Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
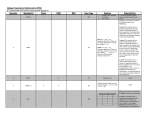
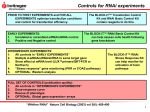
Is There a DES That Works Better for Diabetics? by Aloke Finn, MD DISCLOSURES Aloke Finn, MD Sponsored Research Grant From Boston Scientific Diabetes Mellitus: A Growing Epidemic Diabetes Mellitus affects over 100 million people worldwide Over the next 20 years there will be a 42% increase in the number of people with diabetes By 2050 almost 10% of the US population will have diabetes with the largest percentage increase among those 75 years or older Vascular disease remains by far the leading cause of mortality in patients with diabetes accounting 80% of deaths in type 2 diabetics Ischemic heart disease accounts for the majority of these deaths JAMA. 2001; 286: 1195-2000. Diabetes and Drug Eluting Stents • Given the increased risk of restenosis seen in this population, DES have become the standard of care for patients with symptomatic CAD and DM • Little is know about the vascular responses to DES in this population • It remains unknown which DES is superior in terms of intimal suppression and endothelialization in patients with diabetes Clinical Decision Making: • Choosing sirolimus or paclitaxel DES is currently based upon clinical restenosis rates yet these agents are very different in terms of their effects on the arterial wall and on intracellular signaling cascades • Both devices cause a delay in endothelialization and this is the major pathologic substrate underlying late stent thrombosis • A better understanding of the mechanisms of action by which each agent prevents restenosis is necessary to fully realize the benefits of this technology – Appropriate patient selection – Design of future anti-restenotic therapies Mechanism of Action Sirolimus Endothelial Cell PI3K PI3K Growth factors (VEGF, Insulin) mTOR migration proliferation Sirolimus mTORC1 mTORC2 S6K Akt Migration, proliferation, survival Angiogenesis and Endothelial Regrowth Sirolimus (SRL) inhibits the mTOR (mammalian target of rapamycin), which plays an important role in connecting extracellular signals with intracellular pathways critical for arterial repair. As a result the potential exists for interaction between diabetic agents which share convergent molecular signaling with mTOR pathways and sirolimus. This may have adverse effects on endothelial regrowth given both Akt and S6K are involved in endothelial cell recovery Mechanism of Action of Paclitaxel Paclitaxel binds to microtubles to prevent mitosis Prophase Anaphase Metaphase X Telophase Inhibits smooth muscle cell proliferation Inhibits neointimal hyperplasia G2 M Prevents restenosis Cell Cycle S G2 Endothelial regrowth is also inhibited M G1 The mechanism of action of paclitaxel (Ptx) involves binding to the β subunit of the tubulin heterodimer, promoting tubulin polymerization, cell cycle arrest, and, eventually, inhibition of cell migration and proliferation. Although tubulin cycling is critical for cell division, it is independent of transmission of extra-/intracellular signaling. Thus, in contrast to the effects of SRL on the diverse actions of the mTOR pathway, the action of Ptx may make it independent of these signaling mechanisms Limus versus Ptx: Differential Effects Do Occur in Patients with DM: Data From SPIRIT IV 7 P<0.001 P=ns 6 TLF (%) 5 P interaction=0.02 The effects of PES and SES are significantly different in DM versus no DM 4 3 2 1 0 EES PES No DM Stone GW TCT 2009. EES PES DM • • • • • PPAR Is a ligand-inducible nuclear transcription factor expressed in SMCs and endothelial cells PPAR agonists are commonly prescribed to type 2 diabetics— Rosiglitazone (Avandia) and Pioglitazone (Actos)--have remarkable effects on insulin sensitivity, and some studies suggest they enhance endothelialization after arterial injury. Moreover, these agents are well known to have effects on the coronary vascular wall in doses normally given to humans These agents have been reported to have effects on regulators of translational control (S6K)—thus the possibility for convergent signaling with mTOR exists mTOR itself has also been reported to be involved in control of PPAR mediated gene transcription though this has not been well explored The potential for drug interaction between PPAR agonists and sirolimus exists and its effect of endothelial regrowth remains unknown Hypothesis • To test our hypothesis that convergence of molecular signaling between oral anti-diabetic medications such as the TZD PPAR agonists and locally eluted SRL can result in significant effects on vascular healing, we examined the effect of the oral PPAR agent rosiglitazone (RSG) in combination with sirolimus-eluting (SES), Ptx-eluting (PES), or bare-metal (BMS) stents on endothelialization in the rabbit iliac model and explored the molecular mechanisms underlying the results Study Protocol SRL stent (3.0 x 18) Placebo Paclitaxel stent(3.0 x 16) Bare Metal stent (3.0 x 18) 28 day stent SRL (3.0 x 18) Rosiglitazone (3mg/kg/day) Paclitaxel stent (3.0 x 16) Bare Metal stent (3.0 x 18) endothelialization or 14 day organ culture/western blot Bare Metal Stent Placebo *p=0.01 vs. CypherPlacebo +RSG Sirolimus-Eluting Stent Placebo +RSG Paclitaxel-Eluting Stent Placebo +RSG Group Endothelial Strut Coverage (%) Uncovered Strut Area (mm2) Cypher-Placebo 42.50±16.33 4.43±0.80 Cypher-Rosiglitazone 18.57±5.89* 5.69±0.27* Bare Metal-Placebo 87.70±19.29 1.25±1.91 Bare Metal-Rosiglitazone 90.85±15.40 1.03±1.76 Taxus-Placebo 87.37±8.16 1.64±1.13 Taxus-Rosiglitazone 80.53±24.5 2.42±3.11 Finn AV et al. Circ Research. 2009. 14 Day Organ Culture for VEGF A. B. 2 P=0.05 Relative VEGF levels (% of control ( placebo)) Relative VEGF levels (% of control ( placebo)) 1.2 1 0.8 0.6 0.4 0.2 0 SES-Placebo SES-RSG P=0.007 1.5 1 0.5 0 BMS-Placebo Group Group 2.5 Relative VEGF levels (% of control ( placebo)) C. 2 BMS-RSG D. P=0.05 1.5 1 0.5 0 PES-Placebo PES-RSG Group Group Ratio Comparisons Abs. dif. 95% CI P value BMS vs. SES 0.84 0.41,1.58 0.003 PES vs. SES 0.99 0.43,1.55 0.008 BMS vs. PES 0.15 -0.40,0.71 0.55 8 Fold increase in VEGF Transcript Fold increase in VEGF Transcript A. P=0.002 P=0.0002 B. 6 P=0.0001 4 P=0.01 2 0 0 0.001 0.01 0.1 1 10 25 50 75 100 3 2 1 DMSO (N= 4 experiments/group) D. P=0.002 7 Fold increase in VEGF Transcript Fold increase in VEGF Transcript C. 6 5 4 3 2 1 0 DMSO Ptx RSG (N= 4 experiments/group) SRL RSG SRL/RSG (N= 4 experiments/group) P=0.001 8 P=0.0007 4 0 Rosiglitazone Concentration (uM) p<0.0001 5 Ptx/RSG 8 7 P=0.02 P=0.02 6 5 4 3 2 1 0 Scr siRNA DMSO Scr siRNA PPAR siRNA RSG DMSO (N= 4 experiments/group) PPAR siRNA RSG P=0.001 1.5 P=0.001 1 0.5 0 DMSO SRL RSG 4 3 P=0.006 2.5 2 P<0.0001 1.5 1 0.5 Scr shRNA RSG DMSO (N= 4 experiments/group) D Input (negative primer) Input (positive primer) IP-PPARγ (negative primer) Relative gene transcript DMSO RSG SRL SRL+RSG 14 10 * VEGF HO-1 8 6 4 2 10 * *,# ! 8 * VEGF HO-1 6 *,! 4 2 *.# ** *,# 0 0 (N= 3 experiments/group) mTORshRNA mTOR shRNA DMSO RSG (N= 4 experiments/group) 12 IP-PPARγ (positive primer) P=0.02 0 Scr shRNA SRL+RSG C P=0.0 4 3.5 Relative gene transcript 2 B P=0.002 P=0.01 Relative HO-1 gene transcript Relative HO-1 gene transcript A Scr siRNA p70 siRNA Scr siRNA p70 siRNA DMSO DMSO RSG RSG N= 4 experiments/ group *p<0.05 versus Scr siRNA DMSO and siRNA p70s6k DMSO #p<0.05 versus p70 siRNA RSG !p=0.09 versus Scr siRNA DMSO Scr siRNA Akt2 siRNA Scr siRNA Akt2 siRNA DMSO DMSO RSG RSG N= 4 experiments/ group *p<0.05 versus Scr siRNA DMSO and siRNA p70s6k DMSO #p<0.05 versus Scr siRNA RSG !p<0.05 versus Akt2 siRNA DMSO And Akt2 siRNA RSG **p<0.05 versus Scr siRNA DMSO VEGF Receptor PI 3 kinase Endothelial Cell mTORC2 Sirolimus PDK-1 Akt mTORC1 Rosiglitazone 4EPB1 p70S6K ? Downstream mediator eIF4E Translation S6 DNA Cell Growth HIF-1α VEGF transcription PPAR-mediated transcription Nucleus VEGF/HO-1 Conclusions • mTOR signaling is best known for its role in translational regulation via two downstream effectors, S6K1 and 4E-BP1 • In this study we reveal that mTOR also interacts with PPARγ likely through control of transcriptional regulation • This interaction has important consequences for patients receiving sirolimus (and its analogues?) DES who are also taking oral PPAR agents (rosiglitazone and pioglitazone) in that it results in further delay of vascular healing of the vessel wall • Do other commonly used diabetic agents also share convergence with sirolimus/mTOR (i.e. insulin, metformin)and how does this affect healing? Clinical Data Numerous studies have shown diabetes to be an independent predictor of late stent thrombosis after DES (Iacovou JAMA 2005, Daemen J Lancet 2007) Meta-analysis of 4 pivotal randomized trials with sirolimus stent (SES) has shown significantly increased cardiac death, Q wave MI, and late stent thrombosis in patients w/ DM treated with SES versus BMS but with significantly reduced TLR (Caixeta A et al. JACC 2009.) Meta-analysis of 5 randomized trials of paclitaxel eluting stents (PES) demonstrated significantly reduced TLR with no differences in death, MI or stent thrombosis in DM patients treated with PES versus BMS (Kirtane AJ et al. JACC 2008) Paucity of data exists on the vascular responses to stents in diabetic models despite the routine use of these devices in patients with DM Long term data from diabetic only randomized trials are lacking Indeed use of DES in patients with DM is considered “off-label” Conclusion • Mechanisms of action of different DES may have important clinical consequences in patients with DM • Considerable overlap exists between mTOR signaling and many meds used to treat DM but the effect of these interacts remains unknown • Diabetic patients talking TZD in combination with SES may be at risk for delayed stent healing • Further work needs to be done in both clinical and basic realms to improve outcomes in patients with diabetes after PCI Sirolimus (500 nM) Rosiglitazone (100 uM) - + - + p-Akt B + + p-Akt Akt p-p70s6k p70s6k 1.5 + + + + - + + D p-p70s6k p70s6k p-Akt 0 - HIF-1α p-p70s6k p-Akt β-Actin (N= 4 arteries/group) SRL/RSG + F DMSO SRL 2 0.8 1.5 0.6 1 0.4 0.5 0.2 0 2 SRL/RSG P=0.04 P=0.03 1 RSG p-p70s6k 1.2 2.5 Relative Phosphorylation + RSG 0 DMSO DMSO RSG RSG Scr siRNA PPAR siRNA Scr siRNA PPAR siRNA Bare Metal Stent Sirolimus Stent - SRL p-Akt 3 (N=4 experiments/group) RSG P=0.002 0.5 Akt E P=0.002 DMSO Relative Phosphorylation C + + - P=0.0002 1.2 P<0.0001 P=0.004 1 P=0.04 0.8 0.6 0.4 0.2 0 1 (N=4 experiments/group) Scr siRNA PPARγ siRNA DMSO RSG p-p70s6k P=0.001 Relative Phosphorylation A . P=0.02 P=0.01 P=0.01 DMSO RSG RSG DMSO Scr siRNA PPAR siRNA Scr siRNA PPAR siRNA p-p70s6k p-Akt HIF-1 * 1.5 1 * * * * ** 0.5 0 *, # *,# *P<0.05 versus BMS #P<0.05 versus BMS-RSG and SES BMS BMS-RSG SES Group SES-RSG