Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
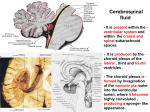
J Neurol (1996) 243 : 165 170 9 Springer-Verlag 1996 M. Rentzos C. Nikolaou A. Rombos K. Voumvourakis I. Segditsa C. Papageorgiou Received: 19 January 1995 Received in revised form: 2 May 1995 Accepted: 22 May 1995 M. Rentzos ([~) - C. Nikolaou A. Rombos - K. Voumvourakis I. Segditsa 9C. Papageorgiou Department of Neurology, Athens University Medical School, 74 Vas. Sofias Av, Athens 11528, Greece Tel 01-7220811 #218 Tumour necrosis factor alpha is elevated in serum and cerebrospinal fluid in multiple sclerosis and inflammatory neuropathies Abstract Tumour necrosis factor alpha (TNFc~) is a peptide that is derived from T lymphocytes and macrophages and is used as a marker of activated cellular immune responses. TNFcz was measured in paired sera and cerebrospinal fluid (CSF) from 30 patients with multiple sclerosis (MS) with worsening disability, 54 patients with other neurological diseases, and 20 normal subjects. A sensitive enzyme-linked i m munosorbent assay was used to determine the TNFc~ levels. We found significantly elevated serum and CSF levels in 12 (40%) and 6 (20%) MS Introduction The aetiology of multiple sclerosis (MS) has not been clearly established, although a number of immunological aberrations, such as the presence of oligoclonal immunoglobulins in cerebrospinal fluid (CSF) [32, 45], the decreased number of T-suppressor lymphocytes in the peripheral blood during acute exacerbations [48], and the presence of CD4 lymphocytes in MS plaques [58], have been reported in MS patients. Newly formed plaques in MS patients have been reported to contain T lymphocytes and macrophages at their active edges [25]. Activated T lymphocytes which circulate in sera and CSF accomplish their cytotoxic activity by producing cytokines [15, 16]. "Cytokine" is a term for a heterogeneous group of polypeptide substances which are involved in immunity, inflammation and tissue damage [6]. Tumour necrosis factor (TNFc0 is a cytokine that has been shown to be capable of selectively damaging oligodendrocytes and myelin sheaths in vitro [53] as well as being an important media- patients, respectively, compared with healthy controls (P < 0.007 and P < 0.05). Among the 18 patients with neuropathy, we also found high serum and CSF TNFt~ values in 3 (17%) and 5 (28%) patients, respectively (P < 0.04 and P < 0.002). Our study shows that TNFt~ is probably involved in the pathogenetic mechanisms of MS and other inflammatory neurological diseases. Key w o r d s Tumour necrosis factor alpha. Multiple sclerosis 9 Inflammatory neuropathies tor in several inflammatory disorders [7, 40, 42, 57]. It has been reported that in MS patients TNFt~ is produced by sera and CSF circulating activated macrophages [39]. In the present study, serum and CSF TNFc~ levels were measured in 30 MS patients, 45 patients with other neurological diseases and in 20 controls in order to examine the correlation of this cytokine with the immunological disturbances in MS. Patients and methods Serum and CSF samples were studied in 95 individuals comprising the following groups: (1) 30 MS patients (12 men, 18 women, aged 17-57 years, mean 34); (2) 54 patients with other neurological diseases (20men, 34 women, aged 18-78 years, mean 59): 7 of these patients had motor neuron disease, 6 were epileptic, 8 had cerebrovascular disease, 9 had progressive dementia (7 with Alzheimer's disease and 2 with multi-infarct dementia), 6 had Parkinson's disease and 18 had neuropathy [5 with chronic inflammatory demyelinating polyradiculoneuropathy, 3 with diabetic neuropathy, 1 with post-herpetic cranial neuropathy, 1 with paraneoplastic neuropathy, 2 with Guillain-Barr6 syndrome (GBS), 2 with cranial 166 mononeuritis of unknown aetiology, 1 with hereditary amyloid neuropathy and 3 with chronic polyneuropathy of unknown aetiology]; (3) 20 individuals (12 men, 8 women, aged 40-80 years, mean 55) who were hospitalized for backache and headache and who had no evidence of organic neurological disease, studied as a control group. Of the 30 MS patients, 28 had clinically definite disease according to the criteria of Poser et al. [47]; of these patients 16 had the relapsing remitting (RR) and 12 the chronic progressive (CP) type. Two patients had retrobulbar neuritis. The clinical diagnosis of MS was based on clinical signs supported by objective findings including the presence of inflammatory lesions as confirmed by magnetic resonance imaging (MRI), as well as the presence of oligoclonal bands and increased IgG level in the CSF. The diagnosis of chronic inflammtory demyelinating polyneuropathy (CIDP) was made according to the criteria of Dyck et al. [8]. This diagnosis was based on the patient's history, clinical findings, nerve conduction studies and CSF examination. None of the MS patients had taken any corticosteroids or immunosuppressive medication, nor had plasmapheresis been performed for at least 6 months before their serum and CSF were sampled. Blood and CSF samples were taken within 7 days of an acute exacerbation of the disease, were immediately centrifuged to remove cells and prevent cytokine leakage from the intercellular compartment, and were stored at - 7 0 ~ until TNFor measuremtns were made. All CSF samples were subjected to a cell count by Rosenthal plate. The IgG index was quantified by nephelometry. The blood-CSF barrier status was assessed by calculating the CSF/serum albumin ratio 134]. 0.3 0.25 0.2 d 0 9 0.15 0 . 1 84 0.05- 1 3 4 5 6 7 8 Fig. 1 Serum tumour necrosis factor alpha (TNFo0 values in all groups (1 multiple sclerosis, 2 motor neuron disease, 3 epilepsy, 4 cerebrovascular disease, 5 dementia, 6 Parkinson's disease, 7 neuropathy, 8 controls, OD optical density) 0.25- 0.2 TNF assay Levels of TNFc~ in serum and CSF were measured by a sensitive sandwich-type enzyme-linked immunosorbent assay (ELISA) with a purified monoclonal antibody to the human TNFcz and rabbit polyclonal antihuman TNFo~ antibody (Genzyme). The standard curve obtained with recombinant TNFo~ ranged fi-om 0 to 1200 pg/ml. Optical densities were determined by means of a microELISA reader (L.P 400, Pasteur diagnostics). The absorbance of each well was read at 450 nm. CSF and sera were assayed at dilutions of 1:2. The limit of detection was 10 pg/ml. 2 0.15 6 6 0.1- 0.05Statistical analyses The statistical method applied was the Student's test, since TNFo~ values had normal distribution. P values of < 0.05 were considered significant. Results The levels of TNFc~ in serum and CSF ranged between 0.052-0.283 and 0.044-0.222, respectively, (Figs. 1, 2). Figures 3 and 4 summarize the mean values of TNF~x in serum and CSF respectively. Serum TNFo~ levels Serum TNFc~ values in MS patients were between 0.068 and 0.258 (mean value 0.16, SD 0.061), in patients with other neurological diseases 0.052-0.247 (mean value 0.13, SD 0.045), and in the controls 0.052-0.172 (mean 0 -1 Fig.2 2 13 4 5 6 7 8 CSF TNFor wdues in all groups (for detailed, see Fig. 1) value 0.11, SD 0.038) (Figs. 1, 3). Twelve of the 30 MS patients (5 with CP and 7 with RR) and 1 with optic neuritis (43%) had serum GNFc~ values higher than the corresponding mean values of the controls +2SD. MS patients had significantly higher serum T N F ~ levels compared with the controls (P < 0.007). MS patients with the CP type of the disease did not have significantly higher serum T N F ~ levels than those with the RR type (P < 0.8). We did not find significantly elevated TNFc~ levels in patients with other neurological diseases compared with controls, except in neuropathy patients. Of the 18 patients with neuropathy, 3 (17%) had high serum TNFc~ values compared with the controls (P < 0.043). One had post-herpetic cranial neuropathy, the second had diabetic neuropathy, and the third patient had CIDP (Fig. 1). 167 Table 1 CSF IgG index in patients with multiple sclerosis (MS) 0.20.16- No 1 0.16- 2" 0.14- 3 0.12ei 6 4 5 6 0.1- 7 8 9a 0.080.06- 10 11 12a 13 0.04- 0.020 1 2 3 4 5 6 7 8 Fig.3 Serum TNF~ mean values (for details, see Fig. 1) 14a 15 IgG index No IgG index 0.69 0.66 0.76 0.34 0.66 0.67 1.5 0.71 0.57 0.69 0.45 0.84 0.68 0.63 1.92 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 0.6 0.52 0.55 0.46 0.77 0.96 0.46 0.73 1.2 0.45 0.55 0.98 0.41 0.79 0.43 a Patients with high tumour necrosis factor alpha values 0"2I 0.18 as well (Table 1). In all MS patients the number of circulating cells in CSF did not exceed 5/mm 3. 0"16H 0.14j~ 0.12- d d Discussion 0.1 0.08 0.06 0.04 0.02 0 1 2 3 4 5 6 7 8 Fig.4 CSF TNFc~ mean values for details, see Fig. 1) CSF TNFo~ levels CSF TNF(~ values in MS patients were between 0.044 and 0.219 (mean value 0.118, SD 0.048), in patients with other neurological diseases 0.049-0.222 (mean value 0.098, S D 0.038) and in the controls 0.044-0.145 (mean value 0.093, SD 0.031) (Fig. 2, 4). High CSF TNFo~ values were measured in 6 MS patients (20%), 4 with the RR and 2 with the CP type. CSF TNFo~ values in MS patients were significantly higher than in the controls (P < 0.005). In 10 MS patients, CSF TNFc~ values were higher than the corresponding serum TNFc~ values (Fig 2). Five (28%) of the patients with neuropathy had higher CSF TNFc~ values than the controls (P < 0.002). One of these patients had diabetic neuropathy, 3 had C I D E and 1 had paraneoplastic neuropathy (Fig. 2, 4). Of 30 MS patients, 18 had an increased CSF IgG index (higher than 0.65); 4 of these had high CSF TNFc~ values There is evidence that TNFc~ is involved in the pathogenesis of MS [4]. Robbins et al. [49] reported that activated astrocytes and microglia cells can produce a substance analogous to T N F a which has a cytotoxic effect on the oligodendrocytes in vitro. According to recent studies, there is evidence that TNFot is present in MS plaques [27, 54] and that it can damage the oligodendrocytes and the myelin sheath [53]. In the present study, serum T N F a was high in 12 of 30 MS patients. High serum TNFc~ values correspond to the blood circulating activated lymphocytes and macrophages which are present at the sites of MS lesions. Serum TNFc~ values were high in both CP and RR course MS patients, and this can be explained by an equivalent lymphocyte activation in both types of the disease. It is not clear what exactly is the role of TNFc~ in MS pathogenetic mechanisms and when in MS evolution the activation of T cells and TNF(x production happens. Increased production of TNFc~ may precede clinical relapse in the RR form of MS and may thus trigger off exacerbations [3]. B and T cell mitogen-stimulated whole blood cells in patients with MS, obtained 2 weeks before to 4 weeks after clinical exacerbation, secrete 5-100 ng/ml TNFc~ when cells from patients with MS in remission and normal control subjects produce only 1-3 ng/ml TNFo~ [3]. The early (that is, before the clinical exacerbation) T N F ~ production and its gradual reduction after the relapse may be the cause of low serum and CSF T N F a values in many studies of patients with MS [13]. 168 High CSF T N F a values were found in 6 MS patients in whom a very small number of CSF circulating cells was measured. It is possible that intrathecal concentrations of TNFc~ are more important than the systemic levels during MS activity, indicating that TNFc~ can also be derived from the central nervous system. Astrocytes can become activated by viruses or endotoxins and produce TNFc~ [33, 49]. High serum and CSF T N F a values were found in 1 and 3 patients with CIDR respectively. CIDP is an immunemediated polyneuropathy in which both humoral and cellular immune responses are implicated [17, 18, 29, 31]. Interactions between the various compartments of the immune system are regulated by cytokines [1, 41]. Their role in the pathogenesis of immune-mediated polyneuropathies has not been completely explored to date. In two published reports, high serum interleukin 2 (IL2) and serum and CSF IL6 values were found in patients with GBS and CIDP [2, 19, 22, 36]. The worsening of experimental allergic neuritis (EAN) upon interferon g a m m a (IFN- 7) administration also underscores the pathogenic role that T-cell cytokines may play in inflammatory disorders of the peripheral nervous system [20]. Recently, abnormally high TNFc~ levels have been reported in the serum and CSF of patients with GBS [11, 56, 59]. In our study the number of cases is very small but the high CSF TNFc~ values in most of the CIDP patients examined may support the notion that there is T lymphocyte and macrophage activation in CIDR TNFc~ was localized by immunostaining of teased nerve fibres of rats with EAN induced either by active immunization with myelin [60] or by adoptive transfer of P2 autoreactive T cells [50]. In that condition nerve roots are infiltrated by T cells and macrophages. T N F ~ is synthesized and released mainly by activated inacrophages [51. T ceils and macrophages in EAN are believed to cause segmental demyelination by mechanisms that are still only partially understood and they have recently been shown to express INF-y in nerve roots prior to demyelination [24, 52]. INF-7 is a potent stimulus for production of TNFc~ [43]. Thus, IFN-y may be the stimulus that attracts activated TNFo~ positive macrophages. TNFo~ produced by these macrophages may cause damage to the myelin sheats, probably mediating toxic oxygen radical production which has also been shown to play an important pathogenic role in EAN [23, 24]. TNFc~ intraneural injections into peripheral nerves of C3H/HeJ mice cause axonal damage [51]. TNfot is also produced by IL2 activated macrophages in vitro and in vivo [10, 30]. TNFo~ may be secondarily released by INF-y or IL2 and may contribute to GBS pathogenesis [20-22, 56]. Monitoring and follow-up of patients with the syndrome may prove that clinical improvement is associated with a decrease in TNFc~ levels. This will provide evidence that high TNFcz levels play an important role in peripheral demyelination in GBS and are not an incidental immunological abnormality [56], TNFcz overproduction is not the unique immune-mediated interaction in that syndrome. Both cellular and humoral immune mechanisms and complement cascade activation may result in the inflammatory demyelinating process [28]. In a study referred to above [56] serum T N F ~ of CIDP patients could not be detected and this may indicate either a difference in severity or sampling time in relation to disease onset, or a different pathogenetic mechanism [9]. The high serum TNFc~ value in 1 patient with post-herpetic neuropathy may be a further demonstration of the inflammatory process in this disease. TNFc~ produces haemorrhagic necrosis of tumours in vivo, and cytostatic or cytotoxic effects on transformed cells in vitro [37, 44]. It is also increased in the CSF of patients with central nervous systems neoplasia, such as metastatic melanoma [61]. The high CSF T N F ~ value in a patient with paraneoplasmatic neuropathy may reflect the immune activation against tumour cells. The high serum and CSF TNFff values in a patient with diabetic neuropathy are probably the result of a coincident infection. No correlation between TNFc~ levels and IgG index was found in our MS patients. The intrathecal synthesis of TNFc~ is probably not continuous during the myelin damage, and it might participate in lesion development by promoting demyelination, enhancing local immune responses [35]. There is conflicting evidence regarding the serum and CSF T N F ~ levels of MS patients [13, 14, 26, 35, 46, 55, 59, 61]. This can be explained by the different sensitivities of the methods applied [38], or by the variation in time of sampling after an acute exacerbation of the RR type, or in CSF and serum storage conditions, because TNF c~ has a limited half-life [12, 13]. The increased CSF TNFo~ levels could also precede the MS exacerbation and trigger off the demyelination process [3, 35]. The significance of TNFot detection in MS patients is not yet completely understood. TNFc~ may be produced in the central nervous system during an acute MS exacerbation in the RR or an increase on the Kurtzke Expanded Disability Scale for the CP form of the disease, but it can also be present in a number of other inflammatory conditions characterized by a demyelinating process, such as in chronic inflammatory polyneuropathy or GBS. However, further studies will hopefully clarify the possible relationship between TNFct accumulations and the clinical course of MS as well as the possible role of TNFo~ in the pathogenesis of this disease. 169 References 1. Arai K, Lee F, Miyajima A, et al. (1990) Cytokines: coordinators of immune and inflammatory responses. Annu Rev Biochem 59 : 783-836 2. Bansil S, Minthen FA, Cook SD, Sheffer A, Rohowsky Kochan C (1991) Clinical correlation with serum-soluble interleukin-2 receptor levels in GBS. Neurology 41 : 1302-1305 3. Beck J, Rondot P, Catinot L, Falcoff F, Kirchner H, Wietzerbin J (1988) Increased production of interferon-'/and TNF precedes clinical manifestation in MS: do cytokines trigger off exacerbations? Acta Neurol Scand 78:318-323 4. Brosnan CF, Selmaj K, Raine CS (1988) Hypothesis: a role for tumor necrosis factor in immune-mediated demyelination and its relevance to multiple sclerosis. J Neuroimmunol 18 : 87-94 5. Chensue SW, Remick DG, ShmyrForsch C, Beals TF, Kunkel SL (1988) Immunohistochemical demonstration of cytoplasmic and membrane-associated tumor necrosis factor in murine macrophages. Am J Pathol 133:564572 6. Dinarello CA, Mier JW (1987) Lymphokines. N Engl J Med 325 : 467-472 7. Dinarello CA, Cannon JG, Wolff SM et al. (1986) TNF (cachectin) is an endogenous pyrogen and induces production of IL-I. J Exp Med 163: 14331450 8. Dyck PJ, Lais AC, Ohta M, Bastron JA, Okazaki H, Groover RV (1975) Chronic inflammatory polyradiculopathy. Mayo Clin Proc 50:621-637 9. Dyck PJ, Arnason BGW (1984) Chronic inflammatory demyelinating polyradiculoneuropathy. In: Dyck PJ, Thomas PK, Lambert EH, Bunge R (eds) Peripheral neuropathy. Saunders Philadelphia, pp 2101-2115 10. Economou JS, McBride WH, Essner R, et al. (1989) Tumour necrosis factor production by IL2-activated macrophages in vitro and in vivo. Immunology 67 : 514-519 11.Exley AR, Smith N, Winer JB (1994) Tumour necrosis factor-c~ and other cytokines in Guillain-Barr6 syndrome. J Neurol Neurosurg Psychiatry 57 : 1118-1120 12. Ferraiolo BL, Moore JA, Crase D, Gribling P, Wilking H, Baughman RA (1988) Pharmacokinetics and tissue distribution of recombinant human TNFot in mice. Drug Metab Dispos 16: 270-275 13. Franciotta D, Grimaldi L, Martino GV, Piccolo G, Bergamaschi R, Citterio A, Melzi d'Evil GV (1989) TNF in serum and CSF of patients with MS. Ann Neurol 26 : 787-789 14. Gallo P, Piccinno MG, Kyralic L, Tavolato B (1989) TNFc~ and neurological diseases. Failure in detecting T N F ~ in the CSF from patients with MS, AIDS dementia complex and brain tumours. J Neuroimmunol 23 : 41-44 15. Golaz J, Steek A, Moretta L (1983) Activated T-lymphocytes in patients with multiple sclerosis. Neurology 33 : 1371-1373 16. Hafler DA, Fox DA, Manning ME, Schlossum SF, Reinherzand FL, Weiner HL (1985) In vivo activated T lymphocytes in the peripheral blood and CSF of patients with MS. N Engl J Med 312:1 17. Hartung HP, Toyka KV (1990) T cell and macrophage activation in experimental autoimmune neuritis (EAN) and the GBS. Ann Neurol 27 [Suppl] : 57-63 18. Hartung HP, Heininger K, Schafer B, et al (1988) Immune mechanisms in inflammatory polyneuropathy. Ann NY Acad Sci 540:122-161 19. Hartung HP, Hughes RAC, Taylor WA, Heininger K, Reiners K, Toyka KV (1990) T cell activation in Guillain-Barr6 syndrome and in MS: elevated serum levels of soluble IL2 receptors. Neurology 40 : 215-218 20. Hartung HP, Schafer B, Meide PH van der, Fierz W, Heininger K, Toyka KV (1990) The role of interferon-gamma in the pathogenesis of experimental autoimmune disease of the peripheral nervous system. Ann Neurol 2 7 : 2 4 7 257 21. Hartung HP, Schmidt B, Toyka KV (1991) Immune activation in GuillainBarr6 syndrome: cytokine studies (abstract). Ann Neurol 30 : 304 22. Hartung HP, Reiners K, Schmidt B, Stoll G, Toyka KV (1991) Serum interleukin-2 concentrations in GuillainBarr6 syndrome and CIDP: comparison with other neurological diseases of presumed immunopathogenesis. Ann Neurol 30 : 48-53 23. Hartung HP, Jung S, Stoll G, Zielasek J, Schmidt B, Archelos JJ, Toyka KV (1992) Inflammatory mediators in demyelinating disorders of the CNS and PNS. J Neuroimmunol 40:197-210 24. Hartung HP, Stoll G, Toyka KV (1993) Immune reactions in the peripheral nervous system. In: Dyck P, et al (eds) Peripheral neuropathy, 3rd edn. Saunders, Philadelphia, pp 418-444 25. Hauser SL, Blan AK, Gilles F, Kemp M, Kerr C, Wriner HL (1986) Immunohistochemical analysis of the cellular infiltrate in multiple sclerosis lesions. Ann Neurol 19:578-587 26. Hauser SL, Doolittle TH, Lincoln R, Brown RH, Dinarello CA (1990) Cytokine accumulations in CSF of MS patients. Frequent detection of IL- 1 and TNF but not IL-6. Neurology 40 : 1735-1739 27. Hofman FM, Hinton DR, Johnson K, Merill JE(1989) Tumor necrosis factor identified in multiple sclerosis. J Exp Med 170 : 607-612 28. Hughes RAC (1992) Immunological mechanisms of demyelination. J R Soc Med 85 : 53-57 29. Ilyas AA, Wilson HJ, Quarles RH et al (1988) Serum antibodies to gangliosides in GBS. Ann Neurol 23 : 440-447 30. Jiang H, Stewart CA, Fast DJ, Leu RW (1992) Tumor target-derived soluble factor synergizes with INF-y and IL2 to activate macrophages for tumor necrosis factor and nitric oxide production to mediate cytotoxicity of the same target. J Immunol 149 : 21372146 31. Koski CL, Chou DKH, Jungalwala FB (1989) Anti-peripheral nerve myelin antibodies in GBS bind a neutral glycolipid of peripheral myelin and crossreact with Forssman antigen. J Clin Invest 84 : 280-287 32. Laterre EC, Calletweart A, Heremans JF, Sfaello Z (1970) Electrophoretic morphology of gamma globulin in CSF in multiple sclerosis and other diseases of the nervous system. Neurology 20 : 982-990 33. Lieberman AP, Pith PM, Shin HS, Shin ML (1989) Production of tumor necrosis factor and other cytokines by astrocytes stimulated with lipopolysaccharide or a neurotropic virus. Proc Natl Acad Sci USA 34. Link H, Tibbling G (1977) Principle of albumin and IgG in neurological disorders. 2. Relation of the concentration of the proteins in serum and the CSF. Scand J Clin Lab Invest 37:391-395 35. Maimone D, Gregory S, Arnason BGW, Reder AT (1991) Cytokine levels in the CSF and serum of patients with MS. J Neuroimmunol 32 : 67-74 36. Maimone D, Annunziata P, Simone IL, Livrea P, Guazzi GC (1993) Interleukin-6 levels in the CSF and serum of patients with GBS and CIDP. J Neuroimmunol 47 : 55-62 37. Matthews N, Neale ML (1987) Studies on the mode of action of tumor necrosis factor on tumor cells in vivo. Lymphokines 14 : 223-252 38. McLaughlin PJ, Elmwood NJ, Ramadi LT, Pica MR, McKenzie IF (1990) Improvement in sensitivity of enzymelinked immunosorbent assay of TNF. Immunol Cell Biol 68:51-55 170 39. Merrill JE, Strom SR, Ellison GW, Myers L W (1989) in vitro study of mediators in MS. J Clin Immunol 9 : 8 4 96 40. Minz M, Rapaport R, Oleske JM, Connor EM, Koenigsberger MR, Denny T, Epstein LG (1989) Elevated serum levels of tumor necrosis factor are associated with progressive encephalopathy in children with acquired immunodeflciency syndrome. A m J Dis Child 143 : 771-774 41. Mizel SB (1989) The interleukines. FASEB J 3 : 2379-2388 42. Mustafa MM, Lebel MH, Ramilo O, Olsen KD, Reisch JS, Bentler B, McCracken G (1989) Correlation of interleukin-1 beta and cachectin concentrations in cerebrospinal fluid and outcome from bacterial meningitis. J Pediatr 1 1 5 : 2 0 8 - 2 1 3 43. Nedwin GE, Svedersky LP, Bringman TS, Palladino MA, Goedel DV (1985) Effect of interleukin 2, interferongamma and mitogens on the production of tumor necrosis factor ot and ~. J Immunol 135 : 2492-2497 44.North R J, Havell EA (1988) The antitumor function of tumor necrosis factor. 2. Analysis of the role of endogenous TNFc~ in endotoxin-induced haemorrhagic necrosis and regression of an established sarcoma. J Exp Med 167 : 1086-1099 45. Olsson JE, Nilsson K (1979) Gammaglobulins of CSF and serum in MS: isoelectric focusing on polyacrylamide gel and agar gel electrophoresis. Neurology 29:1383-1391 46. Peter JB, Boctor FN, Tourtelotte W W (1991) Serum and CSF levels of IL-2, SIL-2R, T N F ~ and IL-13 in chronic progressive multiple sclerosis: expected lack of clinical utility. Neurology 41 : 121-123 47. Poser CM, Paty DW, Scheinberg L, McDonald NI, Davis FA, Ebers GC, Johnson KP, Sibley WA, Silberberg DH, Tourtellotte W W (1983) New diagnostic criteria for multiple sclerosis: guidelines for research protocols. Ann Neurol 13 : 227-231 48. Reinherz EL, Weiner HL, Hauser HL, et al. (1980) Loss of suppressor T cells in active multiple sclerosis. N Engl J Med 303 : 125-129 49. Robbins DS, Shirazi Y, Drysdale BE, Lieberman A, Shin HS, Shin M L (1988) Production of cytotoxic factor for oligodendrocytes by stimulated astrocytes. J Immunol 139:2593-2597 50. Rostami A, Bruns JB, Brown MJ, Rosen J, Zweiman B, Lisac RP, Pleasure DE (1985) Transfer of experimental allergic neuritis with P2-specific Tcell lines. Cell Immunol 9 1 : 3 5 4 - 3 6 1 51. Said G, Hontebeyrie-Joskowicz M (1992) Nerve lesions induced by macrophage activation. Res Imnmnol 143 : 589-599 52. Schmidt B, Stoll G, Meide P van der, Jung S, Hartung HP (1992) Transient cellular expression of interferongamma in myelin-induced and T cell line-mediated experimental autoimmune neuritis. Brain 115:1633-1646 53. Sehnaj KW, Raine CS (1988) Tumor necrosis factor mediates myelin and oligodendrocyte damage in vitro. Ann Neurol 23 : 339 246 54. Selmaj KW, Raine CS, Cannella B, Brown CF (1991) Identification of lymphotoxin and TNF in MS lesions. J Clin Invest 87 : 949-954 55. Sharief MK, Hentges R (1991 ) Association between T N F a and disease progression in patients with MS. N Engl J Med 325 : 467-472 56. Sharief MK, McLean B, Thompson EJ (1993) Elevated serum levels of tumor necrosis factoro~ in GBS. Ann Neurol 33 : 591-596 57. Tracey KJ, Wei H, Manogue KR, Fong Y, Hesse DG, Ngugen HT, Kuo GC (1988) Cachectin/tumor necrosis factor induces cachexia, anemia and inflammation. J Exp Med 167 : 1211-1227 58. Traugott O, Scheinberg L, Rainer CS (1979) Multiple sclerosis; circulating antigen reactive lymphocytes. A n n Neurol 6 : 425-429 59. Tsukada N, Miyagi K, Matsuda M, Yanagisama N, Yone K (1991) TNF and 1L- 1 in the CSF and sera of patients with MS. J Neurol Sci 1 0 2 : 2 3 0 234 60. Waksman BH, Adams RD (1955) Allergic neuritis: an experimental disease of rabbits induced by the injection of peripheral nervous tissue and adjuvants. J Exp Med 1 0 2 : 2 1 3 - 2 3 6 61. Weller M, Stevens A, Sommer N, Melcus A, Dichgans J, Wietholter H (1991) Comparative analysis of cytokine patterns in immunological, infectious, and oncological neurological disorders. J Neurol Sci 104:215-221