Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
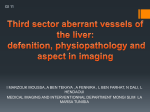
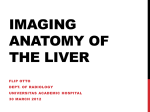
Portal venous gas from ischemic bowel disease 19 Sonographic Detection of Hepatic Portal Venous Gas Originating from Ischemic Bowel Disease: A Case Report and Literature Review Chih-Chung Chao1, Sung-Yuan Hu2,3,4,5,6, Ying-Hock Teng1,4 Hepatic portal venous gas is a rare and ominous radiological finding and it is an important diagnostic clue associated with patients who may be harboring an intra-abdominal catastrophe. Hepatic portal venous gas represents a challenge for emergency physicians in terms of diagnosis and management of the underlying cause. The most common and severest precipitating etiology is ischemic bowel disease, which has a mortality rate of 75% to 90%. Herein, we report a case of ischemic bowel disease with rare but typical hepatic portal venous gas by ultrasonography that led us to the identification of ischemic bowel disease. Key words: ischemic bowel disease, portal venous gas, ultrasonography Introduction An acute abdomen is a common and emergency condition in emergency departments (EDs). Indeed, it is necessary to investigate such a symptom immediately and treated it without delay. Hepatic portal venous gas (HPVG) is an uncommon radiological sign and often portends significant underlying intra-abdominal disease or diseases. HPVG is most commonly caused by mesenteric vascular accidents (61%-72%) and has a mortality rate of 75% to 90% (1-4). HPVG can be associated have a variety of other clinical conditions, including inflammatory bowel disease (8%-16%), intra-abdominal abscess and sepsis (6%11%), bowel obstruction and dilatation (9%-12%), gastric ulcer (3%-4%), cancer (2%-3%), iatrogenic injury and trauma (3%-4%) and being idiopathic in nature (2%) (1-5) . Most studies found in the medical literature mention computed tomography (CT) as the primary imaging tool for HPVG, but ultrasonography (US) is capable of providing real-time imaging and this can result in clues that allow clinicians to approach the underlying disease earlier. Case Report An 88 year-old man had a history of hypertension together with an old cerebrovascular accident associated with right hemiplegic sequelae; the patient was under regular medication and had Received: December 15, 2014 Accepted for publication: December 29, 2014 From the 1Department of Emergency Medicine, Chung Shan Medical University Hospital 2 Division of Clinical Toxicology, Department of Emergency Medicine 3 Center for Translational Medicine, Department of Medical Research, Taichung Veterans General Hospital 4 School of Medicine, 5Institute of Medicine, Chung Shan Medical University 6 Department of Nursing, College of Health, National Taichung University of Science and Technology, Taichung, Taiwan, ROC Address reprint requests and correspondence: Dr. Sung-Yuan Hu Division of Clinical Toxicology, Department of Emergency Medicine, Taichung Veterans General Hospital 1650 Taiwan Boulevard Section 4, Taichung 40705, Taiwan (R.O.C.) Tel: (04)23592525 ext 3670 Fax: (04)23594065 E-mail: [email protected] 20 J Emerg Crit Care Med. Vol. 25, No. 1, 2014 regular follow-up. He denied any history of surgery or trauma recently. He presented at the ED with an intermittent fever of up to about 38oC that had been present since the night previous to this ED visit. In addition, he had vomited light brown material twice and a periumbilical pain was also noted. On arrival at the ED, his vital signs were a body temperature of 37.9 oC, a blood pressure of 140/98 mmHg, a heart rate of 54 beats/min and a respiratory rate of 19 breaths/min. Physical examination revealed tenderness over periumbilical region without peritoneal signs. Laboratory investigation produced a white blood cell count of 7299/μL with 68% of neutrophils and 2% of bands, C-reaction protein level of 2.44 mg/dL, blood urea nitrogen level of 34.45 mg/dL and creatinine level of 1.1 mg/dL. Bedside US showed diffuse hyperechoic branch-like, streak-like and dotlike foci within the peripheral parenchyma of the liver, which were compatible with HPVG (Fig. 1). Based on this clue, we arranged for an abdominal CT in order to investigate the origin of the HPVG under the tentative diagnosis of IBD. The CT scan of abdomen revealed HPVG that was compatible with the bedside US findings and with IBD of the terminal ileum with pneumoatosis intestinalis and poor enhancement of the bowel loops (Fig. 2-4). The families refused surgical intervention and aggressive treatment because of the patient’s age. Unfortunately, the patient expired next day due to septic shock and multiple organ failure despite fluid replacement, treatment with a 3rd generation cephalosporin and intensive care. Discussion HPVG is an ominous but rare radiological and diagnostic sign that usually indicates the presence of serious intra-abdominal pathology that will require emergency surgery in the majority of patients. HPVG was first described by Wolfe JN in 1955 when treating six infants who died from necrotizing enterocolitis.(6) The first adult case was described by Susman N in 1960 in a patient with IBD (7). The commonest cause of HPVG is IBD. This is followed by gastrointestinal inflammation, gastrointestinal dilatation, sepsis, peptic ulcer disease, iatrogenic injury and trauma, cancer, other rare causes and being idiopathic in nature (Table 1) (1,2,4,5,8) . An early study in 1978 indicated a high Fig. 1 Bedside US revealed diffuse hyperechoic branch-like, streaklike and dot-like foci (white arrows) within the peripheral parenchyma of the patient’s liver Portal venous gas from ischemic bowel disease 21 Fig. 2 An axial view of an abdominal CT showing HPVG (white arrows) within the peripheral parenchyma of liver Fig. 3 An axial view of an abdominal CT showing ischemic bowel disease affecting the terminal ileum with pneumoatosis intesnalis and poor enhancement (white arrows) mortality rate of 75% to 90% when HPVG was detected(1,2,9). Recent studies have reported overall mortality rates of 29% to 39% when HPVG is found (4,10,11) . This apparent improvement in the survival rate can be explained by the greater use and higher sensitivity of now available diagnostic imaging modalities, such as US and CT scanning, an increased in the incidence of non-fatal causes of HPVG and the availability of adequate antibiotic therapy when treating an intra-abdominal infection. HPVG is typically identified using plain X-ray, US or CT. HPVG is predominant within the portal veins of the non-dependent left lobe and anterior right lobe(1,2,5,12,13). The first report of HPVG was described as a plain radiological sign in 1955(6). It appeared as branching radiolucencies extending 22 J Emerg Crit Care Med. Vol. 25, No. 1, 2014 Fig. 4 A coronary view of an abdominal CT showing HPVG (black arrows) and ischemic bowel disease affecting the terminal ileum with pneumoatosis intesnalis and poor enhancement (white arrow) Table 1 Causes of HPVG Acute mesenteric ischemia Gastrointestinal inflammation Diverticulitis Inflammatory bowel disease Gastrointestinal dilatation Gastric dilatation Ileus Mechanical obstruction Pseudo-obstruction Sepsis Intra-abdominal abscess Septic thrombophlebitis Peptic ulcer disease Iatrogenic injury and trauma Intraperitoneal tumor Idiopathic disease Other rare causes *Data from references 1-5 61%-72% 8%-16% 9%-12% 6%-11% 3%-4% 3%-4% 2%-3% 2% 15% Portal venous gas from ischemic bowel disease to the liver periphery. Sensitivity was increased in the left lateral decubitus view, but these findings are usually associated with a relatively late stage of the disease and require a large volume of gas to have accumulated(9). Thus HPVG on plain X-ray has been considered to be a poor prognostic sign(13,13) . On US, HPVG appears as hyperechoic dotlike, streak-like or fruit-pulp-like foci within the portal veins or liver parenchyma(1,2,8). US is a fast, low cost, and low radiation modality and also has the advantage of detecting HPVG in real time and of offering other clues as to the underlying diagnosis. US offers comparable accuracy and sensitivity to a CT scan (1,2,14) . US also offers dynamic imaging of the centrifugal flow of the portal gas to the hepatic periphery thus it can be used to differentiate this from air in the biliary tree (pneumobilia); furthermore, sensitivity is increased if color Doppler flow is used(1,2,15). As a result of the increased use and sensitivity of CT scanning, HPVG is now diagnosed more frequently. HPVG on a CT scan appears as branching lucencies within 2 cm of the liver capsule and these are predominantly present in the anterior-superior aspect of the liver’s left lobe and the hepatic periphery. HPVG must be differentiated from pneumobilia. Pneumobilia is typically visualized as a large confluence of air that is located within the central portion of the liver and this air does not extend to within 2 cm of the liver capsule. The classic description of penumobilia emphasizes a confluence of air within the common hepatic duct with branching air densities at the level of the porta hepatis with a predilection for the left lobe of liver on the CT scan because of its more ventral location(1-4,12). Both US and CT are excellent tests for detecting HPVG and CT also allows the emergency physician to determinate the underlying cause(s). The sensitivity of multi-detector CT (MDCT) in this context has been markedly increasing over time from a low of 39% to a current high of 23 82%. MDCT has a highly similar sensitivity to angiography when diagnosing IBD. Nowadays, with the development of high-resolution advanced imaging, it is possible to demonstrate potentially severe pathologies at an early stage, which opens up the possibility of prompt treatment and a significantly reduced mortality rate (1,2) . Early detection of HPVG and the identification of the underlying diagnosis have facilitated timely and targeted treatment. In addition, bedside US is able to provide real-time imaging as well as other clues that help the diagnosis. CT scan is able to detect minimal HPVG and allows determination of the precipitating etiology. A HPVG management algorithm has been proposed (12,14). The management of patients with HPVG can be divided into three groups. For the first group, urgent laparotomy is recommended when patients have clinical or radiological signs of bowel ischemia and the presence of HPVG has been detected by plain abdominal radiography; this is because previous studies have reported a mortality rate of 75% to 90% for this group(1-4). The second group consist of patients with HPVG and an equivocal clinical condition with the absence of peritonitis or bowel perforation; this patients include those with gastrointestinal inflammation, gastrointestinal dilatation, sepsis, mucosal disruption and peptic ulcer disease. They should be closely monitored with a low threshold of surgical intervention; the risk of mortality for these patients is 20% to 30%(4,9). They need to be treated with a combination of intravenous fluid, broad spectrum antibiotics, close observation and no oral intake as well as nasogastric decompression when required(2,12,14). The third group of patients with HPVG are those with non-urgent conditions or other benign causes of HPVG; these should be managed conservatively and with watchful waiting. The length of time to the disappearance of such non-urgent HPVG is very variable and can be from 24 J Emerg Crit Care Med. Vol. 25, No. 1, 2014 minutes to six weeks(16,17). These patients have a negligible risk of mortality (about 0 %)(12,14). Finally, HPVG is not a specific presentation, but it is an important diagnostic sign and clue in patients with an acute abdomen. In terms of realtime imaging capability, US can be a very valuable imaging modality when evaluating HPVG and can also provide additional clues to the emergency physician in terms of underlying diagnosis. CT is a diagnostic modality that is also able to disclose the precipitating etiology. HPVG is not by itself a surgical indication and management of HPVG depends mainly on the underlying disease. References 1.Abboud B, El Hachem J, Yazbeck T, Doumit C. Hepatic portal venous gas: physiopathology, etiology, prognosis and treatment. World J Gastroenterol 2009;15:3585-90. 2.Hussain A, Mahmood H, El-Hasani S. Portal vein gas in emergency surgery. World J Emerg Surg 2008;3:21. 3.Peloponissios N, Halkic N, Pugnale M, et al. Hepatic portal gas in adults: review of the literature and presentation of a consecutive series of 11 cases. Arch Surg 2003;138:136770. 4.Kinoshita H, Shinozaki M, Tanimura H, et al. Clinical features and management of hepatic portal venous gas: Four case reports and cumulative review of the literature. Arch Surg 2001;136:1410-4. 5. S e b a s t i à C, Q u i r o g a S, E s p i n E, B o y é R, A l v a r e z-C a s t e l l s A, A r m e n g o l M. P o r t o m e s e n t e r i c v e i n g a s: p a t h o l o g i c mechanisms, CT findings, and prognosis. Radiographics. 2000;20:1213-24. 6.Wolfe JN, Evans WA. Gas in the portal veins of the liver in infants; a roentgenographic demonstration with postmortem anatomical correlation. Am J Roentgenol Radium Ther Nucl Med 1955;74:486-8. 7.Susman N, Senturia HR. Gas embolization of the portal venous system. Am J Roentgenol Radium Ther Nucl Med 1960;83:847-50. 8.Hussain A, Mahmood H, El-Hasni S. Portal vein gas in emergency survey. World J Emerg Surg 2008;3:21. 9.Liebman PR, Patten MT, Manny J, Benfield JR, Hechtman HB. Hepatic–portal venous gas in adults: Etiology, pathophysiology and clinical significance. Ann Surg 1978;187:281-7. 10. Iannitti DA, Gregg SC, Mayo-Smith WW, Tomolonis RJ, Cioffi WG, Pricolo VE. Portal venous gas detected by computed tomography: Is surgery imperative? Dig Surg 2003;20:30615. 11. Faberman RS, Mayo-Smith WW. Outcome of 17 patients with portal venous gas detected by CT. AJR Am J Roentgenol 1997;169:1535-8. 12. Alqahtani S, Coffin CS, Burak K, Chen F, MacGregor J, Beck P. Hepatic portal venous gas: a report of two cases and a review of the epidemiology, pathogenesis, diagnosis and approach to management. Can J Gastroenterol 2007;21:309-13. 13. Schindera ST, Triller J, Vock P, Hoppe H. Detection of hepatic portal venous gas: its clinical impact and outcome. Emerg Radiol 2006;12:164-70. 14. Nelson AL, Millington TM, Sahani D, et al. Hepatic portal venous gas: the ABCs of management. Arch Surg 2009;144:575-81. 15. Yarze JC, Markowitz DM. Distinguishing between hepatic portal vein gas and pneumo(aero)bilia. Liver Transpl 2007;13:1476. 16.Griffiths DM, Gough MH. Gas in the hepatic portal veins. Br J Surg 1986;73:172-6. 17.Huurman VA, Visser LG, Steens SC, Terpstra OT, Schaapherder AF. Persistent portal venous gas. J Gastrointest Surg 2006;10:783-5. 肝門靜脈氣體由缺血性腸病變而來 25 經超音波偵測到由缺血性腸病變而來的 肝門靜脈氣體:一病例報告及文獻回顧 趙志中1 胡松原2,3,4,5,6 陳永福1,4 肝門靜脈空氣是一個罕見且預後不好的影像學發現,它對於急性腹痛的病人是一個重要的診斷線 索。肝門靜脈空氣的確切原因診斷和處置對於臨床醫師是一個挑戰。最常見及最嚴重的原因是缺血性腸 病變。在此,我們報告一例藉由超音波上罕見且典型肝門靜脈空氣影像而發現的缺血性腸病變。 關鍵詞: 缺血性腸病變,肝門靜脈氣體,超音波 收件:103年12月15日 接受刊載:103年12月29日 中山醫學大學附設醫院急診部 臺中榮民總醫院2急診部臨床毒物科 3醫學研究部轉譯醫學中心 4 中山醫學大學醫學系 5醫學研究所 6國立台中科技大學健康學院護理系 通訊及抽印本索取:胡松原醫師 40705臺中市西屯區臺灣大道四段1650號 臺中榮民總醫院急診部臨床毒物科 電話:(04)23592525轉3670 傳真:(04)23594065 E-mail: [email protected] 1