Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
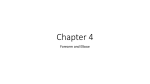
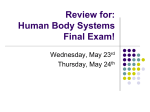
Techniques in Shoulder and Elbow Surgery 7(1):72–76, 2006 Ó 2006 Lippincott Williams & Wilkins, Philadelphia R E V I E W m m Anterior Elbow Capsulodesis Donald H. Lee, MD, Douglas R. Weikert, and Jeffry T. Watson Department of Orthopaedic Surgery Vanderbilt Orthopaedic Institute Nashville, TN m ABSTRACT The technique and role of an anterior elbow capsulodesis in restoring elbow instability following an unstable elbow fracture-dislocation are described. Six patients with an unstable posterior elbow fracture-dislocation were retrospectively reviewed. The average age of the patients was 45.5 years. Five of the 6 patients had a type I coronoid fracture, and 5 patients had a radial head fracture. All patients had an associated posterior dislocation of the elbow. Two patients had previous surgery. All patients underwent elbow reconstruction with restoration of the ulnohumeral joint and lateral collateral ligament complex repair. Five patients had a radial head replacement. An anterior elbow capsulodesis was performed in all patients for residual, postreconstruction, posterior elbow instability. A hinged fixator was used in 1 patient. At an average follow-up of 19 months (range, 6Y33 months), all patients had a stable elbow. The average extension-flexion arc was 26 to 133 degrees. Pronation and supination averaged 54 and 69 degrees, respectively. Conclusion: A stable elbow joint can be achieved by restoring ulnohumeral joint congruency, repairing the lateral collateral ligament complex, and repairing or replacing an injured radial head. An anterior elbow capsulodesis is used when further stabilization of residual posterior elbow instability is needed. Keywords: elbow, complex elbow fracture-dislocations, anterior elbow capsule, capsulodesis m INTRODUCTION Complex elbow fracture-dislocations often occur with a similar pattern of injury. Axial compression of the forearm in combination with forearm supination and a valgus load on the elbow, as seen with a fall on an outstretched arm, produces a common posterior elbow fracture-dislocation pattern.1Y8 An injury pattern, starting laterally and extending medially, is seen. Identifying the Address correspondence and reprint requests to Donald H. Lee, MD, Department of Orthopaedic Surgery, Vanderbilt Orthopaedic Institute, Medical Center East, South Tower, Suite 3200, Nashville, TN. E-mail: [email protected]. 72 pattern and components of a complex elbow fracturedislocation allows for the use of a treatment algorithm. The purpose of this study is to retrospectively review the results of an anterior capsulodesis or repair of an avulsed anterior capsule to the coronoid process and its role in stabilizing the unstable elbow during reconstruction of a posterior elbow fracture-dislocation. m MATERIALS AND METHODS Following an institutional review board approval, 7 patients with a complex elbow fracture-dislocation were retrospectively reviewed. There were 6 men and 1 woman (Table 1). One male patient was lost to follow-up at 2 months, leaving 6 patients for review. The average age of the patients was 45.5 years (range, 21Y77 years). The right dominant elbow was involved in 2 patients and the left elbow in 4 patients. Two patients had a concomitant fracture of the distal radius and a patient with a fracture of the distal ulna. Five of the 6 patients had a type I coronoid fracture.9 All patients were noted to have a distal avulsion of the anterior joint capsule off the coronoid process. Two patients had undergone previous surgery: one elbow open reduction and internal fixation (ORIF) of a comminuted proximal ulnar fracture with iliac crest bone grafting and internal fixation of a comminuted radial head fracture. A second patient had internal fixation of a proximal ulnar fracture. The indications for surgery included a complex posterior elbow fracture-dislocation with a displaced proximal ulnar and/or radial head/neck fracture, persistent posterior elbow joint instability following joint reconstruction, and intraarticular loose bodies. Two patients had a displaced proximal ulnar fracture. Five patients had a radial head/neck fracture. Five patients had a type 1 coronoid fracture. The indication for an anterior elbow capsulodesis (suture capsulorraphy of the anterior joint capsule to the coronoid process) was residual posterior elbow instability following reconstruction of the ulnohumeral joint and the lateral column structures (radial head and lateral collateral ligament complex). Reconstructive surgery included ORIF of a proximal ulnar fracture (2 patients) or reduction of a dislocated ulnohumeral joint (4 patients), repair of the lateral Techniques in Shoulder and Elbow Surgery Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Anterior Elbow Capsulodesis TABLE 1. Demographics Age (y) Type of injury Previous surgery Radial head fracture 1 2 77 21 Fall Fall Yes Yes 3 4 5 6 41 29 44 61 Fall MCA Fall MCA No ORIF ulna/ RH No No No ORIF ulna Patient Average Yes No Yes Yes 45.5 RH, radial head; MCA, motorcycle accident. collateral ligament complex (all patients), and radial head replacement (5 patients). All patients had persistent posterior elbow joint instability following reconstructive surgery when examined under intraoperative fluoroscopy. One patient who had underwent repeat surgery 3 weeks after previous ORIF of a proximal ulnar and radial head fractures had placement of a hinged external fixator. Operative Technique Reconstructive surgery should include (1) the use an extended posterolateral Kocher approach with a posterior midline incision or lateral incision, (2) ORIF of a proximal ulnar fracture, including a coronoid fracture, if present and fixable, (3) repair or metallic radial head replacement of a radial head/neck fracture, if present, (4) repair of the lateral collateral ligament complex using a transosseous suture technique, (5) use of intraoperative fluoroscopy to test for residual posterior elbow stability, (6) use of an anterior elbow capsulodesis, if persistent posterior instability is noted, and (7) use of a hinged external fixator for additional stability or to protect repaired structures, if needed. tion plate or dynamic compression plate. Type 2 or 3 coronoid fractures are repaired using screw or small plate fixation with or without incorporation of the screw into the proximal ulnar plate. Type 1 coronoid fractures are left alone, if following reconstruction of the proximal ulnar fracture or following reduction of the ulnohumeral joint; the joint remains stable in extension. Repair or Replace a Radial Head/Neck Fracture. An ORIF of repairable radial head and/or neck fracture is performed if stable fixation is obtainable. Severely comminuted radial head and/or neck fractures not amenable to internal fixation should undergo a metallic radial head replacement. Use a Transosseous Suture Technique to Repair the Lateral Collateral Ligament Complex. Two drill holes are place in an anterior to posterior direction through the lateral epicondyle. In the sagittal plane, a hole is placed slightly superior and one slightly inferior to the distal humeral central axis of rotation. Two, no. 2, nonabsorbable braided sutures are weaved through the proximal lateral collateral ligament complex using a grasping suture technique. The sutures are then placed through epicondylar bone holes in an anterior to posterior direction using a suture passer (Fig. 1). The avulsed lateral collateral ligament complex is reapproximated to its origin by tensioning but not tying the sutures. Use Intraoperative Fluoroscopy to Determine Elbow Stability. After the lateral collateral ligament complex is reapproximated to its insertion site, the ulnohumeral and radiocapitellar joints are passively ranged and visualized with intraoperative fluoroscopy. The elbow is flexed and especially extended, observing for signs of Key Surgical Points Use an Extended Posterolateral (Kocher) Approach. A posterior or posterolateral longitudinal incision is used. An extended posterolateral or Kocher approach between the anconeus and the extensor carpi ulnaris is developed. The dissection is carried proximally along the lateral supracondylar ridge. The lateral collateral ligament complex is usually partially or completely avulsed from its proximal insertion onto the lateral epicondyle. The dissection is continued superiorly along the supracondylar ridge and extended anteriorly and medially along the distal humerus. The radial head and coronoid process are visualized. The anconeus can be elevated subperiosteally to expose the proximal ulna, if needed, for internal fixation of a proximal ulnar fracture. Repair the Proximal Ulna if a Proximal Ulnar Fracture is Present. An open reduction of the proximal ulna is performed by preferably using a precontoured commercially available plate or a contoured pelvic reconstruc- FIGURE 1. Illustration of the repair of the lateral collateral ligament complex using nonabsorbable sutures placed through transosseous lateral epicondylar suture holes. The holes are placed at the level of the distal humeral central axis of rotation. Volume 7, Issue 1 Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 73 Lee et al through each drill hole from an anterior to posterior direction through the ulna. With the elbow flexed, the sutures are tied along the subcutaneous border of the ulna. Following repair of the anterior joint capsule and with tensioning of the lateral collateral ligament sutures, the elbow is then reexamined under fluoroscopy to note if ulnohumeral joint stability is restored (Fig. 3). Use a Hinged External Fixator if Needed. The main indications for a hinged external fixator are to stabilize a grossly unstable elbow, a chronically unstable or dislocated elbow, and to protect bone fixation or ligament repair. In general, hinged external fixator is not needed. The options for the fixator include a preferred unilateral or monolateral hinged fixator or a semicircular hinged fixator. m FIGURE 2. Illustration of the repair of the anterior elbow joint capsule using nonabsorbable sutures placed through transosseous proximal ulnar suture holes. The suture holes are placed so that the anterior capsule, when repaired, forms a congruent articular surface with the anterior portion of the greater sigmoid notch. posterior ulnohumeral joint instability. Forearm rotation, particularly supination in combination with elbow extension, is observed for signs of posterolateral instability of the radial head. If residual posterior ulnohumeral joint instability with elbow extension is noted, an anterior elbow capsulodesis is performed (see below). If residual posterolateral radiocapitellar joint instability is noted, an additional suture hole can be placed more proximally, and the ligament repair is shifted superiorly. Restore Stability of the Ulnohumeral Joint Using an Anterior Elbow Capsulodesis. A grasping Bunnell-type suture using two, no. 2, nonabsorbable braided sutures is placed into the anterior elbow joint capsule. The joint capsule is usually avulsed off its distal insertion. A portion of the brachialis can be incorporated into the repair if needed to reinforce the repair. Two drill holes are placed into the base of the coronoid fracture. Two converging drill holes are placed from the subcutaneous border of the ulna toward the coronoid process fracture site. Care is taken to insure that the drill holes exit at the proximal edge of the coronoid fracture immediately adjacent to the greater sigmoid notch articular surface. The suture holes are positioned in this manner to insure that the anterior capsule, when repaired, forms a congruent articular surface with the anterior portion of the greater sigmoid notch (Fig. 2). Two sutures strands are passed 74 RESULTS The average follow-up was 19 months (range, 6Y33 months; Table 2). The final range of motion was 26 degrees of elbow extension (range, 10Y40 degrees), 133 degrees of elbow flexion (range, 125Y140 degrees), 54 degrees of forearm pronation (range, 40Y75 degrees), and 69 degrees forearm supination (range, 40Y85 degrees). The ulnohumeral and radiocapitellar joints were radiographically congruent. There was no clinical evidence of varus, valgus, or posterolateral instability in any patient. m DISCUSSION Elbow joint stability is the result of the combination of osseous structures (ulnohumeral and radiocapitellar joints) and soft tissue restraints (collateral ligaments and anterior and posterior capsules).3,10Y13 Complex elbow fracture-dislocations frequently occur with a similar pattern of injury. The injury usually starts laterally and extends medially.3Y8 Following avulsion of the lateral collateral ligament complex off its insertion onto the lateral epicondyle, disruption of the anterior and posterior capsule occurs. The anterior capsule is usually avulsed off its insertion onto the coronoid process.14,15 Subluxation and subsequent dislocation of the radiocapitellar and ulnohumeral joint then occur. Finally, disruption of the medial collateral ligament occurs as the elbow fully dislocates. Elbow dislocations can occur with only soft tissue (collateral ligaments and joint capsule) injuries or with associated fractures (radial head and/or neck, coronoid process, proximal ulna, and distal humerus). An elbow dislocation associated with a radial head/neck fracture and coronoid fracture produces a particularly unstable fracture-dislocation pattern.1Y3,5Y7 The coronoid process working in conjunction with the radial head is recognized as an important stabilizer Techniques in Shoulder and Elbow Surgery Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Anterior Elbow Capsulodesis FIGURE 3. A, A lateral radiograph showing residual posterior subluxation of the ulnohumeral and radiocapitellar joints before an anterior elbow capsulodesis. B, A lateral elbow radiograph showing improvement of the ulnohumeral and radiocapitellar joint subluxation following an anterior elbow capsulodesis. Note the transosseous suture holes (arrows) in the proximal ulna. to resist the posteriorly directed joint reactive forces produced by the biceps and triceps muscles.3Y5,7Y9 Failure to stabilize these fractures frequently results in posterior elbow instability. Less commonly recognized is the importance of the anterior joint capsule. The anterior elbow joint capsule is a fibrous-type structure originating proximal to the coronoid and radial fossae and extends distally to attach to the anterior margin of the coronoid process medially and to the annular ligament laterally.10,13 Avulsion of the anterior capsule usually occurs at its distal attachment.14,15 The brachialis inserting into the base of the coronoid process, distal to the anterior capsular insertion, usually has some muscle fibers inserting into the anterior joint capsule.3,13 Avulsion of the brachialis can also occur with an elbow dislocation.14 The anterior capsule has been variably described as providing no elbow joint stability,16 valgus joint stability,11 or resistance to posterior elbow stability.2,7,14,15 Previous reports have described insertion of the anterior capsule with or without a type 1 coronoid fragment attached to the capsule2,6,7,14,15 to help restore elbow stability. Capsular reattachment provides a buttress effect to the coronoid process similar to a volar plate arthroplasty for an unstable dorsal proximal interphalangeal joint fracture-dislocation.17 Similar to a digital volar plate arthroplasty, the sutures holes and sutures used to repair the anterior elbow capsule are placed at the junction of the greater sigmoid notch articular surface and the coronoid fracture site. This placement insures recreation of a congruent and smooth transition between the articular surface of the greater sigmoid notch and the repaired anterior capsule. An anterior capsular repair is not, however, needed in all cases of posterior elbow fracture-dislocations. Frequently following restoration of the ulnohumeral joint, reapproximation of the lateral collateral ligament complex to the lateral epicondyle, and radial head reconstruction or replacement, elbow stability is restored. If residual posterior instability with elbow extension is noted under fluoroscopic examination, then an anterior capsular repair should be considered. A hinged external fixator is also generally not needed. In this series, the external fixator was used in only one case involving a chronically posteriorly subluxed elbow. Its use should be considered also in cases where residual instability is noted even following all soft tissue repairs or in cases when the soft tissue and osseous repairs may need to be protected. In summary, an anterior elbow capsulodesis is an additional surgical option that should be considered when dealing with complex elbow fracture-dislocations. TABLE 2. Treatment and Results Patient 1 2 3 4 5 6 Average Radial head replacement Yes Yes Yes No Yes Yes Hinged external fixator No Yes No No No No Follow-up (mo) 22 15 33 18 20 6 Extension/flexion (degrees) 30/135 15/135 10/130 40/125 40/135 20/140 Pronation/supination (degrees) 75/85 40/40 45/85 45/85 50/50 70/70 19 26/133 54/69 Volume 7, Issue 1 Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 75 Lee et al If persistent posterior elbow instability, with elbow extension, occurs following reconstruction of the articular surfaces and the lateral collateral ligament complex, then an anterior elbow capsulodesis should be considered. m 8. Osborne G, Cotterill P. Recurrent dislocation of the elbow. J Bone Joint Surg. 1966;48B:340. 9. Regan W, Morrey BF. Fractures of the coronoid process of the ulna. J Bone Joint Surg. 1989;71A:1348Y1354. 10. Morrey BF. Anatomy of the elbow joint. In: Morrey BF ed. The Elbow and Its Disorders, 3rd ed. Philadelphia, PA: WB Saunders, 2000:13Y42. REFERENCES 1. Hotchkiss RN. Fractures and dislocations of the elbow. In: Rockwood CA, Green DP eds. Rockwood and Green’s Fractures in Adults, Vol 1, 4th ed. Philadelphia, PA: Lippincott-Raven, 1996:980Y981. 2. Lee DH. Treatment options for complex unstable fracturedislocations. Injury Int J Care Injured. 2001;32(Suppl D): 41Y69. 3. Morrey BF, O’Driscoll SW. Complex instability of the elbow. In: Morrey BF ed. The Elbow and Its Disorders, 3rd ed. Philadelphia, PA: WB Saunders, 2000:421Y436. 4. O’Driscoll SW, Morrey BF, Korinek S, et al. Elbow subluxation and dislocation: a spectrum of instability. Clin Orthop. 1992;280:186. 11. Morrey BF, An KN. Anterior and ligamentous contributions to the stability of the elbow joint. Am J Sports Med. 1983;11:315Y319. 12. Morrey BF, Tanaka S, An KN. Valgus stability of the elbow. A definition of primary and secondary constraints. Clin Orthop Relat Res. 1991;265:187Y195. 13. Neill Cage DJ, Abrams RA, Callahan JJ, et al. Soft tissue attachments of the ulnar coronoid process. Clin Orthop Relat Res. 1995;320:154Y158. 14. Dryer RF, Buckwalter JA, Sprague Bl. Treatment of chronic elbow instability. Clin Orthop Relat Res. 1980; 148:254Y255. 5. O’Driscoll SW. Elbow dislocations. In: Morrey BF ed. The Elbow and Its Disorders, 3rd ed. Philadelphia, PA: WB Saunders, 2000:409Y420. 15. Terada N, Yamada H, Seki T, et al. The importance of reducing small fractures of the coronoid process in the treatment of unstable elbow dislocation. J Shoulder Elbow Surg. 2000;9:344Y346. 6. O’Driscoll SW, Jupiter JB, King GJW, et al. The unstable elbow. J Bone Joint Surg [Instr Course Lect]. 2000; 50(82A):724Y738. 16. Nielsen KK, Olsen BS. No stabilizing effect of the joint capsule. A kinematic study. Acta Orthop Scand. 1999;70: 6Y8. 7. O’Driscoll SW, Jupiter JB, Cohen MS, et al. Difficult elbow fractures: pearls and pitfalls. AAOS [Instr Course Lect]. 2003;52:113Y134. 17. Eaton RG, Mallerich MM. Volar plate arthroplasty for the proximal interphalangeal joint: a ten-year review. J Hand Surg. 1980;5:260Y268. 76 Techniques in Shoulder and Elbow Surgery Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.