Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
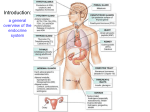
Hormonal Secretion of Pancreas 2 At the end of lecture students should be able to, • Describe Endocrine pancreas, • Describe Islet cells structure, • Describe the Actions of glucagon • Know the Factors affecting glucagon secretion, • Describe the Glucagon action on cells. •Describe the Insulin and glucagon regulate metabolism, Describe The regulation of blood glucose concentration, • Describe What is Diabetes mellitus, • Describe the Cardinal signs of DM, • Describe the Paracrine regulation of somatostatin,insulin and glucagon, •Know the treatment of diabetes mellitus, • Know the Clinical observation, • Know the Rehydration and insulin management. ENDOCRINE PANCREAS: Located behind the stomach between the spleen and duodenum. ISLET CELL STRUCTURE α cell : glucagon β cell : insulin δcell : somatostatin δce ll α cell β cell GLUCAGON: Even in the absence of significant physical activity or stress, several hours after carbohydrate intake, blood glucose levels fall below 4.5 mM because of utilization by brain and other tissues. Lowered blood glucose triggers secretion of glucagon, a hormone produced by the cells of the islets of Langerhans. Glucagon increases blood glucose in several ways: - stimulates breakdown of liver glycogen - inhibits glucose breakdown in liver - stimulates liver gluconeogenesis Together, these lead to accumulation of liver glucose, allowing its export to blood. Glucagon stimulates fatty acid mobilization in adipose tissue, liberating an alternate fuel for tissues (other than brain). GLUCAGON Synthesis and secretion of glucagon ACTIONS OF GLUCAGON Plasma: Glucose ↑ Amino acids ↓ Free fatty acids↑ GLUCAGON A 29-amino-acid polypeptide hormone that is a potent hyperglycemic agent. Produced by α cells in the pancreas Its major target is the liver, where it promotes: Glycogenolysis – the breakdown of glycogen to glucose Gluconeogenesis – synthesis of glucose from lactic acid and noncarbohydrates Release of glucose to the blood from liver cells. GLUCAGON SIGNALING SYNTHESIS DNA in α cells mRNA Preproglucagon proglucagon glucagon FACTORS AFFECTING GLUCAGON SECRETION: GLUCAGON ACTION ON CELLS: INSULIN & GLUCAGON REGULATE METABOLISM THE REGULATION OF BLOOD GLUCOSE CONCENTRATIONS DIABETES MELLITUS (DM) A serious disorder of carbohydrate metabolism Results from hyposecretion or hypoactivity of insulin. CARDINAL SIGNS OF DM The three cardinal signs of DM are: Polyuria – huge urine output. Polydipsia – excessive thirst. Polyphagia – excessive hunger and food consumption. DIABETES MELLITUS TYPE I Type 1: beta cells destroyed- no insulin producedchronic fasted state, "melting flesh", ketosis, acidosis, glucosurea, diuresis & coma. TYPE II A GROUP OF DISEASES: Insulin resistance keeps blood glucose too high Chronic complications: atherosclerosis, renal failure& blindness. SYMPTOMS OF DIABETES MELLITUS PARACRINE REGULATION OF SOMATOSTATIN, INSULIN & GLUCAGON The well-fed state: Stimulated by an increase in blood glucose level. Insulin stimulates glucose consumption and storage in muscle and liver. Stored as glycogen or triacyglycerol.24 Excessive but incomplete oxidation of fatty acids in the liver, resulting in overproduction of the ketone bodies acetoacetate and -hydroxybutyrate. Acetoacetate can convert to acetone, found in the blood of diabetics (breath odor like ethanol). The overproduction of ketone bodies is called ketosis, and their production is accompanied by decreased blood pH, (acidosis) or ketoacidosis, potentially lifethreatening. TREATMENT OF DIABETES Diet therapy 2. Oral hypoglycemic agents Insulin treatment. 4. Future treatment transplantation of islet cells artificial pancreas use of somatostatin Type 1 - insulin injections daily, or insulin infusion from pump. Type 2 - do not usually require insulin treatment because insulin synthesis partially preserved. Treatment relies on diet and oral hypoglycemic agents. DIABETIC KETOACIDOSIS Is the commonest cause of diabetes related death in children. Most occur as a result of cerebral edema. Definition: Hyperglycosuria and ketonuria Hyperglycemia pH <7.3 Bicarbonate < 15 mmol/L and > 5% or more dehydrated +/_ vomiting +/_ drowsy TREATMENT Confirm the diagnosis (HX, Biochem, And Clinical) Expansion of intravascular volume Correction of deficit in fluids, electrolytes, and acid base status Initiation of insulin therapy to correct intermediary metabolism CLINICAL OBSERVATION MONITORING Hourly- pulse rate, blood pressure, RR Capillary, venous or arterial blood gases Accurate I/O Blood glucose, electrolytes, urea Test urine for glucose and ketones Neurological Test –hourly or more frequently ECG Diagnosis confirmed REHYDRATION AND INSULIN MANAGEMENT FLUIDS Shock (poor peripheral pulses , reduced conscious level or coma) RESUSCITATION: Oxygen 100% by face mask Normal saline 0.9% 10ml/kg over 10-30 min until circulation restored. May be repeated. NG tube, to drain stomach if vomiting or impaired consciousness. -------------------------------------------------------------------