Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Meningococcal disease wikipedia , lookup
Neonatal infection wikipedia , lookup
Bovine spongiform encephalopathy wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Tuberculosis wikipedia , lookup
Orthohantavirus wikipedia , lookup
Dracunculiasis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Poliomyelitis eradication wikipedia , lookup
Chagas disease wikipedia , lookup
Bioterrorism wikipedia , lookup
Sarcocystis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Gastroenteritis wikipedia , lookup
West Nile fever wikipedia , lookup
Ebola virus disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Trichinosis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Leptospirosis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Henipavirus wikipedia , lookup
Hepatitis B wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Hepatitis C wikipedia , lookup
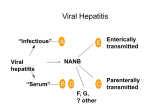
Foodborne Viruses in the European Union Patricia Garvey EPIET fellow Health Protection Surveillance Centre, Dublin Outbreaks of foodborne viral disease, European Union, 2011-2013 •2223 viral foodborne outbreaks reported to European Food Safety Authority (EFSA) between 2011 and 2013 •275 where there was strong evidence implicating a foodstuff •Calicivirus (including norovirus): 260/275 (95%) •Hepatitis A: 10/275 (6 of which were in 2013) •Other viruses: 5/275 Data source: EFSA and ECDC. EU summary reports on zoonoses, zoonotic agents and foodborne outbreaks, 2011, 2012 and 2013 What is Norovirus? •Along with Rotavirus, Norovirus (NoV) is the most common cause of gastroenteritis •AKA 'winter vomiting viruses', 'small round structured viruses' or 'Norwalklike viruses‘ •Belong to a group of viruses called 'caliciviruses'. •Extremely hardy: survives for at least one week on stainless steel and other “touch” surfaces (PC keyboards, light switches, TV remote buttons) What is Norovirus infection? •Incubation period: 12 to 72 hours •Traditional described as a “mild illness”, symptoms include: •watery diarrhoea (>80%), vomiting (75%), abdominal pain (50%), nausea (50%), cramps (45%), Fever (33%), and occasionally, muscle aches and headaches •Duration: •Diarrhoea –5 days •Vomiting persists for 1-2 days •Malaise for 2-3 days. •A minority (usually the very young or elderly) may become very dehydrated and require hospital treatment Surveillance of Norovirus Disease •Notifiable in Ireland (as individual cases and as outbreaks) -1000-2000 notifications annually •Reported cases represent a minority of cases (Tam and O’Brien GUT 2012 estimated that there were 288 cases in community for every case reported to national surveillance in UK ) •Not notifiable at EU level •Member state level surveillance of NoV is useful to describe timing of onset and severity of season compared to other years •Outbreak surveillance useful to understand the relative importance and trends in transmission routes and in settings affected “Notifiable” infectious diseases are those whereby there is a statutory obligation upon all medical practitioners, including clinical directors of diagnostic laboratories, to notify the Medical Officer of Health(MOH)/Director of Public Health (DPH). This list of 80+ diseases are of such clinical/Public Health importance that the information is gathered on them in a systematic manner is used to investigate cases thus preventing further spread Norovirus transmission •Highly contagious and can spread easily from person to person (R0 of NoV ≈ 4.0*) - most outbreaks have an attack rate of >50% Transmission: •Contact with an infected person e.g. when caring for someone with norovirus infection. •Contact with contaminated surfaces or objects and then spread to mouth or mucous membranes via fingers/fomites. •Consuming contaminated food or water •Commonly associated with congregate settings in winter, e.g. hospitals, residential institutions, hotels, schools, etc. *R0= Reproduction Rate; the number of new cases of a contagious disease generated by a single case of that disease (HAV=1.3; Measles = 16) Foodborne transmission •The proportion of NoV illness that is foodborne is difficult to establish •Because of the low severity of illness among healthy individuals, many foodborne outbreaks are not recognised or investigated NoV outbreaks by reported transmission route Ireland 2004-2014 12% 1% 0% •Detection of NoV in food is difficult hampering evidence gathering •Food was reported to have contributed to 1.2% of NoV outbreaks in Ireland 2004-2014 •Other countries with more foodborne-disease oriented surveillance systems have produced higher estimates 87% Foodborne+/- Person to person Waterborne +/- person to person Person to person/airborne Unknown Distribution of food vehicles in foodborne outbreaks with strong evidence caused by calicivirus* in the EU, 2011 Data source: EFSA and ECDC. EU summary reports on zoonoses, zoonotic agents and foodborne outbreaks, 2011 *Is used as a proxy for NoV infection •Numerous NoV outbreaks in Scandinavia linked to frozen raspberries from mid 1990s •Large outbreak of NoV in Germany in 2012 linked to frozen strawberries (>10,000 cases) •Multistate outbreaks of HAV linked to frozen berries in 2013 Tavoschi et al Eurosurv 2015 Hepatitis A virus • Associated with poor hygiene and sanitation - primarily transmitted from person-to-person via the faecal-oral route • Incubation period commonly 28-30 days (range 15-50) • Common source outbreaks due to contaminated food or water also occur • Quite contagious when spread from person to person (R0 HAV= 1.3) • Acute disease – does not have a chronic form. Protective antibodies develop after infection • Vaccine preventable • Clinical severity tends to increase with age. Adults can experience severe illness lasting several months • The most common symptoms are fever, loss of appetite, nausea, fatigue and abdominal pain, followed within a few days by jaundice • In developed countries, hepatitis A is most commonly seen among people who travel to endemic countries, household or sexual contacts of known cases, injecting drug users (IDU) and men who have sex with men (MSM) Geographic distribution of hepatitis A virus infection (Source CDC, Atlanta, USA) Number of notifications of hepatitis A Ireland 1988-2013 Number of notifications 600 564 538 500 432 400 424 367 321 313 309 300 261 218 205 200 133 112 94 100 50 47 55 39 32 42 50 46 26 25 19 30 Year Data source: Computerised Infectious Disease Reporting System (CIDR), HPSC 2013 2012 2011 2010 2009 2008 2007 2006 2005 2004 2003 2002 2001 2000 1999 1998 1997 1996 1995 1994 1993 1992 1991 1990 1989 1988 0 HAV outbreaks notified by transmission route, Ireland 2004-2014 7 Number of outbreaks 6 5 Unknown Person-to-person & waterborne Person-to-person Foodborne 4 3 2 1 0 2004 2006 2007 2008 2009 2010 2012 2013 2014 Year of notification Data source: Computerised Infectious Disease Reporting System (CIDR), HPSC Foods implicated in recent HAV outbreaks internationally Liver paté –France [Schwarz et al Eurosurv 2008] Oysters –France [Guillois et al Eurosurv 2009] Semi-dried tomatoes –Netherlands, England [Petrignani et al. Eurosurv 2010; Fournet et al Eurosurv 2012; Carvalho et al Eurosurv 2012] Raw seafood –Italy [Montano-Ramacha et al Eurosurv Bakery products –Germany [Harries et al Eurosurv 2013] 2014] Pomegranate seeds –Canada [Swinkels et al Eurosurv 2014] Frozen strawberries –Scandinavia [Eurosurv 2014] Strawberries/Mango –European travellers (including Irish tourists) to Egypt [Sane et al 2015] Frozen berries –Multistate including Ireland [Rizzo et al Eurosurv 2013; Severi et al Eurosurv 2015; Fitzgerald et al 2014; Guzman-Herrador et al Eurosurv 2014] May 2013: European alert re HAV outbreak in Italy June 2013: HAV subgenotype IA with an identical sequence identified in Ireland in three cases who had not travelled to Italy In total, 21 outbreak cases (between 31 January and 11 October 2013 Epidemiological evidence implicated frozen berries (linked with different products containing the berries) Sixteen food samples tested were all negative for HAV The public were advised to heat-treat frozen berries before consumption Fitzgerald et al Eurosurv 2014 •Identification of the outbreak •May 2013, Italy declared a national outbreak of hepatitis A •Also affected several foreign tourists who had recently visited Italy •An identical strain of HAV subgenotype IA identified in additional EU/EEA countries •An international outbreak investigation team was convened •Burden of illness •1,589 hepatitis A cases •1,102 (70%) hospitalised • two related deaths Severi et al Eurosurv 2015 •Vehicle of infection: •Mixed frozen berries epidemiological and microbiological evidence •Control measures: •Suspected or contaminated food batches were recalled •the public was recommended to heat-treat berries •post-exposure prophylaxis of contacts •Large food-borne hepatitis A outbreaks may affect the increasingly susceptible EU/EEA general population •With the growing international food trade, frozen berries are a potential high-risk food Severi et al Eurosurv 2015 •14 EU-EFTA countries (including Ireland) reported 107 cases •sub-genotype IB with identical RNA sequences, suggesting a common source outbreak. •Associated with exposure to strawberries or mango •None of the 43 cases interviewed had been vaccinated •Unawareness that HAV vaccination was recommended (23/43, 53%) and perceiving low infection risk in all-inclusive luxury resorts (19/43, 44%) •Recommendation: public health authorities should emphasize the importance of vaccination before visiting HAV-endemic areas, including Egypt Sane et al Eurosurv 2015 At least 103 reported cases A study in Denmark, Finland, Norway and Sweden identified frozen strawberries as the likely cause of the outbreak The origin of the berries was being investigated Guzman-Herrador et al Eurosurv 2014 Hepatitis E (HEV) • Common cause of acute hepatitis worldwide • Traditionally associated with poor hygiene and transmission via the faecal- oral route in endemic regions • Now recognised as an emerging disease in many developed countries -increasing evidence for a rise in locally acquired zoonotic HEV • Increasing number of human cases across Europe • Causes large outbreaks of acute hepatitis in endemic areas and sporadic cases in industrialised countries Clinical aspects of HEV • Incubation period 15 to 64 days • Most HEV infections asymptomatic • Symptoms include fever, fatigue, abdominal pain, nausea, vomiting, loss of appetite and jaundice • Symptomatic infection more common in middle-aged and elderly men • Usually a self-limiting illness -4-6 weeks • In rare cases can be fatal, especially in pregnant women • Persistent infection can occur in persons with suppressed immune systems • Uncertain whether infection confers lifelong immunity • Period of communicability is not known; secondary spread is rare HEV genotypes Reservoirs Distribution Transmission HEV1 and HEV2 HEV3 and HEV4 Humans Humans, pigs, and other mammalian species Developing countries Both developing and developed countries; HEV3 has a worldwide distribution; HEV4 mostly occurs in southeast Asia but recently isolated in European pigs Via contaminated water in developing countries Consumption of raw or undercooked pork or game meat; through occupational exposure to animals, particularly pigs; transmission of HEV through infected blood products has also been reported HEV –non-food risk factors Age: Autochthonous cases in Europe older than imported cases Sex: Higher proportion male in case series of acute cases (but not seroprevalence studies) could be due to higher risk for overt disease rather than infection Co-morbidities: those affecting the liver likely identified due to higher risk of clinical disease rather than infection Pig contact: reported in case studies and in seroprevalence studies [e.g. Chaussade et al J Clin Virol 2013] Having cats/dogs, contact with horses, living in rural areas –in enhanced surveillance studies Human HEV cases linked to food consumption Consumption of processed pork products was associated with HEV infection in England & Wales case control study [Said et al E&I 2014] Case control study in France showed association with pig liver sausage [Coulson et al JID 2010] Spit-roasted piglet. Outbreak in France -independent association with consumption of piglet liver-based stuffing; case, veterinary and environmental strains identical [Guillois et al CID 2015] Cases linked to consumption of wild boar [Kim et al J Clin Virol. 2011; Li et al EID 2005] Cases linked to consumption of deer meat [Tei et al Lancet 2003; Ja Joon et al Clin Mol Hepatol. 2013] HEV at EU level • Not notifiable in humans at EU level • The European Centre for Disease Prevention and Control (ECDC) established an expert group -first meeting in December 2015 • European Centre for Disease Control and Prevention (ECDC) will conduct an inventory of HEV surveillance systems, case definitions, laboratory methods, and epidemiological information across Europe. It is expected that this will contribute to the development of a framework for HEV surveillance SCOTLAND: Laboratory Reported HEV cases by year 2011-2014 (Source: Health Protection Scotland) Number of confirmed cases of HEV 180 •Rate in 2014: 3.0 per 160 140 100,000 120 •Predominantly older 100 males 80 •Some of increase due to 60 40 increased testing but 20 also believed due to real 0 2011 2012 2013 Year of reporting 2014 increase in incidence ENGLAND: Confirmed HEV cases by year 2003-2014 (Source: Public Health England) Number of confirmed cases of HEV 1000 900 800 700 Non-travel 600 associated cases are 500 likely to be older 400 300 men infected with 200 HEV3 (pig strain) 100 0 Year of reporting FRANCE: Annual laboratory reporting HEV from Centre National de Reference (CNR), 2002-2013 2000 Number of laboratory reports 1800 Autochtones Imported 1600 • Increasing number of 1400 samples tested (35,416 1200 in 2013 compared to 1000 800 209 in 2002) 600 • Median age 55 years 400 200 • Predominant genotype 0 3f (57% in 2013) Year of reporting HEV diagnoses at NVRL 2014 •9 laboratory confirmed or probable cases of acute or chronic HEV in Ireland, 5 of which were RNA positive •4 had no history of travel abroad •4 were genotype 3 2015 Jan-Jun 4 cases of viraemic HEV with no history of travel abroad •A decision was taken that from June 2015, all serum samples tested for hepatitis A virus IgM at NVRL would automatically be tested for HEV •Samples found to be positive for HEV IgM would be tested for HEV RNA Personal communication: Dr Joanne O’Gorman, NVRL Personal communication: Dr Joanne O’Gorman, NVRL June 2015 HEV to become a notifiable disease in Ireland Proposed case definition - Hepatitis E (acute and chronic) infection Clinical criteria: Not relevant for surveillance purposes Laboratory criteria: Acute case At least one of the following two: •Hepatitis E virus IgM and IgG antibody positive •Detection of hepatitis E virus RNA Chronic case Hepatitis E virus RNA persisting for at least 3 months Epidemiological criteria: Not relevant for surveillance purposes Case classification •Possible case: N/A •Probable: N/A •Confirmed case: Any person meeting the laboratory criteria Acknowledgements Dr. Lelia Thornton, HPSC Dr. Paul McKeown , HPSC Ms Niamh Murphy , HPSC Dr. Joanne O’Gorman, NVRL Thank you for your attention