Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Occup. Med. Vol. 50, No. 7, pp. 512-517, 2000
Copyright © 2000 Lippincott Williams & Wilkins for SOM
Printed in Great Britain. All rights reserved
0962-7480/00
Burnout syndrome: a disease of
modern societies?
A. Weber and A. Jaekel-Reinhard
Institute and Outpatient Clinic for Occupational, Social and Environmental
Medicine of the University of Erlangen-Nuremberg, Germany
In the light of social change and a transformation in the work situation, interest in the
problem of burnout has grown over the past decade. There is a conspicuous
discrepancy, however, between what is regarded as certain knowledge and what is
published opinion. To date, there is no generally accepted definition of burnout, or
binding diagnostic criteria. According to the most common description at present,
burnout syndrome is characterized by exhaustion, depersonalization and reduced
satisfaction in performance. Because of its aetiopathogenesis, burnout is today mainly
regarded as the result of chronic stress which has not been successfully dealt with. This
paper gives an overview of the current definition for burnout syndrome and states
possible contemporary hypotheses for its aetiology. By examining diagnostic criteria
and possible therapies, methods of prevention are discussed. There is an urgent need
for further investigations to determine whether burnout syndrome is a work-related
disease.
Key words: Burnout; disability management; person-environment misfit; stress at the
workplace; work-related diseases.
Occup. Med. Vol. 50, 512-517, 2000
Received 15 March 2000; accepted in final form 21 June 2000.
INTRODUCTION
'... I'm under a lot of stress, ... completely burned out
..., I'd like to pack it in ..., my battery is flat...!'. Who
has not heard similar comments when people are talking
about their work? Are such statements, which are as
much part of a modern service society as the mobile
phone and computer, just everyday phrases, excuses for
a lack of performance, or are they symptoms of a disease
which can be summarized by the term 'burnout
syndrome'?
The term 'burnout' was coined in the USA a good 25
years ago. The psychoanalyst Freudenberger, for example, published one of the first scientific descriptions of
the burnout syndrome as psychiatric and physical
breakdown.1 In 1981, Maslach introduced a furtherreaching definition and an instrument for measuring
burnout which is still the most frequently used today, the
Maslach Burnout Inventory.2'3
In industrialized countries, public interest in the
problem of burnout has increased over the last few
years. The subject has enjoyed a boom in the media, but
there is a great discrepancy between published opinion
Correspondence to: Priv.-Doz. Dr. med. Andreas Weber, Schillerstr. 25 +
29, 91054 Ertangen, Germany. Tel: +49 9131 8526118; fax: +49 9131 85
22317
and what is regarded as certain knowledge. In the last
decades burnout was a subject of scientific research
mainly among psychologists and sociologists. Major
contributions for identifying and classifying burnout
syndrome have been published by psychologists.3'4
Recently, the subject has caught the attention of
doctors of social and occupational medicine. The central
problems for science and practice result from the fact
that there is no generally accepted definition of burnout.
The separation from other health disorders is difficult
and potential causal factors are still the subject of much
controversy.2'5 ~8 Nevertheless, burnout syndrome is an
important problem in modern working environments
and is addressed in this paper from the point of view of
occupational medicine. By considering the important
work published by psychologists an interdisciplinary
approach would facilitate the understanding of burnout
syndrome in the field of occupational health.
DEFINITION: THE CURRENT SCIENTIFIC
CONSENSUS OF OPINION
According to one of the first more extensive characterizations by Maslach and Jackson, burnout is the result of
chronic stress (at the workplace) which has not been
successfully dealt with. It is characterized by exhaustion
and depersonalization (negativism/cynicism) and is
A. Weber and A. Jaekel-Reinhard: Burnout syndrome
found predominantly in caring and social professions
(e.g. social workers, teachers, nurses, doctors, dentists).3
A later definition based on the MBI and which is in
widespread use today, describes exhaustion, depersonalization, and reduced satisfaction in performance as the
decisive elements of burnout syndrome.2'9 In the 10th
revision of the International Classification of Diseases
(ICD 10) the term 'burnout' was described under Z.73.0
as 'Burnout-state of total exhaustion'.10 In addition to
the question of a uniform, generally accepted definition,
aetiological and pathogenetic aspects are the subjects of
much controversy. It is generally believed today that
'negative stress' (distress) probably represents a key
phenomenon in the aetiopathogenesis of burnout. Other
important pathogenetic factors are thought to be 'being
swamped by daily routine' and 'disappointed expectations'.2'5'6'8'11'12 Most of the theories and models for the
development of burnout syndrome are published in the
psychological, psychosomatic and psychiatric literature.3'4 This paper will focus on three main models from
a social-medical point of view (Box 1).
BOX 1. Burnout syndrome: important
aetiopathogenetic concepts from the social-medical
point of view
A. Result of stress that has not been successfully
dealt with.
Emphasis on strain and society-the 'macrolevel'.
B. Person-environment-misfit.
Emphasis on interaction between society and the
individual-the 'mesolevel'.
C. Discrepancy between expectations and reality.
Emphasis on strain and the individual-the
'microlevel'.
Contrary to earlier observations regarding the epidemiology of burnout, it has been noted that the syndrome
is not associated with certain workplaces, circumstances,
sex or age. The occurrence of burnout syndrome has
been described in diverse occupations, e.g. in social
workers, advisors, teachers, nurses, laboratory workers,
speech therapists, ergo therapists, doctors and dentists,
police and prison officers, stewardesses, managers, and
even in housewives, students and unemployed people. 2 ' 11 ' 13 " 18 Psychological explanations assume that in
most of these occupations the combination of caring,
advising, healing or protecting, coupled with the
demands of showing that one cares, is of central
importance.4'8
The prevalence rates published in the literature for
individual occupations must be regarded sceptically, as
the definitions and diagnostic criteria used are not
uniform. Depending on the evaluation instruments and
classification systems used, an incidence of burnout in
teachers of up to 30% has been given.17'19 For doctors
and dentists more recent studies give prevalence rates of
up to 10%.5>11'13-15
IMPORTANT ASPECTS IN THE
AETIOPATHOGENESIS OF BURNOUT
Despite numerous new discoveries regarding the development of burnout syndrome, many questions still remain
unanswered. Is burnout merely high-level stress at the
workplace or the result of the complex interaction of social
factors (circumstances) and individual factors (behaviour)? Without a doubt, the changes in society and work
have led not only to changed demands, but also to a
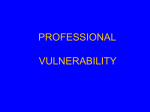
generally undisputed increase in heterogenic psychomental and psychosocial stress.20"22 Occupational psycho-mental/psycho-social stress factors are illustrated in
Fig. 1 and include pressure of time, overtime and shift
Figure 1. Burnout: an interaction between society and the working environment.
Society
Work environment
individualization
•
loss of traditional
support systems
•
globalization/competition
•
increased work complexity
anonymity
mechanization
• job uncertainty ('hire and
fire')
educational
expectations
lack of time
513
Economization
•
mobility/flexibility
•
specialization
multiple stress factors
Increase of psychosocial/psychomental stress
Higher burnout risk
514
Occup. Med. Vol. 50, 2000
work, as well as mobbing, economic pressures, and
multiple tasks such as job, family and leisure activities. In
addition, the importance of personal competence, particularly in the so-called tertiary sector, is continually
increasing (e.g. communicability, being able to work in a
team, frustration tolerance, service orientation, flexibility).
According to the job-strain model, which has been
established for many years in occupational medicine as a
stress - strain concept, a high level of strain can result
from the cumulation of psycho-mental/psycho-social
stress and a lower level of stress tolerance, which in this
context is to be regarded as 'negative stress'. When
'negative stress' becomes chronic and is not dealt with
adequately it leads to adverse effects on the health. Not
only do psychological and social factors play a role, but
so also do biological and biochemical factors. Above all,
hormonal and endocrinological changes, particularly a
permanent increase in the cortisol level and disturbances
in the hypothalamic - pituitary -adrenal control system,
are under discussion.23"28
Recent research suggests that such influences are
possibly not only relevant for the development of
burnout syndrome, but also in the pathogenesis of
occupation-related psychiatric/psychosomatic diseases.17'29'30 According to the 'person-environmentmisfit' concept, an imbalance between psycho-mental/
psycho-social stress and individual stress tolerance is
decisive for the development of burnout syndrome. The
risk of burnout is influenced not only by the extent of the
stress factors and deficits in personal resources, but
above all by 'social support' systems and 'coping'
strategies. In addition to primary personality structure
(e.g. idealism, perfectionism, timidity, insecurity, emotional instability), negative factors which influence the
individual stress tolerance are inadequate or lacking
strategies to deal with stress, disappointed expectations/
negative experiences, and lifestyle (e.g. inadequate
support due to a lack of social relationships/partnerships).6
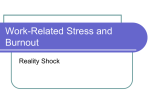
Figure 2. Burnout: a dynamic process ('burnout cascade').
1.
Hyperactivity
2.
Exhaustion
- chronic fatigue, loss of energy
3.
Reduced
activity
- withdrawal, resignation
4.
Emotional
reactions
- aggression
- negativity
- cynicism
5.
Breakdown
- cognitive function
- motivation
- creativity
6.
Degradation
- emotional distress
- loss of social contacts
7.
Psychosomatic
reactions
- sleep disturbances
- gastro-intestinal disorders
- susceptibility to infection
- sexual disorders
- intake of alcohol and drugs
8.
Despair
- psychosomatic disorders
- suicide
In addition, depending on the duration and severity of
the burnout, there are often further negative social
consequences. These include, from the point of view of
the individual, withdrawal at the workplace (so called
'inner resignation') or effects on private life (partner/
sexual problems, social isolation). From the perspective
of society, there is an increased risk of repeated or long
periods of absence from work and early invalidity.2,6,8,11,15
SYMPTOMS
DIAGNOSIS, DIFFERENTIAL DIAGNOSIS, AND
THERAPY
The symptoms of burnout patients are usually multidimensional with several psychiatric, psychosomatic,
somatic and social disorders. The main psychiatric
symptoms are, in addition to chronic fatigue and
continuous exhaustion, above all described as 'mental
dysfunction'. This includes concentration and memory
disturbances (a lack of precision, disorganization), a
lack of drive and personality changes (a lack of
interest, cynicism, aggressiveness). Severe disturbances
are anxiety and depressive disturbances, which can
culminate in suicide. Also the development of addictions (e.g. alcohol, medicines) has been associated
with burnout. Common somatic symptoms are headaches, gastro-intestinal disorders (irritable stomach,
diarrhoea), or cardio-vascular disturbances such as
tachycardia, arrhythmia, and hypertonia. Figure 2
illustrates the dynamic process of developing burnout
syndrome.
In view of the mainly unspecific symptoms, when it
comes to the diagnosis of burnout syndrome a differentiated, all-encompassing approach is necessary. Good
interdisciplinary co-operation and communication between the parties involved in the diagnostic process
(patient, GP, specialist, works physician, psychologist,
other disciplines) is just as essential as medical expertise.
Box 2 shows a diagnostic approach for diagnosing
burnout syndrome from social and occupational medicine points of view.
Valid objectification and quantification of health
impairments and/or functional disturbances must be
carried out. This requires medical expertise and should
not be carried out by non-medical personnel, even if they
are very enthusiastic about the subject. In addition to a
general anamnesis to evaluate previous and accompanying illnesses, a problem-oriented social and occupational
anamnesis in particular should be carried out. This
A. Weber and A. Jaekel-Reinhard: Burnout syndrome
515
BOX 2. Burnout syndrome: the diagnostic, all-encompassing, interdisciplinary approach
Medical history
Social and occupational history
Drug history
Symptoms
Physical examination
Psychosomatic/psychiatric status
Psychometric tests
Special laboratory tests
Previous and current diseases
Identification of potential stress factors and possible social consequences
Smoking, consumption of alcohol and drugs
Course and temporal relationship
General examination
Maslach Burnout Inventory
'Stress biomonitoring'; hypothalamic - pituitary -adrenal control system
serves both to identify potential stress factors and to
evaluate possible negative social consequences in the
person's private life and occupation. In addition, consumption of alcohol or drugs must be documented, and
if necessary quantified using biological monitoring. The
subjective symptoms should be described in as much
detail as possible, noting any changes over time. A
physical examination (internal status) is also essential,
and should be supplemented by results for important
routine laboratory parameters (e.g. blood count, liver
function tests, electrolytes, kidney function) if this
information is not already available. In addition, in
individual cases, 'stress-biomonitoring' (e.g. cortisol
level/daily profiles) and special immunological and/or
endocrinological analyses (e.g. cellular/humeral immune
system, hypothalamic-pituitary-adrenal control system) must be considered. Such investigations can,
however, only be carried out by specialized centres.
An early psychosomatic/psychiatric consultation and
the carrying out of psychometric test procedures are
recommended. The Maslach Burnout Inventory, introduced in 1981, is widely used in the diagnosis of
burnout. It is a self-assessment questionnaire consisting
of 22 items to evaluate emotional exhaustion, depersonalization and dissatisfaction with performance.3 In
individual cases further psychometric investigations, also
to evaluate competing influences, may be necessary. It
must be remembered, however, that the results of such
test procedures are only 'pieces in the diagnostic mosaic'
and cannot replace qualified psychosomatic/psychiatric
investigation. Therefore an interdisciplinary team should
be required in the diagnosis of burnout syndrome.
Differential diagnosis must be used to first separate
primary psychiatric disorders, i.e. those independent of
exogenous factors, and burnout. Furthermore, chronic
somatic diseases, such as chronic infections (e.g. viral
hepatitis), endocrinopathy (e.g. thyroid disorders, Addison's disease), auto-immunopathy, tumours or the socalled chronic fatigue syndrome (CFS) must not be
forgotten. Differentiation between burnout and CFS
can, however, be rendered impossible by similar symptoms and a comparable course of the disease.31
In practice, the diagnostic assignment to burnout
syndrome of the mainly unspecific symptoms described
above is problematic, even with a differentiated approach. It is very difficult to find temporal and causal
relationships to previous psycho-mental/psycho-social
stress when, as is often the case, the illness has existed
for a long time; there are multiple symptoms and many
different influencing factors. Objectification or quantification of occupational stress factors is almost impossible
for a GP or specialist, as they usually do not have
sufficient information or detailed knowledge of the
workplace situation. But even with optimum co-operation between the patient's doctors, occupational physicians and psychologists there are still general
methodological problems in the evaluation of negative
stress at the workplace. In addition, it must be noted that
occupational and non-occupational stress factors are
often interlinked or cannot be separated from each other
as regards their biological consequences. Therefore, not
only the validity of the diagnosis 'burnout syndrome', but
also the decisive meaning of a harmful work situation still
remains at the centre of criticism.
To date there has been no scientific evaluation of the
suggestions published in the literature concerning the
therapy of burnout. In addition, there is often no clear
division between treatment and preventive measures.6'7
The procedures used and their dependence on the type
and severity of the symptoms are listed in Box 3.
PREVENTION
Measures to prevent burnout can be differentiated
according to the preventive approach and levels of
prevention. Preventive approaches to be considered are
both modifications in the working environment (prevention of circumstances) and also improvements in the
individual's ability to cope with stress (behavioural
preventive measures). According to the WHO the levels
BOX 3. Burnout syndrome: therapy suggestions
Pharmacological treatment according to
symptoms, e.g. antidepressants, beta-blockers
Psychotherapy, such as relaxation techniques,
improvement of self-esteem, concepts for dealing
with stress
Reorganization of the work environment, such as
the organization of work and the work structure,
and the introduction of time management
Change of work environment, combined with
rehabilitation and retraining
516
Occup. Med. Vol. 50, 2000
of prevention can be divided into primary preventive
measures (avoidance/removal of factors that make the
patient ill), secondary measures (early recognition—intervention of manifest disease), and tertiary measures
(coping with the consequences of disease—rehabilitation
and relapse prophylaxis).32 The concepts for behavioural
preventive measures presented in the literature focus on
primary prevention and are the 'domain' of psychology.
Some of the measures are:
•
•
•
•
•
improvements in dealing with stress,
the learning of relaxation techniques,
the delegation of responsibility (learning to say 'no'),
hobbies (sport, culture, nature),
trying to uphold stable partnerships/social relationships,
• frustration prophylaxis (reducing false expectations).4
In addition, some authors regard religion and spirituality as having a potentially preventive function/'6
The strategies discussed at present for preventing the
circumstances in which burnout arises are a combination
of primary and secondary prevention. It can be
differentiated between activities where the focus is on
work organization and management, and suggestions
aimed primarily at (groups of) persons.33 Workplacerelated measures are:
• the creation/preservation of a 'healthy working environment' (e.g. time management, communication style
of leadership),
• the recognition of performance (praise, appreciation,
money),
• the training of managers ('key role' of the boss in
burnout prevention).
Person-oriented strategies are:
• the carrying out of 'suitability tests' before job
training,
• specific programmes accompanying the work of
persons from risk groups (e.g. Balint groups for
teachers and doctors),
• regular occupational—medical/psychological monitoring (e.g. establishment of a special 'job-stress' checkup for the early recognition of burnout).
Suitability tests are not likely to be favourably received
from a socio-political point of view. First of all they do
not allow freedom of choice when it comes to occupation, even if, depending on their type and content, they
could be useful from a medical point of view (it is known
from practice that persons with the personalities susceptible to developing burnout choose the occupations with
a higher risk of developing burnout).
Of particular interest is the suggestion of regular
occupational-medical/psychological monitoring of occupational groups at risk of developing burnout. The
occupational-medical management of persons at risk
from stress, and burnout patients, would therefore gain a
standardized framework. In addition, a general increase
in knowledge could be expected, based on well-founded
observations.34"36
In times of limited resources, acceptance and feasibility also play an important role in the development and
implementation of preventive strategies. In addition, it
should not be forgotten that effective and efficient
prevention requires adequate knowledge of the aetiopathogenesis. The closing of gaps in our knowledge
would also be a great improvement for the prevention of
burnout.33'37
CONCLUSIONS: PROSPECTS
As a result of the gaps in our knowledge, there is a
great temptation to dismiss burnout as merely a
'fashionable trend' or an 'invention of the media'. In
addition, in the era of molecular medicine, it may seem
more sensible to some people to leave psychosocial
health risks to psychologists, sociologists or 'health
scientists'. It should be warned that this kind of
thinking takes away an important dimension from
medicine (the social dimension).38 Without a doubt the
multiplicity of the burnout phenomenon requires
intensive interdisciplinary cooperation with the simultaneous preservation of its unity. Medical expertise is
essential here. Moreover, burnout, as the result of the
complex interaction of work/society and the individual,
calls for social-medical and occupational—medical
competence, and also serves to illustrate the close
relationship of these two disciplines.38 It must also be
borne in mind that the numerous possible social
consequences of burnout (e.g. repeated absence from
work, early invalidity) are also of 'classical' socialmedical and occupational-medical content. Social medical and occupational-medical 'know-how' should
not, however, be limited to the analysis of deficits, but
should lead to the drawing up of constructive,
scientifically based solutions. The first priority is to
reach a consensus regarding the use of uniform
definitions and diagnostic criteria. Only in this way
can valid statements be made on prevalence rates in
certain occupational groups, and thus on the extent of
the risk. Furthermore, it is important that epidemiological studies are planned sensibly to reveal potential
causal relationships with psycho-social/psycho-mental
stress at work. Merely asking for subjective evaluations
using a questionnaire does not lead any further.
Methodologically valid prospective longitudinal studies
of an interdisciplinary and comprehensive nature,
which evaluate both subjective and objective data, are
urgently required. In addition, research to reveal the
decisive pathogenetic principles should, of course, not
be neglected. Above all, further research into the
biological, biochemical and molecular effects of chronic
exposure to stress (e.g. endocrinological investigations
of the hypothalamic - pituitary -adrenal control system,
further development of 'stress-biomonitoring', psychoimmunology) is needed.27
The gaps in our knowledge should not excuse us from
trying to carry out in practice preventive measures and
A. Weber and A. Jaekel-Reinhard: Burnout syndrome
517
18. Spiessbach B, Knebelau M, Bender S. Callcenter—Hoffnungstrager oder Belastungstra'ger? ErgoMed 1999; 23:
246-252.
19. Scheuch K, Vogel H. Pravalenz von Befunden in ausgewahlten Diagnosegruppen bei Lehrern. Soz Prdventivmed
1993; 38: 20-25.
20. Bourbonnais R, Comeau M, Vezina M, Dion G. Jobstrain,
psychological distress and burnout in nurses. AmJIndMed
1998; 34: 20-28.
21. Lehnert G, Valentin H. Arbeits—und Betriebsmedizin
zwischen Selbstverantwortung und Fremdbestimmung.
Arbeitsmed Sozialmed Umweltmed 2000; 35: 14-20.
22. Valentin H. Gesundheit und Krankheit an den Arbeitsplatzen der Zukunft. Zbl Arbeitsmed 1991; 41: 182-192.
23. Karasek R. Job demands, job decision latitude and mental
strain: Implications for job redesign. Adm Sci Q 1979; 24:
285-306.
REFERENCES
24. Kelly S, Hertzman C, Daniels M. Searching for the
biological pathways between stress and health. Annu Rev
Public Health 1997; 18: 437^62.
1. Freudenberger HJ. Staff burnout. JSoc Issues 1974; 30:15925. v. Oncill J. Stress at work. BMJ 1996; 313: 745-748.
165.
26. Orris P, Hartmann DE, Strauss P, et ai. Stress among
2. Burisch M. Das Burnout-Syndrom—Theorie der inneren
package truck drivers. AmJIndMed 1997; 31: 202-210.
Erschopfung 2. Auflage. Berlin, Heidelberg: Springer
27. Pruessner JC, Hellhammer DH, Kirschbaum C. Burnout,
Verlag, 1994.
perceived stress and cortisol responses to awakening.
3. Maslach C, Jackson SE. The measurement of experienced
Psychosomatic Med 1999; 61: 197-204.
bumout. J Occup Behav 1981; 2: 99-113.
4. Schaufeli W, Enzmann D. The Bumout Companion to Study
28. Scheuch K. Psychomentale Belastung und Beanspruchung
and Practice: A Critical Analysis. London: Taylor & Francis
im Wandel von Arbeitswelt und Umwelt. Arbeitsmed
Ltd, 1999.
Sozialmed Umweltmed 1997; 32: 289-296.
29. Niedhammer I, Goldberg M, Leclerc A, Bugel I, David S.
5. v.d. Dammerau-Dombrowski V. Das Burnout-Syndrom.
Psychosocial factors at work and depressive symptoms in
Seminar — Hausarztpraxis 1998; 16-18.
the Gazel cohort. ScandJ Work Environ Health 1998; 24:
6. Ewald O. Das Burnout-Syndrom. ErgoMed 1997; 21: 93197-205.
96.
30. Stansfeld SA, Fuhrer R, Shipley MJ, Marmot MG. Work
7. Keel P. Psychische Belastungen durch die Arbeit: Burnoutcharacteristics predict psychiatric disorder: prospective
Syndrom. Soz Prdventivmed 1993; Suppl. 2: 131-132.
results from the Whithall II study. Occup Environ Med
8. KlieserE,ScharV. Burnout-Syndrom. MMP1996; 19:171999; 56: 302-307.
20.
31. Goshorn RK. Chronic fatigue syndrome: a review for
9. Savicki V, Cooley EJ. Theoretical and research consideraclinicians. Seminars in Neurology 1998; 18: 237-242.
tions of burnout. Children and Youth Services Review 1983; 5:
32. World Health Organization. Ottawa Charter for Health
227-238.
Promotion. An International Conference on Health Promotion.
10. Deutsches Institut Fur Medizinische Dokumentation und
The Move Towards a New Public Health. Ottawa: WHO,
Information (DIMDI) (Hrsg.). 1CD-10—Internationale
1986.
statistische Klassifikalion der Krankheiten und verwandter
Gesundheitsprobleme Revision. Band I: Systematisches Ver- 33. Weber A. Sozialmedizinische Evaluation gesundheitlich bedingter Fruhpensionierungen von Beamten des Freistaates
zeichnis. Munchen: Urban u. Schwarzenberg, 1994.
Bayern. Stuttgart: Gentner Verlag, 1998.
11. Felton JS. Burnout as a clinical entity—its importance in
34. Blome O. Arbeitsbedingte Erkrankungen—arbeitsbedingte
health care workers. Occup Med 1998; 48: 237-250.
Gesundheitsgefahren—ein Spannungsfeld fur die Unfall12. Goiter RC. Burnout among dentists: identification and
versicherung. ErgoMed 1998; 22: 168-175.
prevention. Amsterdam: Thele Thesis, 1999.
35. Blome O. Arbeitsbedingte Erkrankungen—§ 3 BKV.
13. Chan DW, Hui KP. Burnout and coping among Chinese
ErgoMed 1998; 22: 276-282.
secondary school teachers in Hongkong. BrJEduc Psychol
36. Borsch-Galetke E. Arbeitsbedingte Gesundheitsgefahren
1995; 65: 15-25.
und Erkrankungen—wo besteht Handlungsbedarf? Ergo
14. Cooper CL, Kelly M. Occupational stress in head teachers:
Med 1999; 23: 31-33.
a national UK study. BrJEduc Psychol 1993; 63: 130-143.
15. Goner RC, Albrecht G, Hoogstraten J, Eijkman MAJ.
37. Kentner M. Gesundheitsreform 2000—Welchen StellenProfessional burnout among Dutch dentists. Community
wert hat die arbeitsmedizinische Prevention? Arbeitsmed
Dent Oral Epidemiol 1999; 27: 109-116.
Sozialmed Umweltmed 1999; 34: 275-276.
38. Weber A, Lehnert G. Sozialmedizin—Warum eigentlich?
16. Rottenfusser R. Viele Kassenarzte fuhlen sich ausgebrannt.
Ein Pladoyer fur die soziale Dimension in der HumanDt Arztebl 1999; 96: A610-613.
medizin. Arbeitsmed Sozialmed Umweltmed 1999; 34: 49217. Soderfeldt B, Soderfeldt M, Ohlson CG, Warg LE.
498.
Psychosomatic syndromes in human service work. ScandJ
SocMed 1996; 24: 43-49.
medical care to the best of our abilities. Burnout patients
need competent help and should feel that their complaints are taken seriously. Even in times of limited
resources, comprehensive clarification of the complaints,
while avoiding the too early fixation with certain causal
relationships, is important.
On the threshold to the 21st century burnout is a
challenge to both research and practice, and not only
because doctors can potentially be affected. Specialists of
social medicine and occupational medicine should not
miss the chance of acting in interdisciplinary teams with
psychologists to investigate together the problem of
burnout syndrome.