Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Xenoestrogen wikipedia , lookup
Menstrual cycle wikipedia , lookup
History of catecholamine research wikipedia , lookup
Neuroendocrine tumor wikipedia , lookup
Endocrine disruptor wikipedia , lookup
Breast development wikipedia , lookup
Mammary gland wikipedia , lookup
Glycemic index wikipedia , lookup
Bioidentical hormone replacement therapy wikipedia , lookup
Hyperthyroidism wikipedia , lookup
Hyperandrogenism wikipedia , lookup
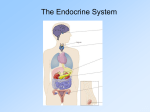
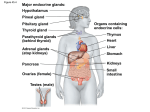
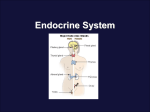
ANATOMY & PHYSIOLOGY I Lecture #20: Selected Endocrine Glands * Refer to the table from Lecture 19 for a complete list of the glands and hormones to KNOW FOR TEST 6. I. Hypothalamus – one of the many things the hypothalamus does is to regulate the pituitary gland. It does this by: A. Secretion of releasing and inhibiting hormones, which control the activity of the anterior pituitary. B. Production of oxytocin and antidiuretic hormone (ADH), which are stored in the posterior _ pituitary. C. Neuroendocrine reflexes, which stimulate release of these hormones from the posterior pituitary. II. Pituitary Gland (or Hypophysis) A. Location – sits in hypophyseal fossa of the sella turcica, attached to the hypothalamus by the infundibulum. B. Structure – a pea-shaped gland about ½ inch in diameter. - Two distinct parts: 1. Anterior lobe (adenohypophysis) - Derived from glandular epithelial tissue - Forms anterior 2/3 of the gland - Linked to the hypothalamus by a portal blood system. 2. Posterior lobe (neurohypophysis) - Derived from nervous tissue that is an extension of the diencephalon. - Forms posterior 1/3 of gland. - Linked to hypothalamus by nerve fibers of the infundibulum. C. Hormone Secretion 1. Anterior pituitary – produces its own hormones and secretes them in response to releasing and inhibiting hormones from the hypothalamus. Many are tropic hormones that control other glands. For this reason the pituitary is sometimes called the “master gland.” a. Growth hormone (GH or somatotropin) – stimulates growth, mainly by promoting uptake of amino acids into cells and their incorporation into proteins. It also promotes the use of fats as a fuel, thus sparing glucose for use by the brain. Too little GH causes: Pituitary dwarfism in children Progeria in adults (premature aging due to tissue atrophy; rare). 2 Too much GH causes: Gigantism in children. Acromegaly in adults (thickening of bones and growth of soft tissues; but long bone growth cannot occur due to ossification of the epiphyseal discs). b. Thyroid-stimulating hormone (TSH or thyrotropin) – stimulates the thyroid gland to make and release thyroxine and triiodothyronine. c. Adrenocorticotropic hormone (ACTH) – stimulates the adrenal cortex to secrete glucocorticoids, such as cortisol. d. Prolactin – stimulates development of the breasts and production of milk in females. High levels are secreted just prior to birth of a baby and in response to suckling. e. Follicle-stimulating hormone* (FSH) – in females, FSH stimulates development of the ovarian follicles, which produce estrogen. In males, it stimulates sperm production. f. Luteinizing hormone* (LH or ICSH) – in females, LH stimulates ovulation and conversion of the ruptured Graafian follicle into the corpus luteum, which secretes progesterone. In males, LH is sometimes called interstitial cell-stimulating hormone (ICSH) because it causes the interstitial cells of the testes to produce testosterone. *Together FSH and LH are referred to as gonadotropic hormones 2. Posterior pituitary – stores the hormones ADH (also called vasopressin) and oxytocin, which are produced in the hypothalamus, and releases them in response to neural signals from the hypothalamus. a. Antidiuretic hormone (ADH or vasopressin) – stimulates the kidneys to retain water so that less is excreted in the urine and more is retained in the blood. In high levels it also causes vascular constriction which increases blood pressure, hence the name vasopressin. ADH is secreted when osmoreceptors in the hypothalamus sense an increase in the blood sodium concentration (which signals that the blood is becoming too concentrated and more water should be retained). Too little ADH results in diabetes insipidus, which causes an individual to suffer from excessive urination, excessive thirst, and severe ionic imbalances. b. Oxytocin – in females it stimulates contractions of the uterus during labor and milk ejection from the mammary glands during lactation. It has no known function in males. It is released in response to neural signals caused by pressure on the cervix (producing a positive feedback loop) and suckling by the infant. 3 To Do: Next to each hormone, indicate whether it is secreted by the anterior (A) or posterior (P) pituitary. A a. Adrenocorticotropic hormone A e. Luteinizing hormone P b. Antidiuretic hormone P f. A c. Follicle-stimulating hormone A g. Prolactin A d. Growth hormone A h. Thyroid-stimulating hormone Oxytocin Use the letters from the list above to match the hormones with their actions. B Stimulates kidneys to retain water and causes vascular constriction. D Stimulates growth by uptake and incorporation of amino acids; helps spare glucose. G Stimulates development of the breasts and production of milk in females. E In females it stimulates ovulation, in males it stimulates testosterone production. A Stimulates the adrenal cortex to secrete glucocorticoids. C Stimulates development of ovarian follicles in females and sperm production in males. F Stimulates contraction of the uterus and milk ejection in females. H Stimulates production and release of thyroxine and triiodothyronine. III. Thyroid Gland A. Location – in the anterior neck, inferior to the larynx. It is made up of two lobes lying on either side of the trachea, connected across the front by a broad isthmus. B. Structure – consists of numerous thyroid follicles, round structures that make and store thyroxine and triiodothyronine. These are surrounded by parafollicular cells, which make calcitonin. C. Hormones 1. Thyroxine (T4) and triiodothyronine (T3) – the hormones are composed of two tyrosine amino acids with either 4 or 3 iodine atoms attached. Function: These hormones have a wide range of effects. They stimulate protein synthesis in most cells and to a large extent determine a person’s basal metabolic rate. Too little thyroxine causes: Cretinism in infants (stunted growth, abnormal development, and mental retardation) Myxedema in adults (low metabolic rate, lethargy, and edema) Endemic goiter (enlargement of the thyroid gland) results if the low levels are due to a lack of iodine. Too much thyroxine causes: Grave’s disease – an autoimmune disease that causes over-stimulation of the thyroid. Results in high metabolic rate, weight loss, and protrusion of the eyes (exophthalmos). 2. Calcitonin – lowers blood calcium levels by stimulating osteoblasts to form new bone matrix. Works in opposition to parathyroid hormone. It seems to mainly be important during childhood. 4 IV. Parathyroid Glands A. Location – four small, rounded glands on posterior surface of the thyroid gland. B. Parathyroid hormone – increases blood calcium level by stimulating osteoclasts to break down bone and other systems to conserve calcium. Works in opposition to calcitonin. V. Adrenal Glands (Suprarenal Glands) A. Location – two glands which sit just above and medial to each kidney. B. Structure – roughly pyramid-shaped with an outer cortex and inner medulla, which function as separate glands. C. Adrenal Cortex 1. Composed of glandular epithelium. 2. Regulated by adrenocorticotropic hormone (ACTH) from the anterior pituitary and humoral mechanisms (concentration of sodium and potassium in the blood). 3. Hormones of the adrenal cortex: a. Mineralocorticoids (aldosterone) – control sodium and potassium balance. b. Glucocorticoids (cortisol) – increase blood glucose levels by stimulating its formation from amino acids (gluconeogenesis), help the body resist stress, and inhibit inflammation and immune system functions. Too few glucocorticoids results in: Addison’s disease (hypoglycemia, sodium and potassium imbalance, dehydration, rapid weight loss, and general weakness). Fatal if not treated rapidly. Too many glucocorticoids results in: Cushing’s disease (hyperglycemia, hypertension, and muscular weakness). Usually caused by an adrenal tumor or overuse of steroidal drugs. c. Gonadocorticoids (androgens and estrogens) – these are sex hormones, but the amount secreted is usually very small compared to that secreted by the ovaries or testes. D. Adrenal Medulla 1. Derived from the same fetal tissue as the nervous system. 2. Regulated directly by nerve stimulation from the sympathetic nervous system. 3. Hormones – epinephrine and norepinephrine trigger the fight-or-flight response along with the sympathetic nervous system, but the hormonal effects last 10 times longer than the effects of nervous stimulation alone. 5 To Do: Next to each hormone, indicate whether it is secreted by the thyroid (T), parathyroid (P), adrenal cortex (C), or adrenal medulla (M). T a. Calcitonin C e. Mineralocorticoids M b. Epinephrine and norepinephrine P f. C c. Glucocorticoids T g. Thyroxine and triiodothyronine C d. Gonadocorticoids Parathyroid hormone Use the letters from the list above to match the hormones with their actions. D Sex hormones secreted by the adrenal gland. E Hormones that control sodium and potassium balance. G Stimulate protein synthesis and determine a person’s long-term metabolic rate. B Help trigger the fight-or-flight response. F Increases blood calcium level by stimulating osteoclasts. A Decreases blood calcium level by stimulating osteoblasts. C Raise blood glucose level, help resist stress, and inhibit inflammation and the immune system. VI. Pancreas A. Location – posterior to the stomach, extends from the duodenum (on the right side of the stomach) to the spleen (on the extreme left side of abdominal cavity). B. Structure – soft, lobular tissue with groups of endocrine cells called islets of Langerhans interspersed in exocrine tissue, which makes digestive enzymes. Thus the pancreas is both an endocrine gland and an exocrine gland. C. Hormones 1. Insulin – decreases blood glucose levels when they are too high by promoting glucose uptake into cells and storage as glycogen or conversion to fat. Also stimulates amino acid uptake, protein synthesis and fat storage. Acts in opposition to glucagon. Too little insulin causes: Diabetes mellitus – characterized by high levels of glucose in the urine and blood. Type I (insulin –dependent or juvenile onset) is caused by destruction of the cell in the pancreas that make insulin (beta cells). This accounts for about 10 % of all cases. Type II (non-insulin-dependent or adult onset) is caused by decreased tissue sensitivity to insulin. Accounts for about 90 % of all cases. Because insulin also affects lipid and protein metabolism, diabetes mellitus has wide-ranging effects, including acidosis. A deficiency of insulin can quickly lead to coma and death. 6 2. Glucagon – increases blood glucose levels when they are too low by stimulating conversion of glycogen to glucose and formation of new glucose from amino acids (gluconeogenesis). Opposes the effects of insulin. * Refer to the table from Lecture 19 for other tissues that have an endocrine function and the hormones they produce. To Do: Indicate whether each statement best applies to insulin (I) or glucagon (G). G Increases blood glucose level I Decreases blood glucose level G Stimulates formation of new glucose from amino acids G Released when the level of glucose in the blood is too low I Released when the level of glucose in the blood is too high I Promotes glucose uptake into cell and storage as glycogen or conversion to fat G Stimulates conversion of glycogen to glucose I Stimulates amino acid uptake and protein synthesis Match each hormonal imbalance with its cause. F Cushing’s disease a. Too little growth hormone C Cretinism b. Too much growth hormone A Pituitary dwarfism c. Too little thyroxine (use twice) E Addison’s disease d. Too much thyroxine D Grave’s disease e. Too few glucocorticoids G Type I diabetes f. C Myxedema g. Too little insulin B Acromegaly h. Too much insulin Too many glucocorticoids Learning Objectives for Lecture #20: Selected Endocrine Glands After studying this material you should be able to: 1. Describe the role of the hypothalamus in regulating activity of the anterior and posterior lobes of the pituitary. 2. Describe the structure of the pituitary gland, including the types of tissue that compose each of the two lobes. 3. List the hormones secreted by each lobe of the pituitary gland and their function. 4 Describe the location and structure of the thyroid, parathyroid, adrenal gland, and pancreas. 5. List the hormones secreted by each gland above, their functions, and the factors that regulate their secretion. 6. Know the disorders that result from too much or too little of the following hormones: growth hormone, antidiuretic hormone, thyroxine, glucocorticoids, and insulin. 7. List the hormones produced by the testes, ovaries, pineal gland, thymus, stomach, small intestines, heart and kidney (see table from Lecture 19).