Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
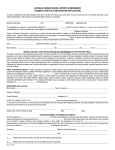
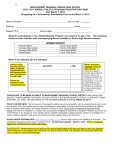
Nauset Regional High School Athletic Department PO Box 1887 North Eastham, MA 02651 For Office Use Only Date to Athletic Office: ____________ Physical Date: ________________ Impact Date: ___________________ Parent Meeting: _______________ PHYSICAL DATE MUST BE AFTER: July 20th, 2011 RETURN BY: August 1st, 2012 ImPACT Testing Dates: Middle School; May 30th & 31st/High School; June 6th & 7th PLEASE CIRCLE ONE SPORT: BOYS: FOOTBALL SOCCER GIRLS: FIELD HOCKEY SOCCER COED: CREW CROSS COUNTRY CROSS COUNTRY GOLF VOLLEYBALL CHEER EMERGENCY CONTACT INFORMATION This form is to be used by the athletic trainer or EMT on site, in the event of an emergency when you cannot be reached. Please complete, sign, and return this form to the school prior to the first practice of the athletic season. Student’s Name: ___________________________________ Birthdate: ____________ SS#: _____________ Year of Graduation: _______________ Parent’s Name: _______________________________________ Address: _______________________________________ City: ______________ Zip Code: _________ Phone #: ______________________ Work #: _______________________ Cell #: ______________________ Parent E-Mail Address: _____________________________________ Student Email: ____________________________________________ In Case of an Emergency Contact: __________________________ Phone #:_______________________ (Other than Parent or Guardian) Insurance Group: _________________________________ Policy #: _________________________ Primary Care Physician:____________________________ Phone #: _________________________ Allergies to Insect/Medications/Foods: NO/YES If Yes, please explain: _______________________________ Do You Wear Glasses or Contacts NO/YES If Yes, please specify: __________________________________ MEDICAL HISTORY QUESTIONNAIRE 1. Please list any previous significant injuries your child has sustained: ______________________________ ____________________________________________________________________________________ 2. Have you had any prior surgery/surgeries? Please explain: _____________________________________ ____________________________________________________________________________________ 3. Have you had any illnesses or injuries in the past year that have kept you from participating in athletics or school? If yes, please explain: ____________________________________________________________ ____________________________________________________________________________________ 4. Were you seen or treated by a doctor for the previous illness or injury? If yes, please name the physician and the diagnosis: _____________________________________________________________________ ____________________________________________________________________________________ 5. Have you ever suffered from a concussion that was diagnosed by a physician or an Athletic Trainer? If yes, how many times and when: __________________________________________________________ 6. Have you ever suffered from a hit to the head where you have had a headache, nausea, dizziness, or lightheaded? If yes, how many times and when: _____________________________________________ 7. Have you ever been diagnosed with any of the following; if you answer yes, please explain: a. Headache or Migraines: (NO/YES):____________________________________________ b. Learning Disability or Dyslexia: (NO/YES): ______________________________________ c. ADD/ADHD: (NO/YES): ____________________________________________________ d. Depression, Anxiety, or any other psychiatric Disorder: (NO/YES): ___________________ ________________________________________________________________________ e. Seizure Disorder: (NO/YES): ________________________________________________ 8. Have you been told by a doctor not to participate in a certain sport? If yes, please explain: ___________ __________________________________________________________________________________ 9. Do you have asthma, diabetes, or heart related conditions that the Athletic Trainer should be aware of? Please explain: ________________________________________________________________________ ____________________________________________________________________________________ 10. Do you have a medical condition that requires the use of medication? Please list all medications (asthma inhalers, insulin, epi-pens, etc) and explain: _________________________________________________ ____________________________________________________________________________________ 11. Are you required to wear protective devices such as knee, ankle or shoulder braces as directed by a physician? If yes, please explain: _________________________________________________________ 12. Are there any other medical conditions the Athletic Trainer should be aware of: _____________________ ____________________________________________________________________________________ I hereby authorize in advance any necessary medical treatment required for my son/daughter while he/she is participating in Nauset Regional High School activities. This includes treatment by the certified athletic trainer on site, EMT’s, team physician (Dr. Andrew Judelson) and school physician (Dr. Nancy Golden), and emergency medical staff at area hospitals. I have read the student athlete handbook at Nauset Regional High School and will abide by its guidelines and maintain good athletic citizenship while participating in athletics at Nauset Regional High School. I herewith give permission for my son/daughter to participate in athletics and all trips and activities related to the athletic program. I also give permission for my child _________________________ to receive Tylenol (2 tablets, 650mg), Calcium carbonate (Tums) and/or Ibuprofen (2 tablets, 400mg). If at all possible over the counter medication should be given out at home prior to school and/or athletics. NEW THIS YEAR MANDATED CONCUSSION COURSE INFORMATION: I have been given all information regarding head injuries and trauma that can be sustained while participating in athletics at Nauset Regional High School. It is understood that I will review the material given by the MIAA and Nauset Regional High School and will use the CDC website to complete the sports concussion awareness course on line @ www.nfhslearn.com. This is in accordance with the MIAA & the Commonwealth of Massachusetts Department of Public Health. All parents or guardians are required to do so prior to the start of the athletic season. It is further understood that as parent(s) or guardian(s) you acknowledge that you have successfully completed said course. Please print a copy of the completion certificate for your records. Notice of risk: Student athletes and the student’s parent or guardian need to be aware that sports activities involve risk of injury. When an athlete practices, plays or participates in any sport, the activity can be dangerous. The student risks serious, permanent injury, and possibly death. Instructions given by the coach/certified athletic trainer regarding playing techniques, hitting techniques (where applicable), weight training, proper equipment usage and team rules must be followed. X Student’s Signature: __________________________ __ Date: ________ X Parent’s/Guardian’s Signature: ____________________ Date: ________