Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
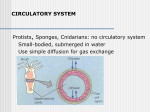
Lecture 15: Depolarization cells and heart There are two different types of cardiocytes (heart cells) in the heart. The first type is depolarizing cells The second type is contractile cells. The contractile cells are large, they branch, and they are connected to each other by a special gap junction, a type of desmosome, called an intercalated disc. These discs allow the cytoplasm from one cell to mix with the cytoplasm with the adjacent cell. If one cell starts an action potential, the electrical current (movement of ions) can rapidly move to the next cell and the next cell. That means that, if a specialized cell can start an action potential, the action potential will spread to all the cells connected to it. They behave as if they were one big cell. And what can we say about the rate of the action potential in a big cell compared to a little cell? The action potential is conducted more quickly in a big cell. In the heart, the two types of cells are connected. One of them can start an action potential. In muscle, and action potential leads to a mechanical event (contraction). The specialized cells that start an action potential can contract, but they are weak. They need to be connected to the contractile cells, which are bulky, and have a lot of myofilaments. But the contractile cells cannot start the action potential. What would happen if the electrical event moved throughout the heart simultaneously? All four chambers would contract, and blood would not move. You have to have a change in pressure in order to have a change in volume. When you squeeze a water bottle, the pressure is increased, and water moves up and out of the bottle. If the pressure across a valve is equal and opposite, the valve cannot open. The chambers have to time their contraction. The atria contract first, creates more pressure, so the AV valve can open, so blood goes into the ventricles. Then the ventricles contract from the apex upward, and the blood will be pushed superiorly. That closes the AV valve so the blood is not regurgitated back the way it came. The pressure will also cause the semilunar valves to open, allowing the blood to move into the pulmonary trunk or the aorta. We need the different parts of the heart to experience the action potential at different times. We need another anatomical structure in the heart to keep the whole organ from depolarizing at the same time. The structure is the fibroskeleton of the heart, called the atrio-ventricular septum. It is fibrous connective tissue, so it is not a good conductor of electricity. The atria depolarize first, and the current quickly moves through all the intercalated discs, and it moves downward and to the left. So the atria are depolarized and they contract. While they are contracting, the electrical current is having a hard time getting through the AV septum. It cannot go around it; it has to go through it, and there is only one little spot where it can get through. At that location are specialized cells. By the time the electrical current can get through the AV septum, the atria have finished contracting and are starting to relax. Now the ventricles experience the action potential and they contract. It is perfect timing of the atria contracting, then the ventricles contracting, then a long period of relaxation before the atria contract again. This timing is called atrial syncytium, followed by ventricular syncytium. It allows oneway movement of blood, by following the rule that pressure and volume is inversely related. When you increase the pressure in the atria, the blood goes into the ventricles. When you increase the pressure in the ventricles, the blood is ejected out of the heart. The blood goes in those directions because of the valves. Review of Heart Muscle • Cardiocytes, myocardium • Branched cells • Intercalated discs- (desmosomes) and electrical junctions (gap junctions). • Has actin and myosin filaments • Has low resistance (1/400 the resistance of cell membrane) • Atrial syncytium (contraction of the atria) • Ventricular syncytium (contraction of the ventricles) • Fibrous insulator exists between atrium and ventricle (what would this do to any electrical activity trying to go through?) If the electrical signals from the atria were conducted directly into the ventricles across the AV septum, the ventricles would start to contract at the top (base). Then the blood would be squeezed downward and trapped at the bottom of the ventricle. The apex to base contraction squeezes blood toward the arterial opening at the base of the heart. The AV node also delays the transmission of action potentials slightly, allowing the atria to complete their contraction before the ventricles begin their contraction. This AV nodal delay is accomplished by the naturally slow conduction through the AV node cells. (Why are they slow conductors? Small diameter cells, fewer channels. Refer to text) The specialized cells are not very abundant, unlike the contractile cells. Be able to describe the direction of flow of current. It starts in the right atrium, and goes down and to the left. Then it arrives in the IV septum, and the current moves around the lateral walls of the ventricle. If you have to pick one direction to describe the movement of current, which wall is thickest? The left. So overall, the movement of current is to the left. It carries more electrical current. The specialized cells of the heart have names like the sinoatrial (SA) node, the atrioventricular (AV) node, the Bundle of His, the right and left bundle branches, and Purkinje fibers. These special cells generate their own action potential. The heart is innervated by the ANS but it does not require it to beat. These cells create autorhymicity. They have VGCs that they can open on their own. How can they reach threshold on their own? Gene expression: they can make themselves more positive by trapping K in the cell, open Na channels. They do both of these. They have more Na and fewer K channels. These cells constantly migrate toward threshold, reach their action potential, depolarize, then repolarize. They do not have resting membrane potentials. They are never at rest. They repolarize and start toward AP immediately. If you detach a heart and put it in isosmotic solution with glucose and keep it chilled, it can beat for quite some time: it can remain alive on a plane from New York to LA to be used in a heart transplant. • • • Fibers within the heart Specialized Fibers – Are the fibers that can spontaneously initiate an AP all by themselves! – The AP will spread to all other fibers via gap junctions – AKA “leading cells” – But they are also muscle, so they do contract, albeit feebly! – They are not nerves!!!! Contractile Fibers – These maintain their RMP (resting membrane potential) forever, unless brought to threshold by some other cell – – – They cannot generate an AP by themselves AKA “following cells” But they do have gap junctions, so once they’re triggered, they will help spread the AP to neighbors. Pathway of Heartbeat • Begins in the sinoatrial (S-A) node • Internodal pathway to atrioventricular (A-V) node • Impulse delayed in A-V node (allows atria to contract before ventricles) • A-V bundle takes impulse into ventricles • Left and right bundles of Purkinje fibers take impulses to all parts of ventricles Sinus Atrial (SA) Node • Specialized cardiac muscle connected to atrial muscle. • SA node acts as pacemaker because they reach threshold the fastest; membrane leaks Na+ and membrane potential is -55 to -60mV • When membrane potential reaches -40 mV, slow Ca++ channels open causing action potential. • After 100-150 msec Ca++ channels close and K+ channels open more thus returning membrane potential toward -55mV. • If the SA node fires 60-80 times a minute, that would be your heart beat. If the SA node failed and you relied only on your AV node, your heart would only beat 40-50 times a minute. That will keep you alive, but you cannot exercise. If both nodes fail, have to rely on your right bundle branch or Perkinje fibers to spread the action potential. That would give you about 15-40 beats per minute; you need a pacemaker. When someone has a myocardial infarction, it can disrupt the electrical impulses in the heart, and they may fire at the same time, not communicating, and the heart beat is called fibrillation, blood is not flowing. Need a defibrillator to reset the normal electrical rhythm. When the SA node reaches threshold, the AP travels through intermodal pathways, going from the top of the right atrium to the bottom left side of the atrium. Internodal Pathways • Transmits cardiac impulse throughout atria • Anterior, middle, and posterior Internodal pathways • Anterior interatrial band carries impulses to left atrium. Atrio-ventricular node (AV) Node • The AV node is an area of specialized tissue between the atria and the ventricles of the heart. • It is called the ventricular pacemaker • It conducts impulses from the atria to the Bundle of His Bundle of His (Av bundle) • The Bundle of His is the fibrous connective tissue that makes up the fibrous septum. • It is the only conducting path between atria and ventricles • Located in the right atria, on top of the AV septum. The cells here are small in diameter, so they conduct electrical impulses slowly. This allows the atria to contract while the AV node is delaying transmission of current to ventricles. • Time delay of 0.04sec • The Bundle of His then branches into left and right bundles that run along the IV septum Purkinje Fibers • The bundle branches give rise to thin filaments known as Purkinje fibers. These fibers distribute the impulse to the ventricular muscle. • Once impulse reaches Purkinje fibers, the conduction is fast Summery The bundle of His, also known as the AV bundle or atrioventricular bundle, is a collection of heart muscle cells specialized for electrical conduction that transmits the electrical impulses from the AV node (located between the atria and the ventricles) to the point of the apex of the fascicular branches. The fascicular branches then lead to the Purkinje fibers which innervate the ventricles, causing the cardiac muscle of the ventricles to contract at a paced interval. Once we are through the Bundle of His, then we have cells that carry the action potential around the lateral walls of the ventricles. Those are Purkinje fibers, they are huge, so the current will speed up. The IV septum receives the electrical impulse before the lateral walls of the ventricle. The IV septum contracts first. That means the apex of the heart is pulled superiorly, so the blood starts to rise, and the pressure on the IV valves causes them to close. Next, the walls of the lateral ventricles depolarize, and they are thick. When they contract, it opens the semilunar valves, and the blood is ejected. What would happen if the sides contracted first? The blood would be pushed down. How can these specialized fibers spontaneously “fire?” • Can’t hold stable resting membrane potential • Potentials drift (gradual depolarization) –”prepotential” or “pacemaker potential” • During this time, they have a gradually increasing perm to Na+ and less leaky to K+ (more “+” inside causes cell to depolarize, remember?) They have different gene expression than the contractile cells. They don’t have as many K channels, they have more Na channels, they allow more positive charges to accumulate in the cell, reach threshold sooner. The slow rise to threshold is called a pre-potential. They have this instead of resting membrane potential. The pr-potential is caused by sodium entering the cell and K being trapped in the cell. What does the AP look like for a specialized cell? See photo below. The prepotential means the inside is becoming more positive. Once it has reached threshold, it does not have Na VGC like in skeletal muscle. It has calcium VGCs. Calcium comes into the cell during an action potential. It comes across the cell membrane, not from the endoplasmic reticulum. During the AP, the cardiac cell can start to contract right away, unlike skeletal muscle, where Ca is released after the cell has been excited, and there is a time delay between the time that the cell has been excited and the release of calcium and you see contraction. The upstroke seen in the AP is caused by an external source of calcium entering the cell. This will also trigger a release of calcium from inside the cell. This will allow for two unusual things in a cardiac muscle (unlike skeletal): 1) The AP lasts for a long time 2) Contraction occurs during the AP This happens because of the source of calcium being external. Once the AP is reached, it needs to repolarize. The K channels open, and the cell repolarized, then experiences a prepotential again. Unlike the specialized cells, contractile cells have a negative RMP, and it is stable. They would stay at RMP indefinitely if it weren’t for the intercalated discs, which allow electrical signals to transmit to them. Contractile cells also have a plateau at the top, means that more calcium in entering the cell, and the contractile cell is creating its greatest force of contraction during the plateau phase. Specialized fibers • Specialized fibers of conductive system • Each region generates its own rhythm. • If cells didn’t touch, then…. • Faster at SA vs. AV node, etc. • SA is faster than AV- “pacemaker” – SA 60-80 depol/min – AV 40-60 depol/min – Purkinje 15-30 depol/min The nerves in the heart are extensions of the sympathetic and parasympathetic nervous system When the sympathetic nervous system releases epinephrine on the beta-1 adrenergic receptors, this alters the prepotential flow by making it steeper. If the parasympathetic nervous system releases Ach on the mACh receptor on the heart, the SA node prepotential will be flatter. During sympathetic stimulation, more K channels are shut down, more positive charges are inside cell, it reaches potential faster, and contracts. The parasympathetic nervous system increases K permeability, making the inside of the cell less positive, and it takes longer to reach threshold. The primary way the ANS alters heart rate is by altering K permeability. Specialized fibers of conductive system • These rhythms can ALSO be modified by the ANS • NTS can change slope of prepotentials…faster or slower rise to threshold (bringing them closer or further from threshold) by altering ion permeability. • ACh (psymp postganglionic); NE (symp postganglionic) • Sympathetic and Parasympathetic • Sympathetic – speeds heart rate by Ca++ & Na+ channel influx and K+ permeability/efflux (positive chronotropy) • Parasympathetic – slows rate by K+ efflux & Ca++ influx (negative chronotropy) Terminology: Chronotropy (refers to time), Inotropy (refers to force of contraction) A sympathomimetic drug will increase ionotropy and ionotropy. HR and force would both increase. This is represented as (+, +) The parasympathetic system slows the heart rate and has little to no effect on the force of contraction. This is represented as (-, ) The para can reduce HR. Do we want it to reduce force of contraction? No. There has to be a finite amount of force to get the stoke volume needed. So the parasympathetic division has no effect on ionotropy. Other effect of ANS • Symp (NE) also affects Inotropy in ALL fibers, specialized and contractile • Inotropy is the “force of contraction” or the tension development in the muscle fiber (strength of the contraction.) • Sympathetic firing causes positive ionotropy! (the pounding heart) • Parasympathetics have little effect on ionotropy Where is the pacemaker of the heart? Top right atrium. Spreads down and across the IV septum, then the bottom part of the left atrium is the last part to depolarize. It enters the ventricles by the AV node. The IV septum depolarized first. The blood is pulled superiorly. Then the lateral walls of ventricles depolarize and contract, ejecting the blood. Electrical events can be monitored. If the inside of the cell is negative at rest, the outside is positive at rest. Know when the inside and outside of the cell is positive and negative. Spread of depolarization At rest, the outside of cells are positive, negative on the inside. Make inside positive, AP triggers and outside is negative. At repolarization, inside becomes positive again. How do the atria depolarize? Top right to bottom left. The cells at the bottom left hold on to their surface charge the longest. They stay at rest the longest. They will be the last ones to spike an AP. The AP for contractile cells look like this: steep polarizing current, then plateau, then steep drop off. It looks very different than AP of skeletal muscles. There is only one way through the AV septum: through the Bundle of His. Then we have the right and left bundle branches. The left branch goes straight down the IV septum, but the right bundle goes up first, then it goes down the IV septum. Because the right bundle takes a detour, the left side of the IV septum will lose its positive charge faster than the right side. It will contract faster. The area of the IV septum that holds onto the positive charge the longest, it would be at the top right area of the ventricle. The left ventricle is thicker, so the current will take longer to get through myocardium to get to the epicardium there. The side that stays at rest the longest is the left side of the left ventricle on the top of the lateral wall of the left ventricle. If the IV septum depolarizes first, apex is pulled up, AV valve closes, contraction, and blood is ejected. Do you want it to repolarize first? No, the blood will fall down. Have to relax the lateral walls first. The first cells to depolarize at the top of the IV septum are the last to repolarize. They will hold onto their contraction the longest. The cells to depolarize last will be the first to repolarize. Regulators of the Heart: Reflex Controls of Rate • Your HR at any moment is the balance between symp and parasym discharge rates. (“tone”/ reserve) • Tonic discharge • How to speed up? Two ways (faucet analogy) • How to slow down? Two ways • Range: about 50 – near 200 • Typical resting HR: near 70 --SA would normally beat at 60-80 bpm- but vagal tone slows it down. Parasympathetic slows-down (20bpm or even stop)• Sympathetic speeds-speed up (230bpm) Contractile Fibers of Heart • Bulk of heart mass • Review APs – Still need calcium to initiate contraction • Differences from Skeletal Muscle and neurons – Nature of AP – Source of calcium (EC vs. SR) – Duration of contraction – Resting potential The contractile cells start to repolarize during absolute refractory period. After relative refractory period, cell has gone back to almost complete relaxation. After calcium is removed, cell starts to relax. In skeletal muscle PhysioEx, you could not hit the button fast enough to create tetani (sustained contraction) because skeletal muscle recovers so fast. Cardiac muscle does not reach its action potential so fast. Important things to consider • Cardiac muscle cells have a long absolute refractory period • Twitches cannot summate • Tetanus not possible (this is good!) • If average heart beats 72bpm; what does the heart do for the rest of the time? • Answer : It “rests” and fills