Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
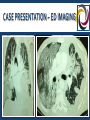
GRAND ROUNDS ~ RESPIRATORY FAILURE SECONDARY TO COMPLICATIONS FROM METASTATIC SYNOVIAL CELL SARCOMA Moderator / ICU: Dr Jeremy Barnett MD Pulmonary / ICU: Dr Anthony Guerrino MD Pharmacology: Priti Shah RPh ED: Dr Amy Gutman MD OBJECTIVES Multidisciplinary review of a oncological process with an rare complication with significant impacts on management of critically ill patients 3rd in the Kingston Hospital Grand Round Series ACCME application for accreditation initiated so state-required CME can be completed without leaving Kingston CASE PRESENTATION ~ CC & HPI 33 yo M with history of metastatic synovial sarcoma reports 24 hours history of increasing dyspnea Denies cough, fever, calf swelling, tenderness or prior history of similar events States that he had chest pain overnight, but not upon presentation. Also denies hemoptysis, recent URI, abdominal pain, N/V/D, melena, hematochezia, recent travel, prolonged immobility CASE PRESENTATION ~ PMH PMH: Metastatic synovial sarcoma FAMILY: (-) pertinent ALLERGIES: NKDA MEDICATIONS: Opdivo (nivolumab) SOCIAL: (+) former smoker (10 PYH) (+) occasional ETOH CASE PRESENTATION ~ ROS Limited initially due to respiratory distress; ROS more fully explored with family GENERAL: (-) prior fever GU: HEENT: (-) congestion SKIN / MS: (+) chronic pain PULM: (+) cough, (+) SOB / DOE (+) wheezing ENDO: (+) generalized weakness NEURO: (-) localized weakness PSYCH: (+) emotional stress CV: GI: (+) CP last night (-) abdominal pain (+) loss of appetite (+) weight loss (-) urinary complaints CASE PRESENTATION ~ EXAM VITALS: T 97.6 (oral) GENERAL: HEENT: PULM: CV: HR 105 / reg RR 30 / labored A&Ox3, moderate respiratory distress Membranes moist, airway patent; (-) conjunctival pallor, stridor, hoarseness, neck stiffness, LAD, JVD BS = BL; (+) rhonchi, (+) rales; (-) wheezes RRR (-) MRG, (+) tachycardic BP: 107/66 Sat 75% ra Wt 63.5 kg GI: Soft, NT, ND, BSAQ, cachectic GU: (-) LAD MUSC: Warm, dry, (-) cyanosis; surgical scars over R olecranon, (+) right PICC site CDI; (-) deformity, edema, calf tenderness NEURO: A&Ox3, afocal otherwise PSYCH: Anxious but appropriate CASE PRESENTATION ~ EKG Sinus tachycardia, rate of 120, short pr (110ms) with an incomplete right bundle branch block (QRS duration 100ms) & diffuse ST/T-wave changes including T-wave inversions & ST-depression CASE PRESENTATION ~ LABS UA: (+) Ketones Troponin: <0.010 129 85 13 LFTs: Alk Phos 376 / T Bili 1.3 AST / ALT 56 / 34 Albumin 3.8 3.8 26 0.78 Coags: PTT / Pt / INR 42 / 12 / 1 Lactic Acid: 21 ABG: 7.32 / 44 / 64 / 26 / 91 (FiO2 100%) COHb 2.5 133 13 16 228 39 AG = Na - (Cl + HCO3) AG = 129 – (85 + 26) = 18 Hypochloremic normal anion gap acidosis CASE PRESENTATION ~ ED IMAGING Extensive bilateral infiltrates Left pulmonary masses Hilar & mediastinal adenopathy Pleural effusions CASE PRESENTATION ~ ED IMAGING No pulmonary artery filling defects Pleural, pericardial & skeletal metastasis Left pleural effusions w/o pericardial effusion Mediastinal adenopathy with diffuse thickening of distal esophageal wall Bibasilar ground-glass consolidations with air bronchograms representing lymphagitic carcinomatosis vs pneumonitis CASE PRESENTATION ~INITIAL MANAGEMENT IV, O2, Monitor PICC access for initiation of sepsis protocol (O2, antibiotics, fluid resuscitation) 45 mins post-presentation, on-coming MD reviewed all diagnostics, re-examined patient & called his hospital of choice to arrange transfer Patient progressively worsening from the respiratory standpoint, increasingly anxious Advanced from NC to NRB, then high-flow O2 which patient did not tolerate BiPAP not attempted as patient did not tolerate high-flow O2 At this point, patient declining intubation, though wished to be “resuscitated” CASE PRESENTATION ~ ICU CONSULTATION Intensivist consulted to assist from pulmonary & CV standpoints Despite an initial acceptance at his hospital of choice, after 2 hours of promises of an open bed, the transfer was “put on hold until a bed was available” Intensivist accepted patient to the ICU rather than wait in ED for potential transfer Presumptive diagnoses of respiratory distress secondary to pneumonia, influenza, underlying metastatic process CASE PRESENTATION ~ CRITICAL CARE MANAGEMENT Patient increasingly anxious, with worsening oxygenation Patient & family agreed to intubation Immediately post intubation, he became hemodynamically unstable requiring norepinephrine & fluid resuscitation CT reviewed, demonstrating pneumothorax Likely secondary to tumor / scarring rupturing a bleb Chest tube high risk due to scarring / masses Continued on 100% FIO2 Large needle taped to patient’s chest INITIATING MECHANICAL VENTILATION ~ RATIONALE Airway Protection NO gas exchange derangements CNS or mechanical loss of airway protection / patency Hypoxic Respiratory Failure pO2 < 50 on 100% NRB Decreased ambient FiO2, increased pCO2, diffusion block, V/Q mismatch, right-left shunt Hypercarbic Respiratory Failure pH < 7.3, pCO2 > 50 Acute vs chronic, “Won’t” vs “Can’t”, CNS vs Bellows www.nursingconsult.com INITIATING MECHANICAL VENTILATION Thoughtful process Use numbers to guide you If you can’t fix the process with non-invasive measures, then commit to prophylactic intubation rather than wait until patient in extremis Allows patient to rest while you gather data & figure out how to manage their physiological process(es) Remember, sometimes it is easy but wrong TO intubate….sometimes it is easy & wrong NOT to intubate NITROGEN WASHOUT TEST Gauges functional residual capacity & airflow Evaluates for dead space without gas exchange Usually caused by non-functional alveolar capillaries not absorbing O2 or expelling CO2 Dead space decreases lung efficiency function To accurately measure effects a lung disease will have on lung function the test evaluates for: Volume: overall amount of air filling lungs Capacity: actual amount of air used in regular breathing Functional Residual Capacity: amount of unused air in lungs Diffusing Capacity: ability of alveoli to absorb O2 into bloodstream Airflow: physical ability to pull in & expel air ICU COURSE 100% FiO2 / low PEEP x until PTX resolved Pan-cultured while initiated / continued on: Antibiotics: Piperacillin-tazobactam, Vancomycin, Meropenem Antiviral: Oseltamivir Antifungal: Micafungin Sedation / Analgesia: Dexmedetoimidine, Fentanyl Pulmonary: Ipratropium Nitrogen washout testing preformed ICU Day 2 ICU COURSE ~ CULTURES (+) S. epidermidis from both aerobic bottles pansensitive except to PCN (+) M. pneumonia IgG Ab & IgM Ab (+) CMV Nasal / Sputum (-) Influenza A & B PCR (-) RSV Bronchial wash: normal respiratory flora, (-) pneumocystis Negative Cultures: Anaerobic bottles at 48 hours Legionella pneumophila AFB, acid-fast MRSA Viral Candida Alpha-1-Antitrypsin deficiency mutation Stool: (-) Clostridium difficile toxin A & B ICU COURSE Transferred to ICU / oncology unit at NYU where he received care, including monoclonal antibody therapy Remained intubated, with mild improvement in lung function Dr Llobet confirmed masses seen on CT were not on a CT scan from 1 month earlier Continued on vasopressors, sedation, antivirals, antibiotics and pulmonary medications throughout his stay Discharge diagnoses: Respiratory failure secondary to: Pneumonia with possible empyema Metastatic synovial cell sarcoma with space-occupying lung masses Immune-mediated pneumonitis / interstitial lung disease ICU Day 3 SYNOVIAL CELL SARCOMA BACKGROUND Soft tissue sarcomas are a heterogeneous group of rare mesenchymal tumors which include synovial cell sarcomas Malignant precursor cells differentiate along muscle, adipose, fibrous, cartilage, nerve, or vascular tissue Arise in limbs, thorax, head, neck, abdominal cavity, retroperitoneum Improved survival improved due to early / radical surgery, along with radiation Tumorlibrary.com EPIDEMIOLOGY Incidence 2.75 per 100,000 ~800 new cases in US annually Male:Female 1:1 prevalence 5-10% of all soft-tissue sarcomas Generally presents at a younger age than other soft tissue sarcomas 3rd most common soft-tissue tumor in adolescents & young adults 1/3 cases diagnosed in those under 20 years of age Mean age at diagnosis ~30 years of age Tumorlibrary.com SYNOVIAL CELL SARCOMA CELL ORIGIN Not associated with synovium, rather undifferentiated mesenchymal cells Named for similarity between tumor cells & primitive synoviocytes Neurologic origin suggested due to histologic resemblance between neural cells of malignant peripheral nerve sheath tumor & synovial cell sarcomas Stem Cell Reviews and Reports. March 2011, Volume 7, Issue 1, pp 32-42 SARCOMA METASTATIC DISEASE Occurs most often in para-articular regions, though can arise from tendon sheaths, bursae or joint capsules Primary metastatic site is pulmonary Extrapulmonary metastases to local bones, fascial planes / soft tissue, spine, paraspinous tissues Hematogenous or lymphatic dissemination rare but life-threatening Retroperitoneal & visceral sarcomas primarily metastasize locally or hepatically www.spandidos-publications.com PRESENTATION Usually occurs within the 1st three decades with patients being symptomatic months to years prior to diagnosis HPI: small, painful nodule rapidly increasing in size 80% occur in extremities, 70% in lower limbs Popliteal fossa most common, followed by hands / feet, though affects entire appendicular skeleton Most sarcomas intermuscular, found within 5 cm of a joint Intra-articular origin <10 % of cases PLAIN RADIOGRAPHS Normal in ~50% Spotty / irregular calcifications (“snowstorm”) within soft tissue matrix in a peripheral distribution 10-20% show periosteal reaction, bony erosion or invasion Tumorlibrary.com COMPUTED TOMOGRAPHY Confirm presence of mass, describe size & location, but non-diagnostic Often detects secondary bony involvement or metastatic spread prior to identification of primary lesion posterng.netkey.at; J Korean Surg Soc. 2012 Dec;83(6):403-407 MAGNETIC RESONANCE IMAGING Diagnostic test of choice Low signal intensity (T1) vs high signal intensity (T2-weighted) “Triple Signal Intensity Sign” Pathognomonic (30-50%) Hypointense, isointense & hyperintense with fat on T2–weighted Matrix signal homogeneous unless calcifications present With contrast enhancement appears heterogeneous with nodular enhancement & cysts Often mistaken for ganglion cysts Tumorsurgery.org SAGITTAL T2 WEIGHTED AXIAL T2 WEIGHTED Tumorsurgery.org DIAGNOSTIC IMAGING COMPARISONS radiologycases.com; roentgenrayreader.blogspot.com HISTOLOGY / GROSS PATHOLOGY Appearance similar to other round blue cell tumors Circumscribed, round or multilobed May grow to >15 cm, but average 3-5 cm diameter Less differentiated variants grow rapidly, are poorly circumscribed, have multiple areas of hemorrhage, necrosis & cystic formation Macroscopically, yellow to gray-white & “greasy” Three types of synovial sarcoma: Monophasic, Biphasic, Poorly Differentiated www.kjim.org; tumorsurgery.org MICROSCOPIC PATHOLOGY ~ TWO CELL TYPES SPINDLE CELL Small, uniform & ovoid cells with pale nuclei & sparse cytoplasm EPITHELIOID CELLS Ovoid nuclei & abundant cytoplasm MONOPHASIC Types: Fibrosarcoma, leiomyosarcoma, epithelioid, clear cell Monophasic Fibrous: Predominantly spindle cells mixed with round cells Arranged in fascicles, poorly defined cytoplasm without glandular areas Monophasic Epithelial: Difficult to differentiate from adenocarcinoma BIPHASIC Types: Malignant peripheral nerve sheath, carcinoma, diffuse type tenosynovial giant cell tumor Columnar epithelial & spindle-cell components in equal proportions Round cells & spindle-shaped fibroblasts alternate with glandular-like areas lined by mucin-containing synoviallike cells POORLY DIFFERENTIATED Types: Malignant peripheral nerve sheath tumor, fibrosarcoma, hemangiopericytoma, Primitive peripheral neuroectodermal High grade round cell tumor with dense cellularity, numerous mitoses, necrosis & punctate calcifications Histologically graded by mitotic activity plus necrosis: Grade 1 (differentiated) to grade 3 (poorly differentiated) Immunohistochemically positive for vimentin, cytokeratin, or epithelial membrane antigen LABORATORY STUDIES Histology & molecular diagnostic testing diagnostic 90% have translocation & fusion between chromosomes 18 SYT gene & short arm of chromosome X SSX gene t(X;18)(p11;q11) with variants SYT-SSX1, SYT-SSX2, or SYT-SSX4 Reverse transcriptase-PCR 96% sensitive, 100% specific Fluorescence in situ hybridization (FISH) less expensive than RT-PCR but with a lower sensitivity SURGICAL MANAGEMENT Excision is cornerstone of treatment Careful preoperative staging crucial as resection of isolated metastases increases survival if primary tumor well controlled Palliative surgery appropriate, particularly to alleviate pain or achieve hemorrhage control Tumorsurgery.org SURGICAL MANAGEMENT Surgical approach plans for a wide / radical resection Amputation required in 20% of patients due to required tumor-free margin of 1-3 cm Tumorsurgery.org RADIATION THERAPY Preoperative radiation therapy associated with poor wound healing, though often recommended to reduce tumor size Post-operative radiation recommended, particularly if margins close to vital neurovascular structures External-beam radiation (40-60 Gy) directed at tumor site & surrounding normal tissue margins Vital neurologic structures, open physes, or extreme peripheral location increase complications Alternatives are brachytherapy & / or intensity-modulated radiation therapy (IMRT) aapm.org MEDICAL THERAPY Chemotherapy as adjuvant or neoadjuvant treatment to post-operative radiotherapy does not increase survival or disease control unless primary tumor >5cm, but may improve months of survival Granulocyte colony-stimulating factor (G-CSF) added to any chemotherapy stimulates healthy marrow growth Clinical trials: Promising results with a murine monoclonal antibody that attacks frizzled homologue cell-surface receptor (FZD10), present only in sarcoma cells Innovative SYT-SSX–derived peptide vaccine in phase 2 trials Uptodate.com OPDIVO® (NIVOLUMAB) Patient undergoing Opdivo (nivolumab) therapy for unresectable sarcoma Acute pneumonitis / interstitial lung disease thought be a result of Opdivo, contributing to acute respiratory failure & susceptibility to sepsis Opdivo is a human monoclonal antibody that blocks interaction between PD-1 & it’s ligands PD-L1 / PD-L2 Indicated for treatment of unresectable metastatic melanoma, advanced sarcoma, non-small cell carcinoma, or disease progression after platinum-based chemotherapy (i.e. ipilimumab / Yervoy®) Given as single agent, or with ipilimumab , a monoclonal antibody targeting CTLA-4 protein receptors, allowing cytotoxic T lymphocytes to recognize & destroy cancer cells Combined nivolumab & ipilimumab results in enhanced T-cell function greater than the effects of either antibody alone OPDIVO® (NIVOLUMAB) MECHANISM OF ACTION Inhibits binding of PD-1 ligands to T cell PD-1 receptors, inhibiting T-cell proliferation & cytokine production resulting in decreased tumor growth PD-1 ligand upregulation contributes to inhibition of active T-cell tumor immune surveillance Opdivohcp.org OPDIVO® (NIVOLUMAB) PHARMACOKINETICS No specific contraindications other than pregnancy, breast-feeding, & development of specific adverse reactions Weight-based dosing 3 mg/kg IV over 60 minutes every 2 weeks until disease progression or unacceptable toxicity Half-life: 25 days Mean clearance 10 mL/hr No effect on the clearance for age, gender, race, tumor size / type, LDH, PD-L1 expression, renal or hepatic impairment discovermedicine.com No drug-drug interaction studies conducted OPDIVO® (NIVOLUMAB) SIDE EFFECTS ~ ALL “IMMUNE MEDIATED” GI: Colitis, hepatitis, bloody diarrhea, weight loss, jaundice, constipation, N/V HEENT: Sclera injection, photophobia, dacrocystitis, oral ulcers, deepening of voice CV: Tachyarrhythmia, bradyarrythmia, ischemia MS: Back pain, “bone” pain, muscle cramps Endo: Hypo/ hyperthyroid, edema, fatigue, heat / cold sensitivity, diaphoresis Renal: Nephritis, AKI / ARF, hematuria Skin: Dermatitis, blistering, hair loss CNS / PNS: Encephalitis, diplopia, dizziness / vertigo, syncope, persistent headache Psych: Depression / anxiety, insomnia, night sweats Pulmonary: Pneumonitis, interstitial lung disease, respiratory distress, thickening of bronchial secretions, persistent cough OPDIVO® (NIVOLUMAB) ASSOCIATED PNEUMONITIS By FDA definition the immune-mediated pneumonitis must have no clear etiology other than the PD1-inihibtor therapy & require use of corticosteroids Immune-mediated pneumonitis & / or interstitial lung disease are adverse effects of all PD1inhibitor therapies Median time to pneumonitis development after initiating treatment is 5 months In one phase 2 trial, pneumonitis was a common “life-threatening” adverse event, occurring in 5% of all patients3 In two recent phase 3 trials, the incidence of pneumonitis was 1.5%1 & 1.9%2 Across clinical trials in 1590 patients with solid tumors, fatal immune-mediated pneumonitis occurred in 0.3% (5/1590) of patients receiving nivolumab as a single agent 1NEJM. 2015;372:320-330; 2Lancet Oncol. 2015;16:375-384; 3Lancet Oncol. 2015;16:257-265 PNEUMONITIS CLINICAL GRADING SYSTEMS Group Grade 1 Grade 2 Grade 3 Grade 4 South-West Oncology Group Radiographic changes; symptoms do not require steroids Steroids required, or pleurocentesis of pleural effusion O2 required Requires assisted ventilation Radiation Therapy Oncology Group Mild symptoms of dry cough or DOE Persistent cough requiring narcotic or antitussives; dyspnea with minimal efforts but not at rest Severe cough unresponsive to antitussives; dyspnea at rest, clinical / radiologic evidence of acute pneumonitis; O2 or steroids required Severe respiratory insufficiency, continuous O2 or assisted ventilation National Cancer Institute Asymptomatic, radiographic findings only Symptomatic, but not interfering with ADLs Symptomatic, interferes with ADLs, O2 required Life-threatening; ventilatory support indicated Semin Oncol 32(Suppl 3): S42-S54. Int J Radiation Oncology Biol Phys. 63(1):5-24 OPDIVO® (NIVOLUMAB) ASSOCIATED PNEUMONITIS Management: High-dose systemic corticosteroids (>40 mg prednisone or equivalent / day) followed by a taper Temporarily withhold nivolumab in moderate (grade 2) pneumonitis Permanent discontinuation in severe (grade 3) or life-threatening (grade 4) pneumonitis Pneumonitis led to discontinuation of PD-1 inhibitor in 1% all patients In one study, symptoms completely resolved in 7 of 9 patients with grade 2 or 3 pneumonitis1 Low-power image showing interstitial pneumonia and necrosis with areas of hemorrhage. www.captodayonline.com 1NEJM. 2015;372:320-330 SYNOVIAL CELL SARCOMA PROGNOSIS After metastases, disease stabilization viewed as a realistic end point as essentially incurable Median survival after distant metastases 11-15 months with 25% 2-3 year survival In selected patients, resection of pulmonary metastases increases 5 year survival to 25-40% Prognostic factors for prolonged survival differ from those predicting chemotherapy response, suggesting survival more dependent upon disease biology than treatment In metastatic unresectable disease, systemic therapy provides symptom palliation, slows progression, & may prolong survival Survival curves for primary sites based upon data from 3677 patients with STS treated at Sloan-Kettering 1982-2001. Borden EC, et al. Soft tissue sarcomas of adults: State of the translational science. Clin Cancer Res 2003; 9:1941. PROGNOSIS Outcome predicted by: Tumor size, Anatomic localization, Histologic grade POOR PROGNOSIS Poorly differentiated histology Recurrence Male gender Metastases at presentation 25% 2 year survival Bone or neurovascular invasion Proximal extremity or truncal tumor location GOOD PROGNOSIS Biphasic histologic pattern SYT/SSX2 fusion genes Hand or foot location Size < 5 cm Female gender Age < 50 years Negative resection margins SYNOVIAL SARCOMA PROGNOSIS In a recent study, 60% patients responding to Opdivo were still responding six months later Study of nivolumab in subjects with advanced or metastatic squamous cell non-small cell lung cancer who have received at least two prior systemic regimens (CheckMate 063). Accessed December 2015. CASE FOLLOW-UP Patient transferred to NYU on Day….of his ICU stay WILL FILL IN THIS SLIDE WHEN I CLARIFY DETAILS ON MONDAY ADDITIONAL REFERENCES Images: Tumorsurgery.org, Wikipedia, Google, Bing, Medline image searches Lessnick SL, Dei Tos AP, Sorensen PH, Dileo P, Baker LH, Ferrari S, et al. Eilber FC, Dry SM. Diagnosis and management of synovial sarcoma. J Surg Oncol. 2008 Mar 15. 97(4):314-20. Bergh P, Meis-Kindblom JM, Gherlinzoni F, Berlin O, Bacchini P, Bertoni F, et al. Synovial sarcoma: identification of low and high risk groups. Cancer. 1999 Jun 15. 85(12):2596-607. Spira AI. The use of chemotherapy in soft-tissue sarcomas. Oncologist. 2002. 7(4):348-59. Zagars GK, Ballo MT, Pisters PW, Pollock RE, Patel SR, Benjamin RS, et al. Prognostic factors for patients with localized soft-tissue sarcoma treated with conservation surgery and radiation therapy: an analysis of 1225 patients. Cancer. 2003 May 15. 97(10):2530-43. Sakabe T, Murata H, Konishi E, Takeshita H, Ueda H, Matsui T, et al. Evaluation of clinical outcomes and prognostic factors for synovial sarcoma arising from the extremities. Med Sci Monit. 2008 Jun. 14(6):CR305-310. Mazeron JJ, Suit HD. Lymph nodes as sites of metastases from sarcomas of soft tissue. Cancer. 1987 Oct 15. 60(8):1800-8. Deshmukh R, Mankin HJ, Singer S. Synovial sarcoma: the importance of size and location for survival. Clin Orthop Relat Res. 2004 Feb. 155-61. Pisters PW, Harrison LB, Leung DH, Woodruff JM, Casper ES, Brennan MF. Long-term results of a prospective randomized trial of adjuvant brachytherapy in soft tissue sarcoma. J Clin Oncol. 1996 Mar. 14(3):859-68. Ladenstein R, Treuner J, Koscielniak E, d'Oleire F, Keim M, Gadner H, et al. Synovial sarcoma of childhood and adolescence. Report of the German CWS-81 study. Cancer. 1993 Jun 1. 71(11):3647-55. Stefanovski PD, Bidoli E, De Paoli A, Buonadonna A, Boz G, Libra M, et al. Prognostic factors in soft tissue sarcomas: a study of 395 patients. Eur J Surg Oncol. 2002 Mar. 28(2):153-64. Kawai A, Woodruff J, Healey JH, Brennan MF, Antonescu CR, Ladanyi M. SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. N Engl J Med. 1998 Jan 15. 338(3):153-60. Spillane AJ, A'Hern R, Judson IR, Fisher C, Thomas JM. Synovial sarcoma: a clinicopathologic, staging, and prognostic assessment. J Clin Oncol. 2000 Nov 15. 18(22):3794-803. Thompson RC Jr, Garg A, Goswitz J, Cheng EY, Clohisy DR, Dusenbery K. Synovial sarcoma. Large size predicts poor outcome. Clin Orthop Relat Res. 2000 Apr. 18-24. Ten Heuvel SE, Hoekstra HJ, Suurmeijer AJ. Diagnostic accuracy of FISH and RT-PCR in 50 routinely processed synovial sarcomas. Appl Immunohistochem Mol Morphol. 2008 May. 16(3):246-50. www.uptodate.com. “Soft Tissues Sarcoma”, Synovial Cell Sarcoma”, “Opdivo”. Accesed Dec 2015 N Engl J Med. 2015;373:288-290 Kind M, Stock N, Coindre JM. Histology and imaging of soft tissue sarcomas. Eur J Radiol. 2009 Oct. 72(1):6-15. Judson I, et al. Lancet Oncol 2014; 15:415. Accessed online December 2015. Mesna tablets. United States Prescribing Information. US National Library of Medicine. (Available online at dailymed.nlm.gov, accessed May 13, 2014) NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V.2.2016. © 2015 National Comprehensive Cancer Network, Inc. All rights reserved. Accessed December 2015 SUMMARY Multidisciplinary review of a oncological process with an rare Reminder…. complication with significant impacts on management of critically ill patients Grand Rounds will be every other month until final Review of the indications for mechanical ventilation ACCME CME Approval Review of a novel monoclonal antibody agent with significant side effects February ~ Focusing on a Surgical Case