Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
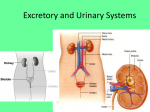
2/26/2014 The Evidenced-Based Approach to Managing Postoperative Urinary Retention (POUR) Lara Beth Conner, RN, MSN, ONC Charla B. Johnson, RN, MSN, ONC Conflict of Interest We hereby certify that, to the best of our knowledge, no aspect of our current personal or professional situation might reasonably be expected to affect significantly our views on the subject on which we are presenting, other than the following. Objectives O Identify three risk factors associated with POUR O Discuss the assessment and treatment of POUR 1 2/26/2014 Poll Question #1 O The first urge to void is felt at ___cc’s? O 150 O 200 O 300 O 500 Bladder Function: Normal Physiology of Urination O Urinary System O Bladder fills with urine at approximately 0.5 ml/kg/hour O The bladder wall is stretched when volume reached (200-400ml) O Nerve impulse travels to the spinal cord and to brain signaling that the bladder is full. O To empty the bladder, a nerve impulse to bladder muscle and urinary sphincters O Detrusor muscles contracts and sphincters open To brainstem From brainstem Sensory afferent Brain Sympathetic ganglion Somatic efferent (tonic) Sympathetic postpost-ganglionic (tonic) Parasympathetic ganglion Bladder Stretch receptor Sphincters Int. Ext. Urethra 2 2/26/2014 Steps to the Normal Voiding Cycle Definition of POUR The inability to void with a full bladder O Acute Urinary Retention O Acute-on-Chronic Retention O Chronic Retention Acute Urinary Retention O Anatomical Retention O Functional Retention O Psychogenic Retention 3 2/26/2014 Poll Question #2 O Which of the following is not a predisposing risk factor for POUR? O Male O Diabetes O Immobility O Age over 50 Risk Factors O Predisposing- Preoperative risk factors O Age & Gender O Age over 50 O Male Consequences of Aging Normal O Bladder capacity: 400 – 600 mL O Desire to void at 250 – O O O O 300 mL 300 –400 mL per void Residual < 50 mL 1/3 voided volume at night No straining, hesitation, pain or post-void dribble Changes with Aging O Bladder capacity 250 – 300 mL O Same or less O Total volume voided per void decreases O Residual < 100 mL O Up to 2/3 voided volume after 8 PM O No straining, pain, or post-void dribble 4 2/26/2014 Risk Factors O Predisposing – Preoperative risk factors O Co morbidities O Neurological conditions O Alcohol intake O Constipation O Renal disease O Urethral strictures O Chronic UTI O Diabetes Risk Factors O Predisposing – Preoperative risk factors O Co morbidities O Medications O Antipsychotic drugs O Antidepressants O Benzodiazepines O NSAIDS O Calcium channel blockers O Anticonvulsants O Opioids Risk Factors O Precipitating – Intraoperative and Postoperative Factors O Duration of surgery O Excessive fluid intake (>750cc) O Anesthesia O Analgesia 5 2/26/2014 Poll Question #3 O Do you routinely use a bladder scanner in clinical practice? O Yes O No Assessment O Voiding Status O Fluid Balance O Clinical Exams Voiding Status O Spontaneous Voiding O Amount Voided O Bladder Scanning 6 2/26/2014 Lower Urinary Tract Storage &Emptying Symptoms O O O O O O O O O O O Dysuria Frequency Incontinence Pressure Urgency Hesitancy Incomplete Emptying Intermittent- stream Post-void dribbling Straining to void Weak stream Ask…. Do you have a feeling or urge/sensation to void? Character of the stream? Strains or bears down when voiding? Once on the toilet, can the patient initiate the stream within a minute? Fluid Balance O Intra-operative O Oral Intake O Blood Output O Urine Output Clinical Exam O Frequent Inspection O Palpation of the Bladder O Percussion O Bladder Scanner Technique 7 2/26/2014 Bladder Scanner Technique Prepare the patient Bladder Scanner Technique Bladder Scanner Technique 8 2/26/2014 Bladder Scanner Technique Bladder Scanner Technique Bladder Scanner Technique 9 2/26/2014 Bladder Scanner Technique 286 ml Bladder Scanner Technique We thank our Model for allowing us to demonstrate a bladder scanning technique Poll Question #4 O When would you perform in and out catheterization? O Bladder scan equal to or greater than 600 cc O Patient discomfort O 8 hours post-op 10 2/26/2014 Interventions to Assist with Spontaneous Voiding O Early Mobilization O Offering Toileting O Bedside Commode O Privacy O Offering Caffeinated Fluids (if appropriate) Treatment Indwelling versus Intermittent O Initially managed with Indwelling O Remove quickly as possible O Intermittent while waiting for voiding function resolution Goal: Allow the bladder to store a reasonable volume of urine at low pressure, and empty it at appropriate intervals if the patient is not adequately voiding. Poll Question #5 O Does your institution have a risk assessment tool in place to assess for patients at risk for POUR? O Yes O No 11 2/26/2014 Best Practice O Institution Guidelines and Protocols O Peri-operative Risk Assessment O Indwelling catheters in high risk patients O Use of silver alloy catheter O Insertion technique O Catheter size O GU Assessment O SCIP Catheter Care O Aseptic Technique O Securement Devices O Perineal Care O Catheter Removal at 24 Hours The Key is Prevention!!! NAON Practice Point 12 2/26/2014 13 2/26/2014 Case Study #1 O 83 year old male with THA O PMH: BPH, angina, HTN, diverticulitis, renal disease, arthritis, TIA, hyperlipidemia O Intra-op fluids 2400 cc O BUN, Cr O Foley cath placed in OR due to high risk Case Study #1 O Foley removed POD 2, reinserted @ MN O Foley removed POD 3 @ 12:48 pm O Foley reinserted POD 4 @ 5:30 am, removed @ MN O Flomax; urology consult What went wrong in this case? Case Study #1 O Bladder scan not done O Flomax not started until POD 4 O Indwelling instead of intermittent catheter O Voiding volumes not recorded 14 2/26/2014 Case Study #2 O 72 year old female, TKA O PMH: renal CA/nephrectomy, diabetes, HTN, hyperlipidemia, urinary retention O BUN, Cr O Intra-op fluids 2400 cc Case Study #2 O Procedure ended @ 8:59 am O Foley inserted @ 8:30 pm O Foley removed POD 2 @ 6:40 am O Bladder scan = 610 cc @ 3:30 pm, intermittent cath O Intermittent cath repeated @8:30 = 400 cc What went wrong in this case? Case Study #2 O Foley not inserted in OR O Foley not inserted until > 11 hrs postop O No bladder scan until 9 hrs after catheter removal O No documentation on voiding volumes after last intermittent cath 15 2/26/2014 References O Fleming, R. (2013). The development of post-operative urinary guidelines. The Dissector, 40 (4), 22-24. O Gallo, S. DuRand, J. & Pshon, N. (2008). A study of naloxone effect on urinary retention in the patient receiving morphine patient controlled analgesia. Orthopaedic Nursing, 27 (2), 111-115. O Hansen, B.S., Soreide, E., Warland, A.M., & Nilsen, O.B. (2011). Risk factors of post-operative urinary retention in hospitalized patients. Acta Anaesthesiologica Scandinavica, 55, 545-548.doi: 10.1111/j.13996576.2011.02416. O Johansson, M. & Christensson, L. (2010). Urinary retention in older patients in connection with hip fracture surgery. Journal of Clinical Nursing, 19, 2110-2116. doi: 10.1111/j.1365-2702.2010.03261. O Johnson, C.B. & Conner, L.B. (2010). Practice Points: Post operative Urinary Retention (POUR). National Association of Orthopaedic Nursing. References O McVary, K. (2006). Non-steroidal anti- inflammatory drugs and urinary retention. Retrieved from http://wwwthelancet.com. (367) O Miller, A.G., McKenzie, J., Greenky, M., Shaw, E., Gandhi, K., Hozack, W.,Parvizi, J. (2013). Spinal anesthesia: Should everyone receive a urinary catheter? The Journal of Bone and Joint Surgery, 95, 14981503. doi:10.2106/JBJS.K.01671 O Newman, Diane K., Managing Urinary Retentaion in the Acute care Setting. February 10, 2014. http://verathon.com/portals/0/Uploads/ProductMaterials/_bsc /0900-0447-08-86.pdf O Pavlin, D.J., Pavlin, E.J., Fitzgibbon, D.R., Koerschgen, M.E., & Plitt, T.M. (1999). Management of bladder function after outpatient surgery. Anesthesiology, 91, 42-50. O Steggall, M., Treacy, C., & Jones, M. (2013). Post-operative urinary retention. Nursing Standard, 28 (5), 43-48. Question and Answers Incorporate Best Practice in your care!!! 16