Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
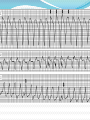
MEHDI BAKHSHI MSN,CCN PHD CANDIDATE 1 2 3 V3 Importance of diagnosis of WCT -Correct diagnosis is important both for acute management and also subsequent management. -If we inject verapamil to a patient with VT and low EF , prolonged hypotension and hemodynamic deterioration happens. -Non of the criteria is perfect but they can be helpful. -The clinical situation of the patient with WCT usually don’t allow leisurely analysis of ECG ,so the criteria must be not only accurate but easily applied and easily remembered. Definitions -WCT :Rate equal or more than 100 and QRS duration of at least 120 msec. -VT :a WCT originating below the level of His bundle. -SVT : a tachycardia dependent on participation of structures at or above the level of His bundle. -LBBB morphology: QRS duration more than 120 with predominantly negative terminal deflection in V1. -RBBB morphology : QRS duration more than 120 and a terminal positive deflection in V1. -LBBB and RBBB morphology denote the appearance of QRS , without implying actual His-Purkinje disease. Top 10 reasons for WCT* 1. Ventricular 6. VT Tachycardia 2. Ventricular Tach 3. VT 4. VT 5. VT 7. VT 8. VT 9. SVT with preexisting BBB 10. SVT with aberrant conduction * Ken Grauer. A Practical Guide to ECG Interpretation. 2nd Diagnostic methods 12-lead electrocardiogram ! ! ! Post-op atrial/ventricular pacing wires Esophageal pacing leads Adenosine can be diagnostic Invasive electrophysiology study Diagnostic methods Always Always Always record a rhythm strip during any intervention (adenosine, cardioversion, Valsalva, etc.) Differential Diagnosis of WCT -Ventricular tachycardia (about 80% of cases ). -SVT with abnormal interventricular conduction (15-20 %): *SVT with BBB aberration (fixed or functional). *Pre-excited SVT (SVT with ventricular activation occurring over an anomalous AV connection ).Their ECG can be indistinguishable from VT originating at the base of ventricle.(15 % of all) *SVT with wide QRS due to abnormal muscle-muscle spread of impulse.( surgery, DCM) *SVT with wide complex due to drug or electrolyte-induced changes. (hyperkalemia. Class Ia ,Ic drugs or Amiodarone) -Ventricular paced rhythms .(small but growing percentage ) 1. VT is more common than SVT with aberrancy 2. In patients with structural heart disease, particularly prior infarction, VT is much, much more common than SVT with aberrancy 3. If SVT is misdiagnosed as VT for the purposes of acute treatment, no harm will come to the patient 4. If VT is misdiagnosed as SVT for the purposes of acute treatment, a cardiac arrest can be precipitated SVT vs VT History -The majority of patients with VT have structural heart disease, In SVT they may or may not have. -Patient with VT are older. -Patients with SVT more often have history of previous similar episodes .(cutoff of 3 years) Factors Favoring VT Concordance across all V leads (+/-) ERAD axis deviation QRS > .16 sec AV dissociation Suggestive QRS morphology SVT vs VT ECG criteria -A fundamentally simple approach: If WCT is due to SVT with aberration, the QRS must be compatible with some form of BBB or FB. -QRS duration:70% of VTs have QRS duration >140, but no SVT has it. VT is probable when QRS> 140 with RBBB and >160 with LBBB pattern.Anti arrhythmic drugs may prolong QRS. Some patients with VT may have QRS of 120-140 specially in those without structural heart disease. SVT vs VT ECG criteria contd, -QRS axis: *The more leftward the axis , the more probable VT. * The quadrant between -90 and 180 (northwest )can’t be achieved with any combination of FB or BBB. *Some has suggested that if the axis in sinus rhythm is more than 40 degrees different with WCT the diagnosis is VT , but it is not widely accepted. SVT vs VT ECG criteria contd -Specific morphologies ; If with RBBB pattern: *In V1:During aberration there is no change in initial portion of QRS so we may see rSr’ ,rR’ , rsr’ or rSR’. But a monophasic R wave , or a broad (> 30 msec) R with any following terminal QRS forces or qR are highly suggestive of VT. * In V6 :During aberration qRs , Rs ,or RS (with R/S ratio >1) are seen but in VT we may see rS,Qrs , QS or QR or monophasic R wave. If RS pattern is present R/S must be less than 1. SVT vs VT ECG criteria contd LBBB pattern: * In V1 :Either rS or QS with rapid initial forces (narrow R with rapid smooth descent to S )is seen in LBBB type aberration. Any other pattern such as broad R/deep S or QS with slow descent to S wave nadir will imply VT. If the initial R is wider than 30 msec it suggest VT , the wider the R , the greater the likelihood of VT. Notching in the down-stroke of S or interval from the onset of QRS to the S wave nadir greater than 60 msec strongly suggest VT. *In V6 :In aberrancy there is no initial Q wave and we see RR’, or monophasic R. During VT common patterns are QR ,QS ,QrS ,or Rr’ although patterns compatible with SVT may also be seen. SVT vs VT ECG criteria contd Combination of LBBB and RAD is almost always due to VT . RBBB with a normal axis is very uncommon in VT. Concordant pattern in precordial leads is uncommon in SVT ,with the exception of preexcited tachycardia .The specificity of concordant pattern for VT is >90% but sensitivity is low(20%). Negative concordance in limb leads is another way of describing NW axis and suggests VT. QRS duration > 140 ms Concordant pattern in all precordial leads Absence of RS complex in all precordial leads R-to-S interval >100 ms in one precordial lead SVT vs VT ECG criteria contd Q waves during WCT show old MI and are in favor of VT. Generally patients with old Q waves maintain it during WCT . Some patients with DCM may have Q during VT while they don’t show it in SR. Pseudo Q waves may be seen in some SVTs with aberrancy. (AVNRT or pre-excited with a posterior AV connection ). AV Dissociation AV dissociation Is the most useful criteria. Complete AVD is seen in 20-50% of all VTs and practically no SVTs. (specificity near 1) 15-20 %of VTs have second degree VA block. Another clue to the presence of AVD is variation in QRS amplitude. (summation of p on QRS or variable ventricular filling). 30% of VTs have 1:1 retrograde conduction. Faster VTs are less likely to have 1:1 conduction but there is no cut-off. Carotid pressure or adenosine can cause transient VA block and show VT. Fusion beats imply the presence of AVD (most often seen during slow tachycardias). It is most reliable when it is a clear fusion and not a simply change in morphology. Which can be due to PVC during VT. PVCs can fuse with SVT beats which can erroneously be taken as VT. Narrow QRS complex VT VT can have QRS duration less than the cutoff of 140 msec. Possible explanations are: 1-Septal origin of VT. 2- Early penetration in the His- Purkinje system. Atrial Fibrillation with Rapid Conduction Via Accessory Pathway Antidromic AVRT AF +WPW Sustained Aberrant Conduction V1 Polymorphic VT V1 “Torsade de Pointes” (Polymorphic VT Associated with Prolonged Repolarization) Sustained VT: Degeneration to VF Atrial Fibrillation with Rapid Conduction Via Accessory Pathway: Degeneration to VF Regular Wide QRS Tachycardia: VT or SVT with Aberrant Conduction? More R-Waves Than P-Waves Implies VT! II Artifact Mimicking “Ventricular Tachycardia” QRS complexes “march through” the pseudo-tachyarrhythmia Artifact precedes “VT” 1 2 3 V3