Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Population genetics wikipedia , lookup
Designer baby wikipedia , lookup
Oncogenomics wikipedia , lookup
Microevolution wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Medical genetics wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Frameshift mutation wikipedia , lookup
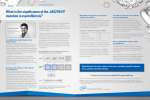
Review PHYSIOLOGY IN MEDICINE: A SERIES OF ARTICLES LINKING MEDICINE WITH SCIENCE Physiology in Medicine: Dale J. Benos, PhD, Editor; Edward Abraham, MD, Associate Editor; Peter D. Wagner, MD, Associate Editor Annals of Internal Medicine: Harold C. Sox, MD, Series Editor Narrative Review: Thrombocytosis, Polycythemia Vera, and JAK2 Mutations: The Phenotypic Mimicry of Chronic Myeloproliferation Jerry L. Spivak, MD The myeloproliferative disorders polycythemia vera, essential thrombocytosis, and primary myelofibrosis are clonal disorders arising in a pluripotent hematopoietic stem cell, causing an unregulated increase in the number of erythrocytes, leukocytes, or platelets, alone or in combination; eventual marrow dominance by the progeny of the involved stem cell; and a tendency to arterial or venous thrombosis, marrow fibrosis, splenomegaly, or transformation to acute leukemia, albeit at widely varying frequencies. The discovery of an activating mutation (V617F) in the gene for JAK2 (Janus kinase 2), a tyrosine kinase utilized by hematopoietic cell receptors for erythropoietin, thrombopoietin, and granulocyte colony-stimulating factor, provided an explanation for the shared clinical features of these 3 disorders. Constitutive JAK2 activation provides a growth and survival advantage to the hematopoietic cells of the affected clone. Because signaling by the mutated kinase utilizes normal pathways, the result is overproduction of morphologically normal blood cells, an often indolent course, and (in essential thrombocytosis) usually a normal life span. Because the erythropoietin, thrombopoietin, and granulocyte colony-stimulating factor receptors are all constitutively activated, polycythemia vera is the potential ultimate clinical phenotype of the JAK2 V617F mutation and, as a corollary, is the most common of the 3 disorders. The number of cells expressing the JAK2 V617F mutation (the allele burden) seems to correlate with the clinical phenotype. Preliminary results of clinical trials with agents that inhibit the mutated kinase indicate a reduction in splenomegaly and alleviation of night sweats, fatigue, and pruritus. I fibrosis, extramedullary hematopoiesis, or transformation to acute leukemia, albeit at widely varying frequencies. Moreover, the list of these disorders has grown (Table), and we now also understand that activating mutations of many different tyrosine kinases are responsible for Dameshek’s postulated undiscovered stimulus. n 1951, William Dameshek (1) hypothesized that such diseases as polycythemia vera and myelofibrosis with myeloid metaplasia (now designated as primary myelofibrosis), which he called “myeloproliferative disorders,” might not be distinct entities but rather interrelated disorders caused by an as-yet undiscovered stimulus acting on the bone marrow. Dameshek was prescient in his thinking, because we now know that the myeloproliferative disorders share many features, including origin in a pluripotent hematopoietic stem cell; an unregulated increase in the number of circulating erythrocytes, leukocytes, or platelets, alone or in combination; clonal dominance (see Glossary); and a tendency to develop arterial or venous thrombosis, marrow See also: Print Key Summary Points . . . . . . . . . . . . . . . . . . . . . . . 301 Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304 Web-Only Appendix Table Conversion of graphics into slides 300 © 2010 American College of Physicians Ann Intern Med. 2010;152:300-306. For author affiliation, see end of text. HEMATOPOIESIS AND www.annals.org CLONALITY Hematopoiesis is the orderly, continuous process by which pluripotent hematopoietic stem cells in the marrow give rise to the cells that populate the blood and lymphatic systems. Because a single pluripotent hematopoietic stem cell can give rise to all of the various cell types in the blood and lymphatic systems, hematopoiesis is by definition a clonal process (see Glossary). Normally, however, hematopoiesis is polyclonal because several pluripotent hematopoietic stem cells are producing progeny at all times. By contrast, monoclonality is the hallmark of the myeloproliferative disorders and defines their malignant nature (2). For unknown reasons, when a pluripotent hematopoietic stem cell transforms, it gains a survival advantage over its normal counterparts, such that only the progeny of the transformed stem cell eventually populate the blood and marrow. The rate of clonal dominance varies with the par- Thrombocytosis, Polycythemia Vera, and JAK2 Mutations Key Summary Points Polycythemia vera, essential thrombocytosis, and primary myelofibrosis are hematopoietic stem-cell disorders characterized by clonal dominance and unregulated increase in circulating erythrocytes, leukocytes, or platelets, alone or in combination. Clinical manifestations of these disorders include widely varying frequencies of arterial and venous thrombosis, marrow fibrosis, and extramedullary hematopoiesis or transformation to acute leukemia. Diagnostic challenges exist because of overlap of clinical manifestations among these 3 disorders and with other hematologic disorders, a situation known as phenotypic mimicry (see Glossary). Distinguishing these disorders is important because of differences in natural history, prognosis, and therapy. Phenotypic mimicry among the chronic myeloproliferative disorders occurs mainly because of a common mutation (V617F) in JAK2, the Janus family tyrosine kinase utilized by the erythropoietin, thrombopoietin, and granulocyte colony-stimulating factor receptors for ligand-mediated signal transduction. The JAK2 V617F mutation results in constitutive activation of a normal hematopoietic signal transduction pathway and an exaggeration of normal hematopoiesis modified to a variable extent by less well-defined genetic and epigenetic influences. Polycythemia vera, the most common of the 3 disorders, differs from its companion disorders because only erythrocytosis occurs in it and diagnosis depends on evidence of absolute erythrocytosis. Essential thrombocytosis does not have a unique clinical phenotype because isolated thrombocytosis can also be the presenting feature of polycythemia vera or primary myelofibrosis. The erythrocytosis present in polycythemia vera is the ultimate expression of the JAK2 V617F mutation and is an important therapeutic target. ticular myeloproliferative disorder, but the reasons for this are still undefined. For example, characteristically almost all of the cells in the blood and marrow of patients with chronic myelogenous leukemia or primary myelofibrosis are progeny of the malignant clone at diagnosis, whereas in patients with essential thrombocytosis and polycythemia vera, blood and marrow cells derived from normal stem cells are usually present at diagnosis—although clonal dominance will eventually occur in these disorders as well (3, 4). www.annals.org Review ACQUIRED JAK2 MUTATIONS Biology The genetic lesions responsible for the various myeloproliferative disorders include balanced translocations, deletions, and point mutations, which lead to constitutive activation of a particular receptor tyrosine kinase in all cases. These activated kinases not only represent Dameshek’s undiscovered stimulus but also impart the clinical phenotype (see Glossary) to each myeloproliferative disorder (Table), permitting for the first time their molecular classification (5). As shown in the Table, polycythemia vera, essential thrombocytosis, and primary myelofibrosis are unique among the myeloproliferative disorders because they share a mutation causing constitutive activation of JAK2 (Janus kinase 2 [see Glossary]) and, as a corollary, the interrelatedness that Dameshek predicted (Figure, top). Indeed, their interrelatedness is epidemiologically unique because first-degree family members of a patient with 1 of these 3 myeloproliferative disorders have a 3- to 7-fold increased risk for acquiring any of the 3 disorders (6). JAK2 is the member of the Janus tyrosine kinase family that is responsible for signal transduction by the erythropoietin, thrombopoietin, granulocyte macrophage colonystimulating factor, and granulocyte colony-stimulating factor receptors in hematopoietic cells, as well as for signal transduction by many cytokine receptors, such as interleukin (IL)-3, IL-5, and IL-6 receptors (7). JAK2 is normally activated when these receptors bind their cognate ligands (see Glossary): erythropoietin, thrombopoietin, granulocyte colony-stimulating factor, granulocyte macrophage colonystimulating factor, IL-3, IL-5, or IL-6. However, in the myeloproliferative disorders, a point mutation resulting in a switch from phenylalanine to valine at amino acid position 671 (V617F) in the regulatory domain of the protein releases the adjacent kinase domain from inhibition, leading to constitutive activation in the absence of any ligand (8). The activated kinase promotes cell proliferation and resistance to cell Table. The Chronic Myeloproliferative Disorders Disease Molecular Defect* Chronic myelogenous leukemia Chronic eosinophilic leukemia and the hypereosinophilic syndrome Chronic neutrophilic leukemia Chronic myelomonocytic leukemia Systemic mastocytosis Polycythemia vera BCR-ABL FIP1L1-PDGFRA Essential thrombocytosis Primary myelofibrosis BCR-ABL p230 TEL-PDGFRB KIT D816V JAK2 V617F (⬃92% positive) JAK2 exon 12 mutations (3% positive) JAK2 V617F (⬃50% positive) MPL W515L/K (⬃3% positive) MPL K39N JAK2 V617F (⬃50% positive) MPL W515L/K (⬃14% positive) * Representative molecular defects caused by balanced translocations or point mutations in the chronic myeloproliferative disorders. 2 March 2010 Annals of Internal Medicine Volume 152 • Number 5 301 Review Thrombocytosis, Polycythemia Vera, and JAK2 Mutations Figure. The close interrelationship among the chronic myeloproliferative disorders, and a schematic representation of hematopoietic stem-cell commitment and JAK2 utilization. The Interrelationship Among the Chronic Myeloproliferative Disorders Primary Myelofibrosis Isolated Thrombocytosis Polycythemia Vera Essential Thrombocytosis Schematic Representation of the Progenitor Cells Most Sensitive to JAK2 V617F Pluripotent Hematopoietic Stem Cell Common Lymphoid Progenitor Cell Epidemiology Common Myeloid Progenitor Cell T Lymphocytes B Lymphocytes Granulocyte-Monocyte Progenitors fect is most pronounced in maturing hematopoietic cells, which require erythropoietin, thrombopoietin, and granulocyte colony-stimulating factor for proliferation and survival, compared with undifferentiated hematopoietic stem cells, which do not (9) and in which only the thrombopoietin receptor is expressed (10). Of importance, unlike most of the other disorders in the Table, with JAK2 mutations, constitutive signaling still occurs through normal signal transduction pathways. Consequently, the result is overproduction of morphologically normal blood cells, a generally indolent course, and in essential thrombocytosis usually a normal life span (11). JAK2 V617F is probably not the initiating molecular defect in polycythemia vera, essential thrombocytosis, or primary myelofibrosis, because it is not present in all patients (12), particularly those with the familial form of these disorders (13); it can be acquired by the malignant clone after the acquisition of other genetic abnormalities (14, 15); and it is also absent in the myeloblasts of some patients expressing JAK2 V617F in their mature blood cells when leukemic transformation occurs (16). In addition, in contrast to JAK2 V617F, which is located in exon 14 of the gene, several different activating mutations have also been identified in exon 12 (17), which, for unknown reasons, primarily cause erythrocytosis but occasionally may be associated with thrombocytosis and splenomegaly (18). Erythroid Progenitors JAK2 V617F Megakaryocyte Progenitors Top. The chronic myeloproliferative disorders not only are phenotypically similar but can also evolve into each other. From a clinical perspective, as illustrated isolated thrombocytosis of unknown cause should not automatically be assumed to be essential thrombocytosis because isolated thrombocytosis can also be the presenting manifestation of polycythemia vera or primary myelofibrosis. Bottom. JAK2 is an obligatory kinase primarily for erythroid and megakaryocytic cell development; granulocytes can also use JAK1, and lymphocytes do not require JAK2. As illustrated, polycythemia vera is the ultimate clinical phenotype that can be caused by constitutive JAK2 activation. death, as well as hypersensitivity to hematopoietic growth factors and cytokines signaling through receptors utilizing JAK2. Thus, cells expressing the mutant JAK2 have both a growth and a survival advantage over their normal counterparts and expand their numbers autonomously. This ef302 2 March 2010 Annals of Internal Medicine Volume 152 • Number 5 JAK2 V617F expression is present in more than 95% of patients with polycythemia vera and in approximately 50% of patients with essential thrombocytosis and primary myelofibrosis (19 –23). The various mutations in JAK2 exon 12 account for the disease in an additional 3% of patients with polycythemia vera (17, 18, 24). In a small proportion of patients with essential thrombocytosis and primary myelofibrosis, mutations are present in the thrombopoietin receptor gene MPL (18, 25, 26), but the genetic basis for these disorders in other patients is still unknown. JAK2 V617F expression has also been observed at a very low frequency in various other clonal myeloid disorders (24, 27, 28), but with the exception of a subgroup of patients with sideroblastic anemia and thrombocytosis (29), none display elements of the clinical phenotype associated with JAK2 V617F expression in polycythemia vera, essential thrombocytosis, or primary myelofibrosis. How the same mutation could be responsible for 3 different clinical phenotypes is not entirely known. In vitro clonal assays (30), animal models (31, 32), studies quantitating the JAK2 V617F allele burden in humans (see Glossary) (12, 33, 34), and the recent identification of a characteristic constitutional JAK2 haplotype (see Glossary) in patients with a myeloproliferative disorder (35–37) and other mutated genes (such as TET2 [38]) indicate that gene dose, sex, genetic predisposition, and additional mutations all have roles. With respect to gene dose, the JAK2 V617F allelic burden correlates with clinical phenotype in www.annals.org Thrombocytosis, Polycythemia Vera, and JAK2 Mutations the myeloproliferative disorders. In essential thrombocytosis, where the JAK2 V617F allele burden is usually low (12), thrombocytosis alone is the rule, the JAK2 V617F allelic burden is relatively constant, and homozygosity for the mutation is infrequent (4, 39). In polycythemia vera, however, because of a propensity for mitotic recombination (see Glossary) involving chromosome 9p, where the JAK2 gene is located (40), the incidence of homozygosity for the mutation increases during the disease (12), and the increased JAK2 V617F allelic burden is associated with erythrocytosis, leukocytosis, splenomegaly, and pruritus in addition to thrombocytosis (41). Pathophysiology Because JAK2 is the obligate tyrosine kinase for the erythropoietin and thrombopoietin receptors (the granulocyte colony-stimulating factor receptor can also utilize JAK1), polycythemia vera is the ultimate phenotypic expression of JAK2 V617F (Figure, bottom). In this regard, many patients with polycythemia vera present initially with thrombocytosis alone, which is well documented (42). Furthermore, many JAK2 V617F–positive patients with essential thrombocytosis have a “polycythemia vera–like” phenotype compared with their JAK2 V617F–negative counterparts, with relatively higher hematocrits and leukocyte counts and an increased incidence of venous thrombosis (43). Indeed, when the erythrocyte mass was measured directly in such patients, approximately 65% of them actually had absolute erythrocytosis (see Glossary) and thus had unrecognized polycythemia vera (44), supporting the proposition that polycythemia vera is the ultimate phenotypic expression of JAK2 V617F and should always be considered in the differential diagnosis of isolated thrombocytosis. The reason for the masked erythrocytosis in JAK2 V617F–positive patients with apparent essential thrombocytosis can be explained as follows. An increase in erythrocyte production (Appendix Table, available at www.annals .org) due to recombinant erythropoietin (45), chronic carbon monoxide exposure (46), or androgenic steroids is associated with a reciprocal decrease in the plasma volume because the body always attempts to maintain a normal total blood volume. By contrast, for unknown reasons, in polycythemia vera, where endogenous erythropoietin production is suppressed, the plasma volume either does not change or increases with expansion of the erythrocyte mass (47, 48). This initially has the beneficial effect of reducing peripheral vascular resistance, but at the same time it can mask the actual increase in the erythrocyte mass, resulting in an apparently normal hematocrit. The situation is exacerbated with splenomegaly, because the plasma volume will expand even further (47). Unfortunately, the expanded plasma volume is not protective against venous or arterial thrombosis, which are the most common causes of morbidity and mortality in polycythemia vera (49). www.annals.org Review Of course, conditions that solely contract the plasma volume (Appendix Table) will also make the hematocrit or hemoglobin level seem elevated when it is not. These observations have important clinical ramifications: A high hematocrit or hemoglobin level is not synonymous with true erythrocytosis any more than a normal hematocrit or hemoglobin level is synonymous with the absence of erythrocytosis when polycythemia vera is a diagnostic consideration (44, 47, 48). Indeed, unless the hematocrit is 60% or greater (hemoglobin level, 20 g/dL), distinguishing plasma volume contraction from absolute erythrocytosis is not possible (50). HOW IS THE JAK2 V617 ASSAY USED DIAGNOSTICALLY? The Differential Diagnosis of Thrombocytosis and Polycythemia Vera The discovery of JAK2 V617F provided a way to distinguish polycythemia vera and approximately 50% of patients with essential thrombocytosis and primary myelofibrosis, from the many benign and malignant disorders they mimic clinically, albeit not from each other (51). Thus, the presence of the JAK2 V617F mutation confirms the clinical impression of a myeloproliferative disorder, but because the mutation occurs in all 3 disorders, it cannot be used to distinguish among them, nor does its absence exclude a myeloproliferative disorder. However, because polycythemia vera is the ultimate clinical phenotype of JAK2 V617F expression and the most common myeloproliferative disorder, a positive JAK2 V617F assay should always suggest the possibility of this disorder. Because only erythrocytosis distinguishes polycythemia vera from essential thrombocytosis and primary myelofibrosis, the diagnosis of polycythemia vera is still clinically based. At the same time, although polycythemia vera is the ultimate expression of a JAK2 mutation, not all patients with erythrocytosis expressing a JAK2 mutation will develop polycythemia vera (18). With expanded access to medical care, patients with myeloproliferative disorders are being seen much earlier in the course of their disease, and the marked degree of hematocrit or hemoglobin elevation classically associated with polycythemia vera is no longer commonly encountered. Thus, the presence of polycythemia vera may only become apparent over time. When polycythemia vera presents with erythrocytosis, often microcytic; leukocytosis; and thrombocytosis, the diagnosis is not in doubt. This is also true when it presents as erythrocytosis together with thrombocytosis or leukocytosis or splenomegaly (52). Furthermore, tissue iron deficiency is often paradoxically associated with erythrocytosis in polycythemia vera because of iron utilization by the expanding the erythrocyte mass, which could, of course, contribute to the presence of thrombocytosis (53). However, between 7% and 20% of patients with polycythemia vera present initially with only thrombocytosis (4, 42) and 2 March 2010 Annals of Internal Medicine Volume 152 • Number 5 303 Review Thrombocytosis, Polycythemia Vera, and JAK2 Mutations up to 17% with only erythrocytosis (54). A JAK2 V617F assay can be useful diagnostically in these patients. With respect to diagnostic parsimony, however, although polycythemia vera is the most common myeloproliferative disorder, investigators of a large epidemiologic study found that only 5% of patients with persistent erythrocytosis had polycythemia vera (52). Therefore, the first obligation when presented with a patient with a persistent high hematocrit or hemoglobin level is not to look for polycythemia vera but rather to look for correctable causes of erythrocytosis (Appendix Table). In a patient suspected of having erythrocytosis, a careful history with respect to tobacco (46) or androgen (55) use or a sleep disturbance (56) combined with arterial oxygen saturation and serum erythropoietin measurements constitute the initial evaluation. A low or normal serum erythropoietin level is an indication for a JAK2 V617F assay, because a low serum erythropoietin level indicates that the marrow erythroid progenitor cell pool has probably expanded autonomously, and a normal serum erythropoietin level provides no diagnostic clues. If the serum erythropoietin level is high, a secondary form of erythrocytosis may be present. If a JAK2 V617F assay is negative and tobacco use, sleep apnea, or hepatic or renal abnormality is not evident, hematologic referral is indicated for evaluation of mutations involving JAK2 exon 12 (18), the von Hippel–Lindau gene (Chuvash polycythemia) (57), the erythropoietin receptor, or hemoglobin genes (58). ARE JAK2 MUTATIONS RELEVANT TARGETS THERAPY? FOR DRUG Management of the Chronic Myeloproliferative Disorders JAK2 is an obligatory kinase for the proliferation and differentiation of erythroid cells and megakaryocytes and, therefore, is a relevant therapeutic target for agents that specifically inhibit its activity. To date, clinical trials are investigating several JAK2 inhibitors in patients with myeloproliferative disorder, and more inhibitors are being developed (59, 60). The results to date indicate that these inhibitors reduce splenomegaly and alleviate constitutional symptoms, such as night sweats, fatigue, and pruritus, in a reversible manner, suggesting that a substantial inflammatory component contributes to the signs and symptoms of the myeloproliferative disorders (61), possibly through JAK2 V617F–activated cytokine receptors. However, these inhibitors have had only a modest impact on the JAK2 V617F allele burden, although this may require a longer duration of therapy. At the same time, pluripotent hematopoietic stem cells do not seem to require JAK2 for their survival or proliferation (9), and JAK2 mutations, unlike the BCR-ABL fusion kinase in chronic myelogenous leukemia, are probably not the initiating molecular event in polycythemia vera, essential thrombocytosis, or primary myelofibrosis. Therefore, JAK2 inhibitors may prove to be 304 2 March 2010 Annals of Internal Medicine Volume 152 • Number 5 Glossary Absolute erythrocytosis: An elevated hematocrit or hemoglobin level can be caused by an elevated erythrocyte mass (absolute erythrocytosis) or a contracted plasma volume (pseudo- or relative erythrocytosis). Allele: Each one of a pair of chromosomes has a single copy of a particular gene located at the same position. These copies are known as the alleles of the gene. The copies may be identical (homozygous) or may differ (heterozygous) with respect to their DNA composition, such as when 1 allele has a mutation or single nucleotide polymorphism. Allele burden: The percentage of cells expressing a mutation in 1 or both alleles of a gene. For the JAK2 V617F mutation on chromosome 9p, the allele burden is usually measured in the blood neutrophils. The allele burden provides an estimate of the number of neutrophils from the malignant clone present in the circulation and thus whether clonal dominance is present. However, unless the allele burden is greater than 75%, it cannot provide an estimate of whether 1 or both JAK2 alleles are involved. For example, a neutrophil JAK2 V617F allele burden of 50% could indicate that all of the circulating neutrophils are derived from the malignant clone but have only 1 allele involved (heterozygosity for the mutation) or that 50% of the neutrophils have both JAK2 alleles mutated (homozygosity for the mutation) but 50% are from normal clones and have no mutated alleles. The marrow neutrophil allele burden is similar to the blood neutrophil allele burden. Clonal dominance: This occurs when the cells from 1 clone in a cell population have a growth advantage over the cells from all of the other clones. Usually in hematopoietic malignant conditions, such as acute leukemia or chronic myelogenous leukemia, there is clonal dominance by the malignant clone at disease presentation. In the chronic myeloproliferative disorders, this is usually also true for primary myelofibrosis but not for polycythemia vera or essential thrombocytosis, in keeping with their more indolent clinical course. Clonality: This describes the stem-cell origin of a cell population. If all of the cells are derived from the same parental stem cell, the cell population is monoclonal. If the cells arise from several different parental stem cells, the cell population is polyclonal, which is the normal situation. Cognate ligand: A protein that specifically binds to and activates a particular cell surface receptor. For example, erythropoietin is the cognate ligand of the erythropoietin receptor. Genotype: The full complement of inherited genetic information in a person, but the term is also used to refer to the allelic status of a specific gene or single nucleotide polymorphism. Haplotype: The alleles at various loci on a chromosome that are transmitted together. Alternatively, the term is used to refer to a set of single nucleotide polymorphisms that are statistically associated on the same chromosome. Janus kinases: A tyrosine kinase family comprising 4 members, JAK1, JAK2, JAK3, and TYK2, which are utilized by hematopoietic growth factor and cytokine receptors to phosphorylate tyrosine residues on specific intracellular proteins after the interaction of the receptor with its ligand. JAK2 is used by the erythropoietin, thrombopoietin, and granulocyte colony-stimulating factor receptors to transmit signals and thus is integrally involved in hematopoiesis. JAK1, JAK3, and TYK2 are used by the interleukin and interferon receptors to transmit signals and thus are primarily involved in the regulation of immune function. Phenotype: The observed physical and behavioral characteristics of an organism or a disease. Phenotypic mimicry: When the clinical features of 2 diseases are similar but their genotypes differ. Mitotic recombination: When chromatids exchange genetic material during mitosis, the resulting chromosome pairs will share identical alleles in the region that the crossover occurred, resulting in loss of the expected heterozygosity of those alleles. Mitotic recombination is the genetic mechanism thought to account for homozygosity with respect to the JAK2 V617F mutation on chromosome 9p. Loss of heterozygosity is an important mechanism by which tumor cells gain advantage over normal cells. Single nucleotide polymorphism: A DNA sequence variation occurring when a single nucleotide—A, T, G, or C—differs between paired chromosomes because of a nucleotide substitution, deletion, or insertion that produces 2 alleles. These can occur anywhere in a gene and may be silent or may cause an alteration in gene function or expression. Because nearby single nucleotide polymorphisms on a chromosome often closely correlate, analysis can be used to identify specific regions of the genome and also the extent to which different persons share the same sequence of alleles (haplotype) in that particular genomic region. www.annals.org Thrombocytosis, Polycythemia Vera, and JAK2 Mutations useful only for suppressing disease manifestations but not for eradicating disease, in contrast to such agents as interferon (62), which seem capable of eradicating the malignant clone (63). Of course, none of these agents can substitute initially for phlebotomy therapy for polycythemia vera, which immediately reduces the erythrocyte mass and lowers blood viscosity (64). From the Johns Hopkins Medical Institutions, Baltimore, Maryland. Grant Support: From the National Institutes of Health (P01CA108671). Potential Conflicts of Interest: Disclosures can be viewed at www .acponline.org/authors/icmje/ConflictOfInterestForms.do?msNum⫽M09 -1012. Requests for Single Reprints: Jerry L. Spivak, MD, Hematology Division, Johns Hopkins University School of Medicine, Traylor Building, Room 924, 720 Rutland Avenue, Baltimore, MD 21205-2196; e-mail, [email protected]. References 1. Dameshek W. Some speculations on the myeloproliferative syndromes. Blood. 1951;6:372-5. [PMID: 14820991] 2. Adamson JW, Fialkow PJ, Murphy S, Prchal JF, Steinmann L. Polycythemia vera: stem-cell and probable clonal origin of the disease. N Engl J Med. 1976; 295:913-6. [PMID: 967201] 3. Golde DW, Hocking WG, Koeffler HP, Adamson JW. Polycythemia: mechanisms and management. Ann Intern Med. 1981;95:71-87. [PMID: 7018337] 4. Moliterno AR, Williams DM, Rogers O, Isaacs MA, Spivak JL. Phenotypic variability within the JAK2 V617F-positive MPD: roles of progenitor cell and neutrophil allele burdens. Exp Hematol. 2008;36:1480-6. [PMID: 18723264] 5. De Keersmaecker K, Cools J. Chronic myeloproliferative disorders: a tyrosine kinase tale. Leukemia. 2006;20:200-5. [PMID: 16341034] 6. Landgren O, Goldin LR, Kristinsson SY, Helgadottir EA, Samuelsson J, Björkholm M. Increased risks of polycythemia vera, essential thrombocythemia, and myelofibrosis among 24,577 first-degree relatives of 11,039 patients with myeloproliferative neoplasms in Sweden. Blood. 2008;112:2199-204. [PMID: 18451307] 7. Verma A, Kambhampati S, Parmar S, Platanias LC. Jak family of kinases in cancer. Cancer Metastasis Rev. 2003;22:423-34. [PMID: 12884916] 8. Campbell PJ, Green AR. The myeloproliferative disorders. N Engl J Med. 2006;355:2452-66. [PMID: 17151367] 9. Parganas E, Wang D, Stravopodis D, Topham DJ, Marine JC, Teglund S, et al. Jak2 is essential for signaling through a variety of cytokine receptors. Cell. 1998;93:385-95. [PMID: 9590173] 10. Solar GP, Kerr WG, Zeigler FC, Hess D, Donahue C, de Sauvage FJ, et al. Role of c-mpl in early hematopoiesis. Blood. 1998;92:4-10. [PMID: 9639492] 11. Passamonti F, Rumi E, Pungolino E, Malabarba L, Bertazzoni P, Valentini M, et al. Life expectancy and prognostic factors for survival in patients with polycythemia vera and essential thrombocythemia. Am J Med. 2004;117:755-61. [PMID: 15541325] 12. Moliterno AR, Williams DM, Rogers O, Spivak JL. Molecular mimicry in the chronic myeloproliferative disorders: reciprocity between quantitative JAK2 V617F and Mpl expression. Blood. 2006;108:3913-5. [PMID: 16912229] 13. Bellanné-Chantelot C, Chaumarel I, Labopin M, Bellanger F, Barbu V, De Toma C, et al. Genetic and clinical implications of the Val617Phe JAK2 mutation in 72 families with myeloproliferative disorders. Blood. 2006;108:346-52. [PMID: 16537803] 14. Kralovics R, Teo SS, Li S, Theocharides A, Buser AS, Tichelli A, et al. Acquisition of the V617F mutation of JAK2 is a late genetic event in a subset of patients with myeloproliferative disorders. Blood. 2006;108:1377-80. [PMID: 16675710] 15. Kralovics R. Genetic complexity of myeloproliferative neoplasms. Leukemia. 2008;22:1841-8. [PMID: 18754034] www.annals.org Review 16. Theocharides A, Boissinot M, Girodon F, Garand R, Teo SS, Lippert E, et al. Leukemic blasts in transformed JAK2-V617F-positive myeloproliferative disorders are frequently negative for the JAK2-V617F mutation. Blood. 2007; 110:375-9. [PMID: 17363731] 17. Scott LM, Tong W, Levine RL, Scott MA, Beer PA, Stratton MR, et al. JAK2 exon 12 mutations in polycythemia vera and idiopathic erythrocytosis. N Engl J Med. 2007;356:459-68. [PMID: 17267906] 18. Williams DM, Kim AH, Rogers O, Spivak JL, Moliterno AR. Phenotypic variations and new mutations in JAK2 V617F-negative polycythemia vera, erythrocytosis, and idiopathic myelofibrosis. Exp Hematol. 2007;35:1641-6. [PMID: 17920755] 19. Baxter EJ, Scott LM, Campbell PJ, East C, Fourouclas N, Swanton S, et al; Cancer Genome Project. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet. 2005;365:1054-61. [PMID: 15781101] 20. James C, Ugo V, Le Couédic JP, Staerk J, Delhommeau F, Lacout C, et al. A unique clonal JAK2 mutation leading to constitutive signalling causes polycythaemia vera. Nature. 2005;434:1144-8. [PMID: 15793561] 21. Kralovics R, Passamonti F, Buser AS, Teo SS, Tiedt R, Passweg JR, et al. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N Engl J Med. 2005;352:1779-90. [PMID: 15858187] 22. Levine RL, Wadleigh M, Cools J, Ebert BL, Wernig G, Huntly BJ, et al. Activating mutation in the tyrosine kinase JAK2 in polycythemia vera, essential thrombocythemia, and myeloid metaplasia with myelofibrosis. Cancer Cell. 2005;7:387-97. [PMID: 15837627] 23. Zhao R, Xing S, Li Z, Fu X, Li Q, Krantz SB, et al. Identification of an acquired JAK2 mutation in polycythemia vera. J Biol Chem. 2005;280:2278892. [PMID: 15863514] 24. Jelinek J, Oki Y, Gharibyan V, Bueso-Ramos C, Prchal JT, Verstovsek S, et al. JAK2 mutation 1849G⬎T is rare in acute leukemias but can be found in CMML, Philadelphia chromosome-negative CML, and megakaryocytic leukemia. Blood. 2005;106:3370-3. [PMID: 16037387] 25. Pikman Y, Lee BH, Mercher T, McDowell E, Ebert BL, Gozo M, et al. MPLW515L is a novel somatic activating mutation in myelofibrosis with myeloid metaplasia. PLoS Med. 2006;3:e270. [PMID: 16834459] 26. Pardanani AD, Levine RL, Lasho T, Pikman Y, Mesa RA, Wadleigh M, et al. MPL515 mutations in myeloproliferative and other myeloid disorders: a study of 1182 patients. Blood. 2006;108:3472-6. [PMID: 16868251] 27. Jones AV, Kreil S, Zoi K, Waghorn K, Curtis C, Zhang L, et al. Widespread occurrence of the JAK2 V617F mutation in chronic myeloproliferative disorders. Blood. 2005;106:2162-8. [PMID: 15920007] 28. Steensma DP, Dewald GW, Lasho TL, Powell HL, McClure RF, Levine RL, et al. The JAK2 V617F activating tyrosine kinase mutation is an infrequent event in both “atypical” myeloproliferative disorders and myelodysplastic syndromes. Blood. 2005;106:1207-9. [PMID: 15860661] 29. Szpurka H, Tiu R, Murugesan G, Aboudola S, Hsi ED, Theil KS, et al. Refractory anemia with ringed sideroblasts associated with marked thrombocytosis (RARS-T), another myeloproliferative condition characterized by JAK2 V617F mutation. Blood. 2006;108:2173-81. [PMID: 16741247] 30. Dupont S, Massé A, James C, Teyssandier I, Lécluse Y, Larbret F, et al. The JAK2 617V⬎F mutation triggers erythropoietin hypersensitivity and terminal erythroid amplification in primary cells from patients with polycythemia vera. Blood. 2007;110:1013-21. [PMID: 17389763] 31. Lacout C, Pisani DF, Tulliez M, Gachelin FM, Vainchenker W, Villeval JL. JAK2V617F expression in murine hematopoietic cells leads to MPD mimicking human PV with secondary myelofibrosis. Blood. 2006;108:1652-60. [PMID: 16670266] 32. Tiedt R, Hao-Shen H, Sobas MA, Looser R, Dirnhofer S, Schwaller J, et al. Ratio of mutant JAK2-V617F to wild-type Jak2 determines the MPD phenotypes in transgenic mice. Blood. 2008;111:3931-40. [PMID: 18160670] 33. Vannucchi AM, Antonioli E, Guglielmelli P, Rambaldi A, Barosi G, Marchioli R, et al. Clinical profile of homozygous JAK2 617V⬎F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110: 840-6. [PMID: 17379742] 34. Pietra D, Li S, Brisci A, Passamonti F, Rumi E, Theocharides A, et al. Somatic mutations of JAK2 exon 12 in patients with JAK2 (V617F)-negative myeloproliferative disorders. Blood. 2008;111:1686-9. [PMID: 17984312] 35. Jones AV, Chase A, Silver RT, Oscier D, Zoi K, Wang YL, et al. JAK2 haplotype is a major risk factor for the development of myeloproliferative neoplasms. Nat Genet. 2009;41:446-9. [PMID: 19287382] 2 March 2010 Annals of Internal Medicine Volume 152 • Number 5 305 Review Thrombocytosis, Polycythemia Vera, and JAK2 Mutations 36. Olcaydu D, Harutyunyan A, Jäger R, Berg T, Gisslinger B, Pabinger I, et al. A common JAK2 haplotype confers susceptibility to myeloproliferative neoplasms. Nat Genet. 2009;41:450-4. [PMID: 19287385] 37. Kilpivaara O, Mukherjee S, Schram AM, Wadleigh M, Mullally A, Ebert BL, et al. A germline JAK2 SNP is associated with predisposition to the development of JAK2(V617F)-positive myeloproliferative neoplasms. Nat Genet. 2009;41:455-9. [PMID: 19287384] 38. Delhommeau F, Dupont S, Della Valle V, James C, Trannoy S, Massé A, et al. Mutation in TET2 in myeloid cancers. N Engl J Med. 2009;360:2289-301. [PMID: 19474426] 39. Pemmaraju N, Moliterno AR, Williams DM, Rogers O, Spivak JL. The quantitative JAK2 V617F neutrophil allele burden does not correlate with thrombotic risk in essential thrombocytosis [Letter]. Leukemia. 2007;21:2210-2. [PMID: 17507997] 40. Kralovics R, Guan Y, Prchal JT. Acquired uniparental disomy of chromosome 9p is a frequent stem cell defect in polycythemia vera. Exp Hematol. 2002; 30:229-36. [PMID: 11882360] 41. Vannucchi AM, Antonioli E, Guglielmelli P, Longo G, Pancrazzi A, Ponziani V, et al; MPD Research Consortium. Prospective identification of highrisk polycythemia vera patients based on JAK2(V617F) allele burden. Leukemia. 2007;21:1952-9. [PMID: 17625606] 42. Jantunen R, Juvonen E, Ikkala E, Oksanen K, Anttila P, Ruutu T. Development of erythrocytosis in the course of essential thrombocythemia. Ann Hematol. 1999;78:219-22. [PMID: 10391102] 43. Campbell PJ, Scott LM, Buck G, Wheatley K, East CL, Marsden JT, et al; United Kingdom Myeloproliferative Disorders Study Group. Definition of subtypes of essential thrombocythaemia and relation to polycythaemia vera based on JAK2 V617F mutation status: a prospective study. Lancet. 2005;366:1945-53. [PMID: 16325696] 44. Cassinat B, Laguillier C, Gardin C, de Beco V, Burcheri S, Fenaux P, et al; PV-Nord Group. Classification of myeloproliferative disorders in the JAK2 era: is there a role for red cell mass? [Letter]. Leukemia. 2008;22:452-3. [PMID: 17713549] 45. Lundby C, Thomsen JJ, Boushel R, Koskolou M, Warberg J, Calbet JA, et al. Erythropoietin treatment elevates haemoglobin concentration by increasing red cell volume and depressing plasma volume. J Physiol. 2007;578:309-14. [PMID: 17095558] 46. Smith JR, Landaw SA. Smokers’ polycythemia. N Engl J Med. 1978;298:610. [PMID: 618465] 47. Lamy T, Devillers A, Bernard M, Moisan A, Grulois I, Drenou B, et al. Inapparent polycythemia vera: an unrecognized diagnosis. Am J Med. 1997;102: 14-20. [PMID: 9209196] 48. Spivak JL. Polycythemia vera: myths, mechanisms, and management. Blood. 2002;100:4272-90. [PMID: 12393615] 49. Marchioli R, Finazzi G, Landolfi R, Kutti J, Gisslinger H, Patrono C, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. 306 2 March 2010 Annals of Internal Medicine Volume 152 • Number 5 J Clin Oncol. 2005;23:2224-32. [PMID: 15710945] 50. Pearson TC, Botterill CA, Glass UH, Wetherley-Mein G. Interpretation of measured red cell mass and plasma volume in males with elevated venous PCV values. Scand J Haematol. 1984;33:68-74. [PMID: 6463587] 51. Spivak JL, Silver RT. The revised World Health Organization diagnostic criteria for polycythemia vera, essential thrombocytosis, and primary myelofibrosis: an alternative proposal. Blood. 2008;112:231-9. [PMID: 18401028] 52. Ruggeri M, Tosetto A, Frezzato M, Rodeghiero F. The rate of progression to polycythemia vera or essential thrombocythemia in patients with erythrocytosis or thrombocytosis. Ann Intern Med. 2003;139:470-5. [PMID: 13679323] 53. Kuku I, Kaya E, Yologlu S, Gokdeniz R, Baydin A. Platelet counts in adults with iron deficiency anemia. Platelets. 2009;20:401-5. [PMID: 19658005] 54. Berglund S, Zettervall O. Incidence of polycythemia vera in a defined population. Eur J Haematol. 1992;48:20-6. [PMID: 1730276] 55. Besa EC, Gorshein D, Gardner FH. Androgens and human blood volume changes. Comparison in normal and various anemic states. Arch Intern Med. 1974;133:418-25. [PMID: 4521323] 56. Choi JB, Loredo JS, Norman D, Mills PJ, Ancoli-Israel S, Ziegler MG, et al. Does obstructive sleep apnea increase hematocrit? Sleep Breath. 2006;10:15560. [PMID: 16770648] 57. Gordeuk VR, Sergueeva AI, Miasnikova GY, Okhotin D, Voloshin Y, Choyke PL, et al. Congenital disorder of oxygen sensing: association of the homozygous Chuvash polycythemia VHL mutation with thrombosis and vascular abnormalities but not tumors. Blood. 2004;103:3924-32. [PMID: 14726398] 58. Gordeuk VR, Stockton DW, Prchal JT. Congenital polycythemias/erythrocytoses. Haematologica. 2005;90:109-16. [PMID: 15642677] 59. Sayyah J, Sayeski PP. Jak2 inhibitors: rationale and role as therapeutic agents in hematologic malignancies. Curr Oncol Rep. 2009;11:117-24. [PMID: 19216843] 60. Atallah E, Verstovsek S. Prospect of JAK2 inhibitor therapy in myeloproliferative neoplasms. Expert Rev Anticancer Ther. 2009;9:663-70. [PMID: 19445582] 61. Mesa RA, Niblack J, Wadleigh M, Verstovsek S, Camoriano J, Barnes S, et al. The burden of fatigue and quality of life in myeloproliferative disorders (MPDs): an international Internet-based survey of 1179 MPD patients. Cancer. 2007;109:68-76. [PMID: 17123268] 62. Silver RT. Long-term effects of the treatment of polycythemia vera with recombinant interferon-alpha. Cancer. 2006;107:451-8. [PMID: 16804923] 63. Kiladjian JJ, Cassinat B, Chevret S, Turlure P, Cambier N, Roussel M, et al. Pegylated interferon-alfa-2a induces complete hematologic and molecular responses with low toxicity in polycythemia vera. Blood. 2008;112:3065-72. [PMID: 18650451] 64. Segel N, Bishop JM. Circulatory studies in polycythaemia vera at rest and during exercise. Clin Sci. 1967;32:527-49. [PMID: 6028131] www.annals.org Annals of Internal Medicine Appendix Table. Causes of Absolute Erythrocytosis and Relative Erythrocytosis Causes of absolute erythrocytosis Hypoxia High-affinity hemoglobins High altitude Pulmonary disease Right-to-left shunts Sleep apnea Neurologic disease Renal disease Renal artery stenosis Focal sclerosing or membranous glomerulonephritis Renal transplantation Tumors Hypernephroma Hepatoma Cerebellar hemangioblastoma Uterine fibromyoma Adrenal tumors Meningioma Pheochromocytoma Drugs Androgenic steroids Recombinant erythropoietin Familial (with normal hemoglobin function) Chuvash ethnicity Erythropoietin-receptor mutations 2,3-Bisphosphoglycerate deficiency Polycythemia vera JAK2 V617F JAK2 exon 12 mutations Causes of relative erythrocytosis Loss of fluid from the vascular space Emesis Diarrhea Diuretics Sweating Polyuria Hypodipsia Hypoalbuminemia Capillary leak syndromes Burns Peritonitis Chronic plasma volume contraction Hypoxia from any cause Androgen therapy Recombinant erythropoietin therapy Hypertension Tobacco use Pheochromocytoma Ethanol abuse Sleep apnea www.annals.org 2 March 2010 Annals of Internal Medicine Volume 152 • Number 5 W-95