Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
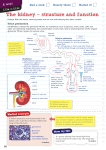
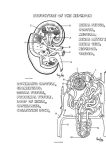
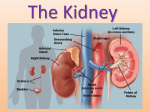
Renal Structure and Function Introduction •Main function of kidney is excretion of waste products (urea, uric acid, creatinine, etc). Other excretory organs are ? •As above function is fulfilled, kidney also extremely important in maintaining –fluid and electrolyte homeostasis –volume of the extracellular fluid volume –Acid-base balance –Blood pressure Functional Background •Kidneys receive ≈ ¼ of total cardiac output even though small lots of capillaries •Filter about 11X the extracellular fluid volume/d. from plasma •Produce ≈ 180 liters/d. of filtrate •Filtrate very similar to plasma except very little protein (protein in urine = serious problem) •99% reabsorbed as pass through renal tubule •Some substances secreted into renal tubule •Approximately 1.5 liters/d. of filtrate is voided as urine Gross Anatomy of the Kidney •Each kidney consists of –an outer cortex –Inner medulla –Hollow pelvis empties into ureter –Functional unit of the kidney is the nephron (≈ 1,300,000 nephrons per kidney) Structure of the Nephron • Nephron – Glomerulus • Bowman’s capsule, Bowman’s space – Proximal convoluted tubule – Loop of Henle • Descending limb • Ascending limb – Distal convoluted tubule – Collecting duct Diagram of nephron structure Flow of filtrate Function of the Nephron: Glomerulus –Site of filtration –Each glomerulus consists of a capillary network surrounded membrane called Bowman's capsule. –Afferent arteriole carries blood from renal artery into glomerulular capillaries –At distal end of glomerulus, capillaries form the efferent arteriole through which blood leaves the glomerulus. Glomerular Filtration • Fluid driven from the glomerular capillaries into Bowman’s capsule by hydrodynamic force (blood pressure) Note: as blood pressure increases, volume of filtrate increases more filtrate formed = less blood volume = lowered blood pressure • Fluid crosses three layers that excludes large molecules (especially proteins) • Blood which passes on through to efferent arteriole is thus high in protein plasma and thus a higher oncotic pressure than normal Note: oncotic pressure = osmotic pressure contributed by large molecules such as plasma proteins Function of the Nephron: Proximal Convoluted Tubule • Epithelium is “leaky” allows passive movement of some ions (Na+, Cl-, glucose, amino acids, HCO3-) and water out of tubule • 60-70% of filtered load reabsorbed in proximal tubule • Transport mechanisms (Na+/H+ exchanger moves Na+ out of proximal tubule, water follows; some Na+ is coupled to other solutes (glucose, amino acids) • Remaining 30-40% of filtrate, which is still isosmotic with plasma, passes on to the loop of Henle Function of the Nephron: loop of Henle • Consists of a descending and ascending portion (which has both thin and thick segments) • Descending portion high permeability to water allows leakage into tubular interstitium • Increased oncotic pressure in peritubular capillaries (coming from efferent arteriole) helps move water from tubular interstitium back into capillaries filtrate becomes concentrated • Ascending portion active reabsorption of NaCl, absorbs 20-30% of the Na+ in the tubule • Reabsorption occurs by transport mechanism driven catalyzed by Na+/K+-ATPase • Volume of filtrate reduced by additional 5% • Because NaCl is reabsorped filtrate becomes hypotonic to plasma as enters distal convoluted tubule Water and NaCl reabsorption in the loop of Henle Function of the Nephron: Distal Convoluted Tubule • Active NaCl out of filtrate continues • Active secretion of K+ (depending on blood levels) and H+ (depending on pH) into filtrate, driven by a Na+/K+ pump • Regulation of Ca++ occurs here • As filtrate leaves DCT it is isoosmotic with plasma • Enters collecting tubule/collecting duct Function of the Nephron: Collecting Tubule and Collecting Duct – Several distal tubules empty into each collecting tubule; they join to form the collecting duct – Collecting duct: NaCl, K+ and water reabsorption – NaCl reabsorption, K+ secretion under control of aldosterone – Water under control of ADH – Some H+ secretion occurs – End result highly concentrated urine (mammals and birds only animals able to do so) elimnates waste using as little water as possible Aldosterone • Has a threefold action on Na+ reabsorption 1. 2. 3. Rapid effect by stimulation of an Na+/H+ exchanger containing an aldosterone receptor Delayed effect by binding to intracellular receptors that direct synthesis of a mediator protein that activates sodium channels Long-term effect by increasing the number of basolateral Na+ pumps Review of reabsorption and secretion in the nephron Natriuretic peptides •Involved with regulation of Na+ excretion in distal tubule •Release from heart atria when arterial pressure is too high •Causes water and salt diuresis by kidney, reducing blood volume and eventually atrial pressure Acid-Base Balance • Kidney’s help regulate H+ and bicarbonate • Urine can be basic or acidic depending on need • Usually acidic to compensate for tendency of blood pH to drop due to presence of CO2 (which forms carbonic acid via carbonic anhydrase-catalyzed reactions) • Compensating mechanism is secretion of H+ into tubular fluid and reabsorption of bicarbonate Potassium Balance • Rapidly and narrowly regulated by kidney • Regulation important because small changes in K+ levels can affect function of many excitable tissues (heart, brain, skeletal muscle • Most filtered K+ is reabsorbed in proximal tubule and loop of Henle • Most secretion of excess K+ occurs in collecting tubule The End