSKELETAL IMAGING: Prevalence of Fatty Atrophy of Hindfoot Muscles Figure 3 Figure 3: Coronal (a) T1- and (b) T2-weighted fast spin-echo and (c) sagittal short inversion time inversion-recovery MR images of a 44-year-old female patient with substantial fatty atrophy of the ADM muscle (arrowheads in a and b) and concomitant plantar fasciitis (arrows in c). (Table 3). No significant differences in the mean cross-sectional area of the ADM, FDB, AH, or QP muscles were found between volunteers and patients. There was no significant correlation between the grade of fatty atrophy and cross-sectional area of the evaluated muscles. Measurement variability was assessed by repeated measurements in 32 (20%) of 160 subjects. The intraclass correlation coefficients for the corresponding measurements were 0.952 for the ADM muscle, 0.967 for the FDB muscle, 0.968 for the AH muscle, and 0.988 for the QP muscle. The results of the secondary case re- view of subjects with substantial (grade 2) muscle atrophy are listed in Table 4. In volunteers with fatty atrophy of the ADM muscle, plantar fasciitis was not observed; however, it was the most common finding in the patient group (Fig 3). Discussion Our study provides information about the prevalence of fatty atrophy of the plantar hindfoot muscles (ADM, FDB, AH, and QP) in asymptomatic individuals. For readers 1 and 2 in our study, the frequencies of fatty atrophy of the ADM muscle in Radiology: Volume 253: Number 1—October 2009 ▪ radiology.rsna.org Schmid et al volunteers (5% and 6%, respectively) were similar to those in patients (4% and 11%, respectively). These rates are comparable to data in a large patient study (6%, 38 of 602) (9). In our study, three (50%) of six volunteers and six (67%) of nine patients with substantial fatty atrophy of the ADM muscle were men, but in previous studies, most of the affected patients were women (9,18). Recht et al (9) found that 76% (29 of 38) of subjects with fatty atrophy of the ADM muscle were women. The higher percentage of women in the group with fatty atrophy of the ADM muscle cannot be solely explained by the overall percentage of women in the study (64%, 387 of 602) (9). The ADM and QP muscles receive their motor supply from branches of the lateral plantar nerve. The AH and FDB are innervated by the medial plantar nerve. In neither volunteers nor patients with grade 2 fatty muscle atrophy were we able to detect direct external compression by a soft tissue mass on the first branch of the lateral plantar nerve (the Baxter nerve) (8). This finding may be explained by the multitude of causes of nerve compression. Clinically, entrapment of the first branch of the lateral plantar nerve occurs mainly between the fascia of the AH muscle and the medial caudal margin of the QP muscle. Edema within the AH muscle or repetitive trauma may compromise the nerve as it courses underneath the plantar ligament or through the osseous canal between the calcaneus and the flexor digitorum brevis muscle. Another factor that may cause injury is excessive pronation. Additionally, hypertrophy of the QP, accessory muscles, abnormal bursae, and phlebitis within the venous plexus have been described as potential causes of entrapment neuropathy (19–21). The lack of a mass lesion or signs of physical nerve compression on MR images does not exclude nerve compression as the cause of fatty muscle atrophy. Fatty atrophy of the intrinsic muscles may be similar to that seen in the rotator cuff muscles in Parsonage-Turner syndrome (22,23) or in quadrilateral syndrome (24,25). The most likely cause of Parsonage-Turner syndrome may be viral or autoimmune brachial neuritis. Axillary 165 MUSCULOSKELETAL IMAGING: Prevalence of Fatty Atrophy of Hindfoot Muscles nerve damage owing to traction injuries has also been discussed as a cause. A similar mechanism might also be responsible for lesions of the plantar nerves (26). In another study (13), the association between fatty atrophy of the ADM muscle and the presence of plantar fasciitis underlines the possibility that mechanical entrapment may have occurred. Our findings of plantar fasciitis in five of 14 individuals with fatty atrophy of the ADM muscle further highlight this possible connection. In instances of fatty atrophy of muscles with different motoric supply, a more proximal entrapment (posterior tibial nerve), neuritis, or systemic neuropathy (eg, diabetic neuropathy) should also be considered. In most cases of entrapment neuropathy, the point of entrapment will not be visible on MR images. Measurement of cross-sectional muscle area at our reference plane revealed large variability among individual subjects even when no signs of fatty muscle atrophy were present. These large interindividual differences hamper the use of such data for quantitative muscle analysis. Quantitative muscle analysis of the hindfoot muscles seems to be less reliable than that in other anatomic regions. A similar quantitative assessment of the rotator cuff muscles by using cross-sectional areas was shown to be more reliable (27). We acknowledge that our study had limitations. The age- and sex-matched patient group included patients with pain of the foot or ankle regardless of the underlying cause. Clinical information about coexisting diseases (eg, diabetes mellitus or peripheral neuropathy) was not available in some patients and could therefore not be included in our study. Another limitation was that we performed a two-dimensional cross-sectional measurement rather than a three-dimensional volumetric measurement of the ADM, FDB, AH, and QP muscles. In addition, we used a narrow scale for the visual grading of fatty muscle atrophy, discriminating only normal from mild and substantial fatty muscle atrophy. The narrow scale was used because subtle changes in mild fatty atrophy are difficult to assess in small muscles. Moreover, atrophy grade may vary from one section to the next. In conclusion, the prevalence of substantial (grade 2) fatty muscle atrophy of 166 Schmid et al the ADM, FDB, AH, and QP muscles in asymptomatic volunteers is low and is similar to that in patients with pain of the foot and ankle who were referred for MR imaging. The prevalence of substantial fatty atrophy of the ADM muscle (4%–11%) is higher than that of the FDB (0%–2%), AH (1%–4%), and QP (0%–1%) muscles. The relatively high prevalence of plantar fasciitis in patients and volunteers with ADM muscle atrophy (five of 14) indicates that some association may exist between plantar fasciitis and fatty atrophy of the ADM muscle. Prevalence of fatty atrophy of the ADM muscle also increases with age. References 1. De Smet AA, Fisher DR, Burnstein MI, Graf BK, Lange RH. Value of MR imaging in staging osteochondral lesions of the talus (osteochondritis dissecans): results in 14 patients. AJR Am J Roentgenol 1990;154:555–558. 2. Lee JK, Yao L. Stress fractures: MR imaging. Radiology 1988;169:217–220. 3. Umans H, Pavlov H. Insufficiency fracture of the talus: diagnosis with MR imaging. Radiology 1995;197:439 – 442. 4. Miller MD, Osborne JR, Gordon WT, Hinkin DT, Brinker MR. The natural history of bone bruises: a prospective study of magnetic resonance imaging-detected trabecular microfractures in patients with isolated medial collateral ligament injuries. Am J Sports Med 1998;26: 15–19. 5. Schweitzer ME, Karasick D. MR imaging of disorders of the posterior tibialis tendon. AJR Am J Roentgenol 2000;175:627– 635. 12. Kim S, Choi JY, Huh YM, et al. Role of magnetic resonance imaging in entrapment and compressive neuropathy: what, where, and how to see the peripheral nerves on the musculoskeletal magnetic resonance image. I. Overview and lower extremity. Eur Radiol 2007;17: 139 –149. 13. Chundru U, Liebeskind A, Seidelmann F, Fogel J, Franklin P, Beltran J. Plantar fasciitis and calcaneal spur formation are associated with abductor digiti minimi atrophy on MRI of the foot. Skeletal Radiol 2008;37:505–510. 14. Bus SA, Yang QX, Wang JH, Smith MB, Wunderlich R, Cavanagh PR. Intrinsic muscle atrophy and toe deformity in the diabetic neuropathic foot: a magnetic resonance imaging study. Diabetes Care 2002;25:1444 –1450. 15. Mengiardi B, Pfirrmann CW, Vienne P, Hodler J, Zanetti M. Medial collateral ligament complex of the ankle: MR appearance in asymptomatic subjects. Radiology 2007;242:817–824. 16. Rosset A, Spadola L, Ratib O. OsiriX: an opensource software for navigating in multidimensional DICOM images. J Digit Imaging 2004; 17:205–216. 17. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;33:159 –174. 18. Stanczak JD, McLean VA, Yao L. Atrophy of the abductor digiti minimi muscle: marker of neuropathic heel pain syndrome? [abstr]. Radiology 2001;221(P):522. 19. Baxter DE, Pfeffer GB. Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229 –236. 20. Sridhara CR, Izzo KL. Terminal sensory branches of the superficial peroneal nerve: an entrapment syndrome. Arch Phys Med Rehabil 1985;66:789 –791. 21. Radin EL. Tarsal tunnel syndrome. Clin Orthop Relat Res 1983;181:167–170. 6. Erdem CZ, Sarikaya S, Erdem LO, Ozdolap S, Gundogdu S. MR imaging features of foot involvement in ankylosing spondylitis. Eur J Radiol 2005;53:110 –119. 22. Parsonage MJ, Turner JW. Neuralgic amyotrophy: the shoulder-girdle syndrome. Lancet 1948;1:973–978. 7. Weishaupt D, Schweitzer ME, Alam F, Karasick D, Wapner K. MR imaging of inflammatory joint diseases of the foot and ankle. Skeletal Radiol 1999;28:663– 669. 23. Scalf RE, Wenger DE, Frick MA, Mandrekar JN, Adkins MC. MRI findings of 26 patients with Parsonage-Turner syndrome. AJR Am J Roentgenol 2007;189:W39 –W44. 8. Baxter DE, Thigpen CM. Heel pain: operative results. Foot Ankle 1984;5:16 –25. 24. Sofka CM, Lin J, Feinberg J, Potter HG. Teres minor denervation on routine magnetic resonance imaging of the shoulder. Skeletal Radiol 2004;33:514 –518. 9. Recht MP, Grooff P, Ilaslan H, Recht HS, Sferra J, Donley BG. Selective atrophy of the abductor digiti quinti: an MRI study. AJR Am J Roentgenol 2007;189:W123–W127. 10. del Sol M, Olave E, Gabrielli C, Mandiola E, Prates JC. Innervation of the abductor digiti minimi muscle of the human foot: anatomical basis of the entrapment of the abductor digiti minimi nerve. Surg Radiol Anat 2002;24: 18 –22. 11. Delfaut EM, Demondion X, Bieganski A, Thiron MC, Mestdagh H, Cotten A. Imaging of foot and ankle nerve entrapment syndromes: from well-demonstrated to unfamiliar sites. RadioGraphics 2003;23:613– 623. 25. Cothran RL Jr, Helms C. Quadrilateral space syndrome: incidence of imaging findings in a population referred for MRI of the shoulder. AJR Am J Roentgenol 2005;184:989 –992. 26. Labib SA, Gould JS, Rodriguez-del-Rio FA, Lyman S. Heel pain triad (HPT): the combination of plantar fasciitis, posterior tibial tendon dysfunction and tarsal tunnel syndrome. Foot Ankle Int 2002;23:212–220. 27. Zanetti M, Gerber C, Hodler J. Quantitative assessment of the muscles of the rotator cuff with magnetic resonance imaging. Invest Radiol 1998;33:163–170. radiology.rsna.org ▪ Radiology: Volume 253: Number 1—October 2009