Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
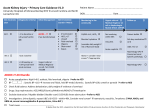
Management of Acute Kidney Injury Type: Policy Register No: 13007 Status: Public Developed in response to: Contributes to: CQC Outcome Local need NCEPOD on AKI 4 Consulted With Dr Abeygunasekara Post/Committee/Group Consultant Nephrologist Date 17/1/2013 Dr Aung Lwin ITU and Acute Medical Consultant ITU Consultant Dr Kevin Kiff, ITU Consultant 12/3/2012 Dr Jake Collins Professionally Approved By Version Number Issuing Directorate Ratified by: Ratified on: Executive Management Group Implementation Date Next Review Date Author/Contact for Information Policy to be followed by (target staff) Distribution Method Related Trust Policies (to be read in conjunction with) Document Review History Version No 1.0 1.1 Extended for 6 mths agreed by DRAG Chair 12/3/2013 12/3/2013 1.1 Emergency Care Document Ratification Group 28th March 2013 April 2013 15th April 2013 December 2016 Dr Anthony Chan, Consultant Nephrologist Medical and Nursing Staff Intranet & Website 10080 Adult Patients Observation Policy Authored/Reviewed by Active Date Dr Anthony Chan, Consultant Nephrologist Dr Anthony Chan, Consultant Nephrologist 15 April 2013 14th June 2016 1 INDEX 1.0 Purpose of guideline 2.0 Background 3.0 Scope 4.0 Definition of Acute Kidney Injury 5.0 Staging of Acute Kidney Injury 6.0 Diagnosis and risk assessment of Acute Kidney Injury 7.0 Investigations for Acute Kidney Injury 8.0 Management of Acute Kidney Injury 9.0 Referral to specialist services for Acute Kidney Injury 10.0 Training 11.0 Implementation and Communication 12.0 Breaches 13.0 Audit and monitoring 14.0 References Appendix 1 Algorithm for the Preliminary Management of Acute Kidney Injury 2 1.0 Purpose of Guideline 1.1 This guideline is intended to provide guidance on the preliminary management of acute kidney injury in non-specialist areas such as accident & emergency, acute admission units and general wards. 2.0 Background 2.1 AKI (Acute Kidney Injury) is common in hospitalised patients and is associated with poor prognosis and high mortality. Patients presenting with uncomplicated AKI have a mortality rate of up to 10%. In contrast, patients with AKI and multi-organ failure are reported to have mortality rates of over 50% and rises further to as high as 80% if renal replacement therapy is required. 2.2 The UK National Confidential Enquiry into Patient Outcome and Death (NCEPOD) Adding Insult to Injury Acute Kidney Injury Report 2009, examined the care of patients who died with a diagnosis of AKI. The report identified many deficiencies in the care of patients with AKI and only 50% of patients received what it considers ‘good care’. There was poor attention to detail, inadequate assessment of risk factors for AKI and an unacceptable delay in recognising post admission AKI. 2.3 The UK National Confidential Enquiry into Patient Outcome and Death (NCEPOD) AKI report recommends: • • • • • • • all emergency admissions should have a risk assessment for AKI all emergency admissions should have electrolytes checked on admission and appropriately thereafter predictable avoidable AKI should not occur all acute admission should receive adequate senior reviews (consultant review within 12 hours) there should be sufficient critical care and renal beds to allow rapid step up care undergraduate medical training should include the recognition of the acutely ill patient and the prevention, diagnosis and management of AKI postgraduate training in all specialties should include training in the detection, prevention and management of AKI. 3.0 Scope 3.1 This guideline applies to the management of acute kidney injury in adult patients only. 3.2 The management of esoteric causes of AKI is not covered in this guideline. 3.3 Hyperkalemia in acute kidney injury is not covered in this guideline. 3.4 It is inappropriate to refer AKI patients with more than single-organ dysfunction, to the Renal Service when it is anticipated that they will require more than renal replacement therapy. For example the septic, hypotensive and respiratory compromised patient with AKI will require critical care referral (ITU) instead of the renal services. 4.0 Definition of Acute Kidney Injury 4.1 Acute kidney injury is defined when one of the following criteria is met • Serum creatinine rises by ≥ 26µmol/L within 48 hours or 3 • • • Serum creatinine rises ≥ 1.5 fold from the reference value, which is known or presumed to have occurred within one week or urine output is < 0.5ml/kg/hr for >6 consecutive hours 4.2 The reference serum creatinine should be the lowest creatinine value recorded within 3 months of the event. 4.3 If a reference serum creatinine value is not available within 3 months and AKI is suspected • repeat serum creatinine within 24 hours • a reference serum creatinine value can be estimated from the nadir serum creatinine value if patient recovers from AKI 5.0 Staging of Acute Kidney Injury Stage Serum creatinine (SCr) criteria Urine output criteria 1 increase ≥ 26 μmol/L within 48hrs or <0.5 mL/kg/hr for>6 consecutive hrs increase ≥1.5 to 1.9 X reference SCr 2 increase ≥ 2 to 2.9 X reference SCr <0.5 mL/kg/ hr for > 12 hrs 3 increase ≥3 X reference SCr or <0.3 mL/kg/ hr for > 24 hrs or anuria for 12 hrs increase ≥354 μmol/L or commenced on renal replacement therapy (RRT) irrespective of stage 6.0 Diagnosis and risk assessment of Acute Kidney Injury 6.1 Clinical assessment of the patient with AKI should include comprehensive history and physical examination. 6.2 The history taking should include the following: • Review of patient notes • AKI risk factors: • age > 75 yrs • chronic kidney disease (CKD,eGFR< 60 mls/min/1.73m2) • Cardiac failure • Atherosclerotic peripheral vascular disease • Liver disease • Diabetes mellitus 4 • Review of medications • Look for potential causes for AKI including • • reduced fluid intake • increased fluid losses • urinary tract symptoms • recent drug ingestion • sepsis Systemic clinical features suggestive of vasculitides • • • 6.3 fever rash joint pains Clinical examination must include: • • General • rash • uveitis • joint swelling Assessment of volume status • core temperature • peripheral perfusion • heart rate • blood pressure • jugular venous pressure • signs of renovascular disease • audible bruits • impalpable peripheral pulses • abdominal examination • palpable bladder 7.0 Investigations for Acute Kidney Injury 7.1 All patients presenting with AKI should have appropriate baseline investigations performed which should include a urinalysis and a renal tract ultrasound within 24 hours. 7.2 Baseline set of laboratory investigations should be sent including: • Urea and electrolytes • FBC and clotting profile • urinalysis (± microscopy) 5 • 7.3 microbiology urine culture (if infection is suspected) blood culture (if infection is suspected) Specific renal investigations are requested dependent upon the clinical presentation and may include: • renal immunology (ANA, DNA, ANCA, complements, electrophoresis) • urinary biochemistry electrolytes osmolality • ECG • chest x-ray • abdominal x-ray • renal tract ultrasound (ideally within 24hrs if obstruction suspected or esoteric cause suspected requiring a kidney biopsy) • kidney biopsy 8.0 Management of a patient with Acute Kidney Injury 8.1 If the advice is this guideline is followed, the care of patients with AKI can often be undertaken in the non-specialist areas such as acute admission units and general wards. 8.2 The management of AKI in the majority of cases is supportive with treatment of the underlying cause/s. General supportive measures include optimisation of haemodynamic status by appropriate fluid therapy, and treatment of any underlying sepsis. Nephrotoxic medications should be stopped. 8.3 Consider insertion of a central venous pressure (CVP) line and urinary catheter (not mandatory and could introduce infection) to aid with assessment of volume status. 8.4 Resuscitation with intravenous (IV) fluids: • • • Begin with fluid bolus of 500mL (250mL if there is history of cardiac failure or over age 75 years) of crystalloid (sodium chloride 0.9% if hyperkalaemic). Assess for clinical response in terms of: peripheral perfusion pulse (reduction in pulse if tachycardic) rise in jugular venous pressure (JVP) blood pressure (BP) rise pulmonary oedema (presence obviates further fluid) urine output (increasing if oliguric) If there is no clinical response and no pulmonary oedema, administer a further 500mL of crystalloid (250mL if cardiac failure or over age 75 years), and reassess clinically. Discuss case with senior member of team 6 8.5 • If clinical response to fluid bolus is achieved, continue with intravenous fluids until euvolaemia is restored or until independent oral intake is achieved and ongoing fluid losses resolves • If patient remains oliguric (less than 0.3mL per kg per 24 hours) despite adequate volume resuscitation, consider the patient as having volume unresponsive AKI and refer to critical care or renal service as appropriate Review of patient’s medication is mandatory as many cases of AKI are medication related. The following medications should be withheld or given in the presence of AKI or in patients who are at risk of AKI: • • • • 8.6 Monitoring of the patient with AKI is an essential part of patient management. A polyuric phase may develop during the recovery of AKI. Patients are at increased risk of developing negative fluid balance and electrolyte disturbances. The following are required for monitoring patients with AKI: • • • • 8.7 Angiotensin converting enzyme inhibitors (ACE-I) and angiotensin receptor blockers (ARB) Diuretics Non-steroidal anti-inflammatory drugs Aminoglycoside antibiotics – please discuss alternative antibiotics with microbiologist in patients with AKI or in patients with chronic kidney disease stage 3 and above. Regular physiological surveillance (PAR score), frequency depending on clinical severity Fluid balance chart recording all input and output, maintain a positive balance of 500ml Daily weight Daily renal profile and full blood count Post recovery of AKI and post-discharge advice: • • Advise GP to recheck renal function 1 month after recovery of AKI Advice on the judicious and cautious re-instatement of anti-hypertensive medication and ACEI/ARB/diuretics to patient’s GP, with careful monitoring of renal function. This will prevent rebound admissions due to uncontrolled hypertension, and congestive heart failure. 9.0 Referral to specialist services for Acute Kidney Injury 9.1 Not all patients with AKI require specialist input. This is especially the case in prerenal AKI which often responds rapidly to fluid resuscitation, discontinuation of nephrotoxic medication and treatment of underlying sepsis. 9.2 However, when a patient with worsening AKI requires escalation of care, referral to specialist areas such as critical care (ITU, MHDU) or renal service (Terling Ward) will depend on the clinical condition of the patient as reflected by their physiological scores (PAR scores). 9.3 It is inappropriate to refer to the renal service the AKI patient with more than singleorgan dysfunction where it is anticipated that they will require more than renal 7 replacement therapy. For example the septic, hypotensive and respiratory compromised patient with AKI will require critical care referral (ITU) instead of the renal services. 9.4 Specialist renal input is recommended in the following circumstances: • • • • • 9.5 Renal referral procedure • • • • • 9.6 Oliguria and non-response to fluid replacement Stage 3 AKI AKI with intractable hyperkalemia, metabolic acidosis and volume overload where renal replacement therapy is imminently required Suspected esoteric causes of AKI such as vasculitis where urgent pre-sumptive treatment will need to be commenced Non-resolving AKI Referral is addressed to the renal consultant on call of the week Contact Switchboard for renal consultant on call rota Fax referrals to 4426 Do not fax to the Renal Dialysis Unit Bleep renal registrar to inform of the referral, or contact renal consultant on call if registrar not available. Residual chronic kidney disease post-AKI 9.6.1 A significant proportion of patients may have chronic kidney disease that may require long term care and management. Arrangements for outpatient renal clinic follow up should be made prior to patient discharge. This can be done by requesting for outpatient follow up appointment (with a named renal consultant) in the discharge letter on Extramed. 10.0 Training 10.1 Training on the subject of AKI will included in formal junior doctor training programmes as per Mandatory Training Policy (Training Needs Analysis) 11.0 Implementation and Communication 11.1 Once ratified, it is the responsibility of Corporate Services to ensure that the guideline is uploaded to the intranet and website and notified to all staff via Focus. 11.2 The policy will be sent to all Clinical Directors and Corporate Nursing for information and dissemination amongst their teams by the author. 11.3 The guideline will be introduced to junior doctors during their induction programmes. 11.4 The author will be responsible for ensuring that all post ratification communications that are required take place. 12.0 Breaches 12.1 A risk event form should be completed for any instance of non-compliance with this guideline. 8 13.0 Audit and monitoring An annual audit will be carried out to assess compliance with this guideline. This will be done on all patients with severe AKI requiring haemodialysis support. Case notes review will be done on these patients to assess compliance with this guideline. Findings will be presented at Trust audit meetings. 14.0 References 1. Renal Association Acute Kidney Injury Guidelines 2011. http://www.renal.org/Clinical/GuidelinesSection/AcuteKidneyInjury.aspx 2. Clinical guideline on Severe Sepsis 2008. MEHT intranet 9 Appendix 1 Algorithm for the Preliminary Management of Acute Kidney Injury Suspected AKI (3.1) No Continue to monitor for risk of AKI (4.2) Yes • δSCr ≥ 26µmol/L within 48 hours or • δSCr ≥ 1.5 x from a known baseline • presumed to have occurred within one week or • UO < 0.5ml/kg/hr for >6 consecutive hours Hypovolaemia Sepsis Cardiac Insufficiency Staging of AKI (3.2) Correct Hypovolaemia Treat Sepsis Restore cardiac output ACEI,ARB, NSAIDS & Diuretics History, Physical Examination and Lab Tests (4-5) Symptoms + signs of vasculitides Active urine – blood, protein & casts Hypercalcaemia, bony pains Antibiotics, NSAIDs and other meds MAHA, thrombocytopenia Anuria History of renal stones, colic Lower urinary tract symptoms Palpable bladder Urgent renal referral (8) Haemdodynamically stable AKI stage 3 (refer ITU if unstable) Oligoanuria despite resuscitation, and pulmonary oedema Medication review Stop Nephrotoxics Intrinsic AKI suspected Urgent vasculitic screen and renal referral Urgent USS Urgent decompression if obstructed Treat causes of AKI Monitor for complications Intractable hyperkalemia,, uraemic encephalopathy and acidosis Post-discharge care Evidence of vasculitides 10