Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
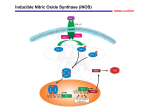
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore ANNEXURE II PROFORMA FOR REGISTRATION OF SUBJECT FOR DISSERTATION 1. NAME OF THE CANDIDATE AND ADDRESS : Dr. AKSHATHA. B.K. POST GRADUATE STUDENT DEPT.OF ORAL AND MAXILLOFACIAL PATHOLOGY AND MICROBIOLOGY, VYDEHI INSTITUTE OF DENTAL SCIENCES AND RESEARCH CENTER, 2. NAME OF THE INSTITUTION: #82, EPIP AREA, NALLURAHALLI POST, WHITEFIELD, BANGALORE-560066. VYDEHI INSTIUTE OF DENTAL SCIENCES AND RESEARCH CENTRE, #82, EPIP AREA, NALLURAHALLI POST, WHITEFIELD, BANGALORE-560066. 3. COURSE OF THE STUDY AND MASTER OF DENTAL SURGERY IN ORAL AND MAXILLOFACIAL PATHOLOGY AND MICROBIOLOGY. SUBJECT: 4 DATE OF ADMISSION TO COURSE 26- MAY-2010 5. TITLE OF THE TOPIC: “EXPRESSION OF INDUCIBLE NITROUS OXIDE SYNTHASE IN ODONTOGENIC KERATOCYST, DENTIGEROUS CYST AND RADICULAR CYST”; AN IMMUNOHISTOCHEMICAL STUDY. 6.0 BREIF RESUME OF THE INTENDED WORK: 6.1 NEED FOR THE STUDY The three most common Odontogenic cysts are Radicular cysts (RCs), Dentigerous cysts (DCs) and Odontogenic Keratocysts(OKCs). Nitric oxide synthases (NOS) are a family of eukaryotic enzymes that catalyze the production of nitric oxide (NO). NOS has three isoforms of which, inducible nitrous oxide synthase (iNOS), is found in various cells including macrophages and natural killer cells in immune system. iNOS is a calcium independent cytosolic enzyme induced mainly by cytokines such as Interleukin-1β, tumor necrosis factor and Interferon-γ (INF-γ) at sites of inflammation. Also, iNOS and VEGF has been shown to play role in cell proliferation, tumor growth, angiogenesis and metastasis. Increased nitric oxide production in OKCs, DCs, and RCs may participate in bone resorption and cystic enlargement. This is because matrix metalloprotienases(MMPs) can be activated by nitric oxide and MMPs play key role in destruction of bone matrix. iNOS plays important role in pathology of both inflammatory and developmental cysts. The epithelial lining cells of OKCs ,DCs, and RCs can produce their own cytokines such as ILα and IL-6; These cytokines may activate iNOS expression of the epithelial cells in autocrine fashion. OKC is now designated by WHO as a “Keratocystic Odontogenic Tumor” (KCOT) because of its aggressive behavior, recurrence risk, and malignant potential. The epithelial lining of OKC appears to have intrinsic growth potential not present in other types of Odontogenic cysts. The present study is to investigate role of iNOS in the pathogenesis of OKCs, DCs and RCs by evaluating the iNOS expression in the epithelial lining of these cysts. 6.2 REVIEW OF LITERATURE: A study was conducted to investigate immunohistochemical expression of iNOS and p53 in OKCs, DCs and RCs and to determine the correlation of these two proteins within each cyst type. The expression of p53 positive cells was significantly found to be higher in OKC when compared to DC and RC; but expression of iNOS positive cells was found to be lower in RC when compared to OKC and DC, hence indicating no correlation between expression of p53 and iNOS in OKCs , DCs and RCs 1. An immunohistochemical Study was conducted to study the expression and distribution of iNOS and heat shock proteins (HSPs) in periapical inflammatory lesions. The results showed increased epithelial staining intensity of iNOS, HSP60 and HSP70 in Radicular cyst compared to periapical granuloma, and residual radicular cyst, suggesting their involvement in inflammatory process and may play a role in the activation and proliferation of lining epithelium, leading to progression of periapical inflammatory lesions2. A study was carried out to determine immunohistochemical correlation of iNOS with the level of inflammation in 30 specimens of periapical cysts. The underlying fibrous connective tissue wall of periapical cysts were inflamed with variable degree of inflammatory cell infiltration; 4 (15%) , 9(30%) and 17(57%) cases present with mild, moderate and severe inflammation respectively. These results showed statistically significant increase of iNOS expression in periapical cysts with higher levels of inflammation when compared to cysts with lower level of inflammatory infiltrate3. Another study was carried out immunohistochemically to investigate the interaction of (IFN-γ) and iNOS producing cells in human radicular cysts . The results revealed that iNOS producing cells were localized adjacent to IFN-γ producing cells and epithelial cells of RCs showed significant levels of iNOS production but not IFN-γ .These data showed that iNOS production could be controlled by autocrine or paracrine effects of IFN-γ producing cells in radicular cysts and might play pivotal role in periapical lesions4. A Study using immunohistochemistry was done to examine the expression of iNOS and Vascular Endothelial Growth Factor (VEGF) in ameloblastoma and to investigate the relationship of this expression to angiogenesis and clinical and biological behavior of the tumor. The results showed that microvessel density counts increased with increasing expression of iNOS and VEGF in ameloblastoma indicating that their expression may be closely related to angiogenesis and invasive biological behavior of ameloblastoma5. 6.3 AIMS AND OBJECTIVES OF THE STUDY: To evaluate expression of iNOS in the lining cells of Odontogenic Keratocyst (OKCs), Dentigerous cyst (DCs) and Radicular cyst (RCs). To compare the iNOS expression in lining cells of OKCs, DCs and RCs. To evaluate the iNOS expression in epithelial lining cells of OKCs to determine its malignant potentiality. 7. MATERIALS AND METHODS: 7.1 SOURCE OF DATA Archived paraffin embedded tissues histopathologically diagnosed as Odontogenic Keratocyst, Dentigerous cyst and Radicular cyst, obtained from the Department of Oral and Maxillofacial Pathology , Vydehi Institute of Dental Science and Research Center, Bangalore. 7.2 METHOD OF COLLECTION OF DATA After obtaining the patient consent, biopsy for routine diagnosis is taken. The specimen is then processed, embedded in paraffin wax and stored at room temperature. Sample size – 60 group 1- Odontogenic Keratocyst(n=20) group 2-Dentigerous cyst(n=20) group 3- Radicular cyst(n=20) INCLUSION CRITERIA Archived tissues histopathologically diagnosed as Odontogenic Keratocyst, Dentigerous cyst and Radicular cyst. EXCLUSION CRITERIA: Systemic diseases. 7.3 METHOD Hematoxylin and Eosin staining will be performed to confirm the clinical diagnosis for OKC, DC and RC. Immunohistochemistry will be done on 4μm thick formalin fixed and paraffin embedded tissue sections mounted on 3- aminopropyl-tri-ethoxysilane(APES) coated slides. Sections will be dewaxed with xylene and rehydrated through graded series of alcohol and finally in distilled water. Sections will be immersed in 0.4% pepsin in 0.01M HCL at 37oC and antigen retrieval will be done using heat induced antigen retrieval method. Blocking will be performed with 3% hydrogen peroxide in absolute methanol for 10 minutes to quench endogeneous peroxidase activity. Washing will be done with phosphate buffered saline ( PBS) .Sections will be incubated with 2% bovine serum albumin for 30 mins to block non specific binding. The sections will be treated with 1:200 dilution of mouse anti-human iNOS monoclonal antibody (biogenex) for 2 hours at room temperature. Sections will be treated with secondary detection system (HRP polymer/ label system) for 30 minutes. The sections will be stained with chromogen 3.3’ diaminobenzidine, counterstained with heamtoxylin and mounted. Phosphate buffered saline will be used throughout for washing and rinsing of slides. Negative controls will be kept with phosphate buffered saline instead of primary antibody. The expression of iNOS in epithelial lining cells of Odontogenic keratocyst, Dentigerous cyst and Radicular cyst will be assessed and data obtained will be compared and statistically analysed. 7.4 STATISTICAL ANALYSIS Statistical analysis will be made using chi- square test. 7.5 DOES THE STUDY REQUIRE ANY INVESTIGATIONS OR INTERVENTIONS TO BE CONDUCTED ON PATIENTS OR OTHER HUMAN OR ANIMALS? IF SO, PLEASE DESCRIBE BRIEFLY. Yes, biopsy specimen of lesional tissue obtained for routine diagnosis will be processed and used. 7.6 HAS ETHICAL CLEARANCE BEEN OBTAINED FROM YOUR INSTITUTION? YES 8. LIST OF REFFERENCES : 1. Poomsawat S, Punyasingh J, Vejchapipat P. Immuno-histochemical Expression of p53 Protein and iNOS in Odontogenic Cysts. J Med Assoc Thai 2009; 92 (7):952-60. 2. Suzuki T, Kumamoto H, Ooya K, Motegi K. Expression of inducible nitrous oxide synthase and heat shock proteins in periapical inflammatory lesions. J Oral Path Med 2002; 31: 48893. 3. Matsumoto MA and Ribeiro DA .Inducible Nitrous Oxide Expression Correlates with the Level of Inflammation in Periapical Cysts Eur J Dent. 2007 October; 1(4):212-215. 4. Takeichi O et al. Inducible nitrous oxide synthase activity by interferon-gamma- producing cells in human radicular cysts. Int endodontic j 1999 ;32:124-130. 5. Chen WL, Ouyang KX, Li HG, Huang ZQ, Li JS, Wang JG. Expression of inducible nitrous oxide synthase and vascular endothelial growth factor in ameloblastoma. J Craniofac Surg. 2009 Jan;20(1):171-5; discussion 176-7 . 9. SIGNATURE OF THE CANDIDATE: 10. REMARKS OF THE GUIDE: 11. 11.1 NAME AND DESIGNATION OF GUIDE: Dr.K.KARPAGASELVI PROFESSOR AND HOD, DEPARTMENT OF ORAL AND MAXILLOFACIAL PATHOLOGY AND MICROBIOLOGY, VYDEHI INSTITUTE OF DENTAL SCIENCES AND RESEARCH CENTER. #82, EPIP AREA, NALLURAHALLI POST, WHITEFIELD, BANGALORE-560066. 11.2 SIGNATURE 11.3 CO-GUIDE: 11.4 SIGNATURE Dr.K.KARPAGASELVI 11.5 HEAD OF THE DEPARTMENT: PROFESSOR AND HOD, DEPARTMENT OF ORAL AND MAXILLOFACIAL PATHOLOGY AND MICROBIOLOGY, VYDEHI INSTITUTE OF DENTAL SCIENCES AND RESEARCH CENTER, #82, EPIP AREA, NALLURAHALLI POST, WHITEFIELD, BANGALORE-560066. 11.6 SIGNATURE 12. 12.1 Remarks of the Chairman and The Principal 12.2 Signature