Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
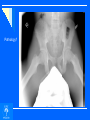
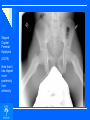
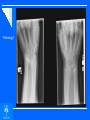
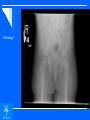
UNC MSK Course Day 1 Lab XR UNKNOWNS (for self study) Pathology? Old fracture of radius with growth arrest of distal radial physis. Relative overgrowth with distal and dorsal dislocation of distal ulna Pathology? Pathology? Pathology? Slipped Capital Femoral Epiphysis (SCFE) Note that it has slipped more posteriorly than anteriorly Slipped Capital Femoral Epiphysis (SCFE) Note that a line drawn along the anterior femoral neck intersects the head on the R but not on the L. Slipped Capital Femoral Epiphysis (SCFE) A screw has been placed on the L to prevent further slip. Pathology? Polydactyly Inheritance? Polydactyly Inheritance for postaxial polydactyly is frequently autosomal dominant, whereas preaxial (duplicate thumb) is usually spontaneous. Pathology? Hemihypertrophy Note: all structures slightly enlarged on the right. Pathology? Osteochondromatosis (Multiple hereditary exotoses) Inheritance? Osteochondromatosis (Multiple hereditary exotoses) Typically autosomal dominant inheritance. Bones often deformed due to pressure or growth abnomalities Pathology? Osteopetrosis Inheritance? Osteopetrosis (Multifactorial and there are autosomal dominant and recessive forms) Note: Bone is dense, marrow space is decreased – Why? Osteopetrosis Note: Bone is dense, marrow space is decreased because osteoclasts are not removing bone to enlarge marrow canal. Pathology? Hypophosphatemic (Vitamin D Resistant) Rickets (May be difficult to differentiate from other causes of bowing on basis of X-ray alone.) Inheritance? Wide physis better seen here Hypophosphatemic (Vitamin D Resistant) Rickets (May be difficult to differentiate from other causes of bowing on basis of X-ray alone.) (Sex linked dominant trait) Pathology? Osteogenesis Imperfecta Severe Inheritance? Mild Moderate Osteogenesis Imperfecta Severe (Autosomal dominant or recessive) Many degrees of severity. Associated with what external finding? Mild Moderate Osteogenesis Imperfecta Severe (Autosomal dominant or recessive) Many degrees of severity. Associated with blue sclera. Mild Pathology? Bladder extrophy Note: Wide pubic symphysis resulting from abnormal development of the cloaca. Pathology? Congenital scoliosis How do you know it isn’t “idiopathic scoliosis”? Congenital scoliosis Note: Presence of hemivertebra Congenital scoliosis Note: Presence of hemivertebra Pathology? Spina Bifida L4-sacrum Note: Wide pedicles and absence of spinous processes. Spina Bifida L4-sacrum Note: Wide pedicles and absence of spinous processes. Inheritance? Spina Bifida L4-sacrum Note: Wide pedicles and absence of spinous processes. Multifactorial – genetic plus intrauterine influences especially prenatal folic acid deficiency Pathology? Proximal Femoral Focal Deficiency (PFFD) Pathology? Pathology? “Scanogram” of another patient with the same condition, shows x-rays of the hips, knees and ankles all shot over a ruler to allow measurement of the leg length discrepancy which is often present Fibular Hemimelia (congenital absence of fibula) (Can be familial) Pathology? Radial hemimelia (Radial Club Hand) Not the same patient, note absence of thumb in this case. Pathology? Pathology? Madelung’s Deformity Note the "V" shaped proximal carpal row. Congenital Madelung’s may be due to an abnormal fibrous band tethering the sigmoid notch of the radius proximally to the ulna and slowing the growth. Traumatic Madelung's may follow partial growth arrest of the distal radius (seen earlier). Pathology? Spondyloepiphyseal dysplasia Note: Platyspondyly or “flat vertebrae.” Pathology? Developmental dysplasia of the hip (DDH) Note: Absence of ossification center L femoral head Inheritance? Developmental dysplasia of the hip (DDH) Note: Absence of ossification center L femoral head Inheritance – multifactorial including intrauterine and post natal positioning influences. Developmental dysplasia of the hip (DDH) Note: Break in Shenton’s line on L with small ossific nucleus Developmental dysplasia of the hip (DDH) Note: Break in Shenton’s line on L with small ossific nucleus Break Shenton’s line Developmental dysplasia of the hip (DDH) Note: Acetabular angle should be less than 30 degrees at birth and less than 20 degrees by age 2 years. The ossific nucleus should be in the inner lower quadrant of the crossing of Hilgenreiner’s line (through the triradiate cartilages) and a perpendicular line through the AIIS. Alaska