Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
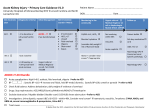
Acute Kidney Injury SUSAN BUDNICK, MD What is an Acute Kidney Injury? AKI is a heterogeneous group of conditions that are all characterized by an acute impairment of renal function, causing an increase in waste products normally filtered by the kidneys All of these conditions are associated with rise in serum creatinine, BUN and (sometimes) decreased urine output (UOP). Divided into 3 broad categories: Prerenal, intrinsic renal and postrenal Why do AKIs matter? AKI is associated with increased risk of mortality, both while in-hospital and long term. Patients with AKI are more likely to die prematurely after hospitalization, even if renal function returns to baseline. AKI is associated with longer hospital stays and increased cost of stay Patients with severe AKI, requiring CRRT or HD are at a high risk of developing progressive CKD and 10% eventually developed ESRD requiring HD. How is AKI defined? A rise in serum creatinine of at least 0.3mg.dL within 4 hours or 50% increase from baseline within 1 week OR A decrease in UOP to <0.5ml/kg lasting longer than 6 hours The RIFLE criteria for kidney injury The RIFLE criteria for kidney injury The RIFLE classification is based on Creatinine and UOP. It includes 3 classes of AKI severity (Risk, Injury and Failure) and 2 classes of post-AKI outcomes (loss of function and ESRD). If UOP and creatinine differ in AKI severity, use the criteria that gives the most severe diagnosis/prognosis. Etiologies of AKI Generally divided into 3 categories: Prerenal: The most common form Intrinsic renal: Either due to direct damage by nephrotoxins or secondary to ATN, ischemia or sepsis (etc.) Postrenal/Obstructive: Obstruction causing increased retrograde hydrostatic pressure that interferes with GFR. Prerenal Azotemia Decreased renal blood flow which causes insufficient hydrostatic pressure for normal GFR Can be due to hypotension, decreased cardiac output and medications that interfere with autoregulation of glomerular blood flow. Can be rapidly reversed with improvement in RBF Prerenal Azotemia Remember this? Common medications (NSAIDs, ACEi/ARBs) can affect RBF by decreasing autoregulatory functions Intrinsic Renal Parenchymal Disease Causes are numerous… TTP/HUS ATN (ischemic or toxic) HTN Sepsis Ischemia- can progress from prerenal azotemia Endogenous toxins (Hb, myoglobin, uric acid, light chain proteins) Nephrotoxic agents DIC Postrenal Obstruction Can occur anywhere from the renal pelvis to the tip of the urethra AKI occurs when either both of the kidneys are obstructed or the unobstructed kidney is dysfunctional. Causes are numerous: BPH, neurogenic bladder, anticholinergics, intraluminal calculi and clots, and compression/damage to normal structures. Diagnostic evaluation Don’t forget your History and Physical! It can give important clues to the etiology of AKI. Hypotension? History of vomiting and diarrhea? New medications? Dry mucous membranes? Do they appear septic? Patterns of Creatinine Rise Contrast induced Nephropathy: Rise in SCr within 24-48 hrs. Peak within 3-5 days and back to baseline in 5-7 days. Prerenal azotemia: A rise in creatinine that downtrend when volume status is corrected. Atheroembolic disease: Typically a subacute rise in SCr (Can be rapid rise and severe in some cases). Nephrotoxic agents like aminoglycosides, carboplatins: Rise in SCr delayed 3-14 days after exposure Diagnostic workup? BUN:Creatinine greater than 20:1 suggest prerenal etiology Urine electrolytes: 𝑈𝑁𝑎 𝑥𝑃𝐶𝑟 𝐹𝑒𝑁𝑎 = 𝑃𝑁𝑎 𝑥 𝑈𝐶𝑟 <1% prerenal, >2-3% intrinsic damage, >4% obstructive Urine sodium is the poor man’s FeNa. If <25, likely retaining sodium due to hypovolemia Renal Ultrasound: Size of the Kidneys: Normal sized kidneys are expected in AKI Kidneys may be nomal size in CKD due to diabetic nephropathy, HIV-associated nephropathy, or infiltrative diseases. Small, shrunken kidneys are suggestive of CKD Enlarged kidneys in a patient with AKI suggests the possibility of acute interstitial nephritis May show obstruction and dilation of the collecting system and hydroureteronephrosis Dopplers may be useful in ruling out renal vein thrombi Kidney Biopsy A biopsy can give diagnostic information when prerenal, postrenal, ischemia and nephrotoxic etiologies are unlikely. Useful in diagnosing glomerulonephritis, vasculitis, interstitial nephritis, myeloma kidney, HUS and TTP, and allograft dysfunction. This procedure carries a risk of serious bleeding, especially when patients are coagulopathic. Complications of AKI Hypervolemia Uremia Uremia poses little direct toxicity at levels below 100 mg/dL. At higher concentrations can cause mental status changes and bleeding Electrolyte abnormalities including hyperkalemia, hyponatremia, hyperuricemia, hyperphosphatemia, hypocalcemia, and hypomagnesemia Metabolic acidosis Cardiac complications can include arrhythmias, pericarditis, and pericardial effusion Indications for Emergent Dialysis AEIOU mnemonic: Acidemia: Persistent academia that is either non-responsive to bicarb or when giving bicarb would result in volume overload Electrolyte abnormalities such as hyperkalemia in setting of EKG changes Intoxications: Salicyclic acid, lithium, isopropanol, magnesium and ethylene glycol Overload Uremia causing complications such as pericarditis, encephalopathy, bleeding Treatment of AKI Treatment depends on the etiology and focuses on treating underlying insult For instance, in setting of post-renal obstruction, relieving the obstruction or in prerenal etiologies such as hypovolemia, correcting the hypovolemia. Patients may need medications renally dose in the setting of AKI. Avoid NSAIDs and consider holding ACEi/ARBs in the setting of acute AKI