Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
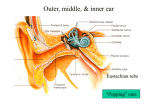
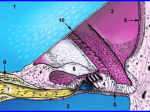
HEARING NOTES WCR May 2015 Marieb & Hoehn chapter 15; Martini & Ober chapter 15 Structure of Ear External (outer), middle, internal (inner): External. Includes auricle=pinna, external auditory meatus (or canal). End with eardrum = tympanic membrane. Middle. Normally air-filled. Malleus, incus, stapes (in that order). Stapedius & tensor tympani muscles. Pharyngotympanic tube connect middle ear to pharynx (throat). Which bone is attached to eardrum? Which to oval window? Oval window = portal at which sound moves from middle to inner ear. Internal. In cavities in temporal bone. Includes vestibule, semicircular canals, and cochlea. Of these, only cochlea involved with hearing. o Cochlear anatomy. Cochlea is a coiled structure with 3 chambers or ducts (scalae) running along its length: vestibular duct (scala vestibuli, connects to oval window), tympanic duct (scala tympani, connects to round window, which is a membrane covered opening between middle and inner ear), and most importantly the cochlear duct (scala media). Vestibular & tympanic ducts filled with perilymph and connect to one another at helicotrema, the connecting hole between them at apex of cochlea. Spiral ganglion spirals around the axis of cochlea and contains cell bodies of the neurons whose fibers come from organ of Corti (see next). Nerve fibers join to make cochlear nerve which joins cranial nerve VIII. o Cochlear duct (scala media) contains the spiral organ of Corti. Organ of Corti = basilar membrane, inner & outer hair cells, overlying tectorial membrane, and nerve fibers going to/from the outer/inner hair cells. Cochlear duct filled with endolymph (not perilymph). Physiology of Hearing Sound Sound = pressure disturbance. A “pure tone” is a sinusoidal wave with a frequency (also known as pitch – what musical note is it?) and an intensity or amplitude, which we perceive as loudness. Frequency measured in Hertz=cycles/second. Intensity measured in decibels (dB). Real world sounds are a mix of many frequencies, each of which has its own intensity. Be able to distinguish between 2 traces that differ in frequency but have same amplitude, or vice versa, and be able to identify which trace has a high pitch versus low pitch, or high amplitude versus low amplitude. (Fig 15.8 #2 in Visual A&P; Fig 15.30 in Marieb & Hoehn 8th ed., Fig 15.29 in Marieb & Hoehn 9th ed.) Sound transmission to inner ear Sound enters external ear canal, makes tympanic membrane vibrate, makes malleus, incus, stapes vibrate. Stapes footplate in oval window causes pressure waves in the inner ear fluid which travel quickly down the vestibular duct. Basilar membrane (BM) resonance. BM is narrow and stiff near base of cochlea (near oval window). Narrow & stiff means its natural frequency of vibration is high. BM gets wider & less stiff with greater distance along cochlea, so BM at far end has a low natural frequency of vibration. Incoming sound waves in the fluid cause vibration of the BM with a corresponding natural frequency: high pitched sounds make BM near base vibrate. Low pitch sounds make BM at far end vibrate. Hair cell excitation One row inner hair cells, 3 rows outer hair cells. All hair cells have stereocilia (“hairs”) sticking out of their tops (apical ends) into the endolymph-filled space between hair cells & tectorial membrane. Afferent nerve fibers connect to basal end of hair cells. Incoming sound causes BM vibration causes stereocilia movement. Stereocilia mechanically linked to ion channels. When stereocilia move back/forth, ion channels open/close, cause cell membrane voltage to get more positive/negative, causing more/less release of excitatory neurotransmitter onto nerve fibers at base of hair cells. Most afferent nerve fibers are from inner hair cells. Outer hair cells receive some efferent innervation and affect local mechanical responsiveness (hence sensitivity) of BM. Auditory pathway to brain Hair cell depolarization releases glutamate from hair cell onto afferent fiber, exciting it. Nerve fibers from hair cells pass through spiral ganglion (where cell bodies are), merge to form cochlear nerve, then join nerves from semicircular canals & vestibule to make cranial nerve VIII. Afferents synapse in cochlear nucleus (medulla). Pathway leads eventually to medial geniculate nucleus of thalamus. Thalamic MGN neuron axons go to primary auditory cortex (temporal lobe) which gives rise to conscious awareness. Most but not all fibers go to opposite side of cortex. Tonotopic mapping (different frequencies excite neurons in different places) is found at multiple levels of processing, from organ of Corti to cochlear nucleus to primary auditory cortex. Auditory processing Pitch perception: Based on which hair cells are activated. Basal end fibers (close to oval window) = high pitch, apical end fibers = low pitch. Complex sounds have many component frequencies. Loudness perception: Based on frequency of nerve impulses on a given fiber, and how many fibers are activated. Louder sound causes more frequent action potentials and more fibers recruited. Direction perception: Done by detecting differences in the intensity and timing of sounds arriving at R & L ears. Homeostatic Imbalances of Hearing Deafness Conduction deafness: Sound not conducted from outside world to the hair cells. Causes include impacted earwax, perforated eardrum, otitis media, otosclerosis (ossicles don’t articulate freely). Sensorineural deafness: Problem with the hair cells or with nerves from ear to brain. Causes include loss of hair cell stereocilia due to aging, exposure to loud sounds, infection, some drugs, or genetic mutation (congenital deafness). Cochlear implants are a treatment for sensorineural deafness caused by hair cell absence or loss.