Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pulmonary Atresia with Ventricular Septal
Defect*
Selection of Patients for Systemic-to-Pulmonary
Artery Shunt Based on Echocardiography
Bruno Marino, M.D.; Luciano Pasquini, M.D.; Paolo Guccione, M.D.;
Salvatore Giannico, M.D.; Maurizio Bevilacqua, M.D.; and
Carlo Marcelletti, M.D.
From January 1987 to December 1988, in 22 infants with
PAVSD, the diagnostic results obtained with echocardiography (two-dimensional, Doppler, and color) were prospectively compared to the angiocardiographic findings. We
classified into group 1 patients with confluent and goodsized pulmonary i -:<mm) arteries, single ductus arteriosus,
and normal pulmonary venous connections ("favorable
pattern"). The other patients with PAVSD were classified
into group 2 ("unfavorable pattern"). The intracardiac
anatomy, the morphology of the pulmonary arteries, and
the pattern of pulmonary blood supply and pulmonary
venous connection were correctly identified with echocardiography in all but one patient, who was erroneously
considered to be in group 2. No false-positive of the
"favorable pattern" (group 1) was detected. Echocardiog
The
pulmonary artery morphology, the blood sup
ply to the lungs, and the pulmonary venous
connections are variable in children with PAVSD. In
fact, in about 50 percent of these patients, the pul
monary arteries are nonconfluent, and the pulmonary
circulation is supplied by MCA.1'5 Palliative operations
in cyanotic infants have been recently reported on the
basis of 2DDE,6-7 but the selection of patients tends
to exclude the subjects with PAVSD because of their
variability of pulmonary artery morphology and pul
monary blood supply. We prospectively studied with
2DDE and angiocardiography
22 consecutive infants
with PAVSD in order to assess the reliability of the
noninvasive method to identify (1) the intracardiac
anatomy and segmental combination, (2) the pulmo
nary artery anatomy, (3) the pattern of blood supply
to the lungs, and (4) the pulmonary venous connec
tions.
MATERIALSAND METHODS
From January 1987 to December
1988, some 22 consecutive
infants with PAVSD were admitted to our department.
The pro
spective study included 2DDE and cardiac catheterization
with
*From the Department of Pediatric Cardiology and Cardiac Surgery,
Bambino Gesu Hospital, Research Institute, Rome, Italy.
Manuscript received March 19; revision accepted June 6.
Reprint requests: Dr. Marino, Pzza S Onvfrio 4, Romt-, Italy 00165
raphy is an effective tool in infants with PAVSD, in order
to discriminate cases with "favorable" and "unfavorable"
patterns of pulmonary arteries, pulmonary blood supply,
and pulmonary veins. The first group with the "favorable
pattern" may be considered for systemic-to-pulmonary
shunt surgery without angiocardiography. Based on this
experience from January to December 1989, four patients
with this "favorable pattern" underwent a successful sys
temic-to-pulmonary
artery shunt with an echocardiographic diagnosis alone.
(Chest 1991; 99:158-61)
PAVSD = pulmonary atresia with ventricular septa! defect;
MCA = major collateral arteries; 2DDE = two-dimensional and
Doppler echocardiography
angiocardiography.
The age ranged from 1 to 78 days (mean, 19
days); 12 patients were boys and 10 girls. The detailed diagnoses
are reported in Table 1.
Echocartlivgraphy
The study was performed with a sector scanner (Hewlett-Packard
77020) using a 5.0-MHz transducer with pulsed-wave Doppler and
with a separate multifrequency
continuous-wave
Doppler trans
ducer. A complete assessment was obtained in each patient; in
particular, the morphology and the size of the pulmonary arteries,
the pattern of the pulmonary blood flow, and the pulmonary venous
connections were delineated according to previous reports by using
suprasternal, parasternal,"1- and subcostal13 views. The last 12 cases
were investigated also with color Doppler echocardiography.'* Our
2DDE analysis was finalized to delineate the intracardiac anatomy
and to recognize the patients with the following features: (1)
confluence of the pulmonary arteries and diameter of each pulmo
nary artery a3 mm; (2) single ductus arteriosus as the only source
of pulmonary blood flow; and (3) normal pulmonary venous connec
tions. The patients with all of these characteristics were defined as
having a "favorable pattern" (group 1). The children without one of
the previously mentioned elements were included in the group with
an "unfavorable pattern" (group 2). The criteria for this classification
are summarized
in Table 2.
Angfoca rdiography
The cardiac catheterization
was performed within one to seven
days after the 2DDE study. Each patient had a right or left
ventricular injection (or both) to confirm the diagnosis of PAVSD
and the intracardiac anatomy. All patients underwent aortography,
with or without balloon occlusion," and three also had pulmonary
venous wedge angiography1" to demonstrate the blood supply to the
158
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21623/ on 05/03/2017
Pulmonary Atresia with VSD (Marino et al)
Table I—Diagnostic Results with 2DDE and Angiography
in 22 Patients with PAVSD*
were confirmed at catheteri/ation
and angiocardiog
raphy in all infants. In all patients the cardiac cathe
teri/ation and angiocardiography
revealed the pul
DiagnosisCase12345678910111213141516171819202122AssociatedMalformationAorta
monary artery and venous anatomy and the blood
supply to the lungs. Using 2DDE, 11 cases were
classified as the "favorable pattern" (group 1), and the
graphicGroupPAHypo
of
2Group
1Group
1Group
1Group
1Group
2Croup
1Croup
1Group
1Croup
1Group
MCAHypo
PA;
2Group
1Croup
2Group
2Group
1Group
2Group
MCANonconfluent;bilateral
PA;
2Group
inversus;dextrocardiaTricnspid
2Group
2Croup
1Group
2Group
1Group
2Group
2Croup
1Croup
2Croup
anteriorfrom
RVSitus
atresiaR
isomerism;AVC;
aortaanterior
fromRVTricuspid
DAHypo
MCAAbsent
PA;
MCANonconfluent;bilateral
PA;
DAHypo
subsequent angiography confirmed these data (Fig 1
and 2). Eleven cases were classified as "unfavorable
patterns" (group 2) with 2DDE, and the angiocardi
ography confirmed this diagnosis in all but one patient.
In this neonate (case 10) with PAVSD, situs inversus,
and dextrocardia, the visualization of a single ductus
arteriosus and normal pulmonary veins was correct
using 2DDE, but the confluence of the pulmonary
arteries was not demonstrated,
and the case was not
initially included in group 1. The angiocardiography
confirmed the pattern of blood supply to the lungs
and venous connections but showed confluent pul
monary arteries, and the definitive classification was
in group 1. In the last 12 cases investigated also with
color Doppler echocardiography,"
we did not encoun
ter any diagnostic mistake.
1Group
2Group
atresiaTricuspid
2Croup
atresiaCCTGACCTGAR
1Group
1Croup
1Group
2Group
2Croup
1Group
1Group
1Croup
2Group
1Croup
isomerism;AVC; 2Group
aortaanterior
fromRV2DDEGroup
1Group
*AVC, Atrioventricular
canal;
MCAHypo
PA;
MCAAbsent
PA;
MCAHypo
PA;
1Group
2Angio2Morphology
PA; MCA
CCTGA,
congenital!)
corrected
transposition of great arteries; DA, ductus arteriosus; PA, pulmo
nary artery; R, right; RV, right ventricle; and hypo, hypoplastic.
lungs and the morphology of the pulmonary arteries and pulmonary
veins. The results ol 2DDE in terms of intracardiac diagnosis and
classification in group 1 or 2 were compared with the findings ol
catheteri/.atiou and angiocardiography.
The 2DDE diagnosis of PAVSD and the assessment
of segments! combination and intracardiac anatomy
Table 2—Criteria for Classification
PAVSD*
Pulmonary
arteries
*DA, Ductus arteriosus.
of Patients with
Favorable
Pattern
(Group 1)Unfavorable
Confluent;
both >3mm
Pulmonary blood flow Single DA
Pulmonary venous
Normal
connections
The complete diagnosis and surgical treatment of
infants with PAVSD is still a challenge for pediatric
cardiologists and cardiac surgeons. The cases with
MCA and discontinuity of pulmonary arteries (group
2) require several surgical procedures, including unifbcalizatkm of the pulmonary artery tree, MCA ligation, or systemic-to-pnhnonary
artery shunt before
complete correction.17'21 Conversely, in patients with
confluent pulmonary arteries and single ductus arte
riosus (group 1), surgical treatment may consist of a
simple systeinic-to-pulmonary
shunt followed by com
plete correction or in a definitive correction as the
initial procedure.— In cases with "right isomerism,"
an anomaly of the pulmonary venous connections
frequently associated may complicate the surgical
approach.-' The conventional method for diagnosis
and surgical indication in this malformation is cardiac
catheteri/ation
and angiocardiography.1"5152- Recent
RESULTS
Data
DISCUSSION
Pattern
(Croup 2)
Nonconfluent or absent or
hypoplastic (>3 mm)
MCA; bilateral DA
Abnormal or obstructed
(or lM)th)
reports of palliative shunts being performed on the
basis of 2DDE in patients with reduced pulmonary
blood flow tend to exclude the cases of PAVSD because
of the nonpredictive pattern of the pulmonary arteries,
pulmonary veins, and blood supply.''•"
This prospective
study correctly identified with 2DDE the pattern of
intracardiac anatomy and of the pulmonary circulation
in infants with PAVSD; we obtained an adequate
correlation between 2DDE and angiocardiographic
data. In particular, the intracardiac
anatomy was
correctly assessed in all cases by 2DDE, and we
recognized with this method all ten patients with an
"unfavorable pattern" of the pulmonary arterial tree
(group 2) and 11 of 12 children with the "favorable
CHEST / 99 / 1 / JANUARY 1991
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21623/ on 05/03/2017
159
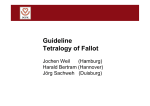
Fici'BK 1. Two-dimensional
ecliocardiograms
in
group 1 with PAVSD. A («;>;><!-):
Right oblique
snhxiphoid view showing pulmonary atrcsia (white
arnnr). snbaortic ventricular septal detect, conflu
ent pulmonary arteries (P), and morphology of right
pulmonary artery (Mack arrows). B (Itncer): Left
oblique snbxiphoid view showing intracardiac anat
omy and morphology ot left pulmonary artery (black
arnncx). A, Aorta; L\° left ventricle; RA, right
atrium; and RV right ventricle.
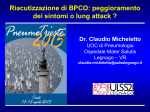
FICUKK 2. Group 1 with PAV'SD. A (left): Two-dimensional
echocardiogram.
Suprasternal
view showing
tortuous ductus arteriosns (D) with acute angle with descending aorta (A). P, Pulmonary artery; and LA,
left atrium. B (right): Aortogram in same patient, which confirmed morphology of pulmonary blood
supply.
160
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21623/ on 05/03/2017
Pulmonary Atresia with VSO (Marino et alj
pattern"
(group 1) without false-positives.
Our single
diagnostic error occurred in a patient with situs
inversus and dextrocardia. At present, 2DDE is not
able to diagnose any single pattern of pulmonary
circulation in children with PAVSD as much as angio
cardiography does; however, we suggest that in pa
tients with PAVSD, a precise 2DDE analysis improved
by color Doppler echocardiography14 can allow a dis
crimination between cases with confluent and goodsized (S:3 mm) pulmonary arteries, single ductus
arteriosus, and normal pulmonary venous connections
(group 1) and cases with an "unfavorable pattern" of
pulmonary arterial circulation. The patients in group
1 may be considered good candidates for a palliative
procedure without further invasive study, as suggested
for other malformations
with reduced pulmonary
blood flow.6-7On the contrary, patients in group 2 still
require cardiac catheterization and angiocardiography
to assess the pattern of pulmonary circulation and to
choose the best surgical option. Based on our experi
ence and in agreement with a very recent report,14 in
our department during the period from January 1989
to March 1990, five patients with PAVSD and a
"favorable pattern" underwent a successful palliative
systemic-to-pulmonary
artery shunt with 2DDE di
agnosis alone. In the same period, five further patients
underwent cardiac catheterization
and angiocardiog
raphy that confirmed the 2DDE diagnosis of PAVSD
and an "unfavorable pattern."
ACKNOWLEDGMENTS:
We thank Ms. Orietta Castellacci for
assistance in the preparation of the manuscript and Mr. Giuseppe
Bolla for technical assistance.
REFERENCES
1 Macartney F, Deverall P, Scott O. Haemodynamic characteristics
of systemic arterial blood supply to the lungs. Br Heart J 1973;
35:28-37
2 Macartney
FJ, Scott O, Deverall PB. Haemodynamic
and
anatomic characteristics of pulmonary blood supply in pulmo
nary atresia with ventricular septal defect including a case of
persistent fifth aortic arch. Br Heart J 1974; 36:1049-60
3 Bharati S, Paul MH, Idriss FS, Potkin RT, Lev M. The surgical
anatomy of pulmonary atresia with ventricular septal defect:
pseudotruncus. J Thorac Cardiovasc Surg 1975; 69:713-21
4 Thiene G, Bortolotti U, Gallucci V, Valente ML, Dalla Volta S.
Pulmonary atresia with ventricular septal defect: further ana
tomical observations. Br Heart J 1977; 39:1223-33
5 Thiene G, Frescura C, Bini RM, Valente ML, Gallucci V.
Histology of pulmonary arterial supply in pulmonary atresia
with ventricular septal defect. Circulation 1979; 60:1066-74
6 Ueda K, Nojima K, Saito A, Nakono H, Yokota M, Muraoka R.
Modified Blalock-Taussig shunt operation without cardiac cath
eterization:
two-dimensional
echocardiographic
preoperative
assessment in cyanotic infants. Am J Cardiol 1984; 54:1296-99
7 Marino B, Corno A, Pasquini L, Guccione P, Carta MC, Ballerini
L, et al. Indication for systemic to pulmonary artery shunts
guided by two-dimensional
and Doppler echocardiography:
criteria for patients selection. Ann Thorac Surg 1987; 44:495-98
8 Snider AR, Enderlein MA, Teitel DF, Juster RP. Two-dimen
sional echocardiographic
determination ol aortic and pulmonary
artery size from infancy to adulthood in normal subjects. Am J
Cardiol 1984; 53:218-23
9 Gutgesell HP, Hutha JC, Cohen MH, Latson LA. Two-dimen
sional echocardiographic
assessment of pulmonary artery and
aortic arch anatomy in cyanotic infants. J Am Coll Cardiol 1984;
4:1242-48
10 Sahn DJ, Allen HD. Real-time cross-sectional echocardiographic
imaging and measurements
of the patent ductus arteriosus in
infants and children. Circulation 1978; 58:343-54
11 Smallhorn JF. Hutha JC. Anderson RH, Macartney FJ. Suprasternal cross-sectional echocardiography
in assessment of patent
ductus arteriosus. Br Heart J 1982; 48:321-30
12 Smallhorn FJ, Gow R, Olley
Perlman M, et al. Combined
patent ductus arteriosus in the
indomethacin treatment. Am J
PM, Freedom RM, Swyer PR,
noninvasive assessment of the
preterm infant before and after
Cardiol 1984; 54:1300-04
13 Marino B, Ballerini L, Marcelletti C, Piva R, Pasquini L, Zacche
C, et al. Right oblique subxiphoid view for two-dimensional
echocardiographic
visualization of the right ventricle in congen
ital heart disease. Am J Cardiol 1984; 54:1064-68
14 Smyllie JH, Sutherland GR, Keeton BR. The value of Doppler
color flow mapping in determining pulmonary blood supply in
infants with pulmonary atresia with ventricular septal defect.
J Am Coll Cardiol 1989; 14/7:1759-65
15 Castaneda-Znnigo
W, Bass JI, Lock JE. Selective opacification
of arteries with balloon occlusion angiography.
138:727-29
Radiology 1981;
16 Freedom RM, Pongiglione G, Williams VVG, Trusler GA, Moes
CAF, Rowe RD. Pulmonary vein wedge angiography: indica
tions, results, and surgical correlates in 25 patients. Am J Cardiol
1983; 51:936-39
17 Davis CD, Fulton RE, Ritter DG, Mair DD, McGoon DC.
Congenital pulmonary atresia with ventricular septal defect:
angiographic and surgical correlates. Pediatr Radio! 1978; 128:
133-43
18 Momma K, Takao A, Ando M, Nakazawa M, Satomi C, Imai Y,
et al. Juxtaductal left pulmonary artery obstruction in pulmo
nary atresia. Br Heart J 1986; 55:39-44
19 Liao PK, Edwards W, Jtirsland PR, Puga FJ, Danielson GK,
Feldt RH. Pulmonary blood supply in patients with pulmonary
atresia and ventricular septal defect. J Am Coll Cardiol 1985;
6:1343-50
20 Shimakazi Y, Maehara T, Blackstone EH, Kirklin JW, Bargeron
LM. The structure of the pulmonary circulation in tetralogy of
Fallot with pulmonary atresia: a quantitative cineangiographic
study. J Thorac Cardiovasc Surg 1988; 95:1048-58
21 Millikan JS, Puga FJ, Danielson GK, Schaff HY Jursland PR,
Mair DD. Staged surgical repair of pulmonary atresia, ventric
ular septal defect, and hypoplastic, confluent pulmonary arter
ies. J Thorac Cardiovasc Surg 1986; 91:818-25
22 Olin CL, Ritter DG, McGoon DC, Wallace RB, Danielson GK.
Pulmonary atresia: surgical considerations
and results in 103
patients undergoing definitive repair. Circulation 1976; 54:3540
23 Di Donato R, di Carlo D, Squitieri C, Rossi E, Ammirati A,
Marino B, et al. Palliation of cardiac malformations associated
with right isomerism (asplenia syndrome) in infancy. Ann Thorac
Surg 1987; 44:35-9
CHEST / 99 / 1 / JANUARY. 1991
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21623/ on 05/03/2017
161