Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
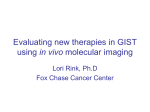
m i gateway Vol. 4 • Issue 4 • 2010 • 4 the newsletter of the snm center for molecular imaging innovation and translation Molecular and Cellular Imaging with Ultrasound Contrast Agents T oday, ultrasound imaging generally plays a minor role in molecular imaging. Most of the clinical activities are focused on PET and SPECT, and most of preclinical research is expanded to the areas of optical imaging and MRI. However, with proper contrast agents designed for molecular imaging, ultrasound can play an essential role both in research and clinical applications. Historically, ultrasound contrast imaging was suggested for visualization of blood flow patterns (1). Early-generation ultrasound contrast agents comprised air bubbles prepared by rapidly mixing air with aqueous saline, albumin or X-ray contrast media immediately (seconds) before intravascular administration (2). Air bubbles were echogenic but would quickly dissolve in the blood; bubbles would not pass through the pulmonary circulation, hence monitoring blood flow following intravenous administration had not been feasible with those contrast particles. Oth- er, sometimes exotic, microbubble preparation approaches were investigated, such as intravenous administration of H2O2 to generate oxygen bubbles in vivo, but they did not gain widespread use (3). Next, so-called first-generation contrast materials were much more stable and circulated longer than uncoated air bubbles because they were stabilized with a surfactant or a protein shell (4). They were capable of transpulmonary passage, so blood flow characterization after intravenous administration became feasible, although circulation time of air-filled bubbles was generally quite short and these contrast agents did not gain much recognition in clinical use. Significant clinical use of microbubbles for blood pool enhancement became possible less than a decade ago, with the approval of second-generation contrast agents, which contained water-insoluble fluorinated gases (5, 6) (7). These materials stayed in the bloodstream for minutes, not seconds, so, viable in vivo imaging studies have been performed. The features (such as circulation time) and structure (such as the shell to which targeting ligands can be coupled) of these second-generation microbubbles are quite acceptable for the design of the molecular ultrasound imaging contrast materials, which target the specific molecular markers of disease. Particle size constraints apply to the design and applicability of molecular imaging ultrasound contrast agents to achieve successful imaging. In most cases, these materials are gas-filled microbubbles with the size of several microns. These particles, with a picogram mass, are detected by ultrasound very well, to the level of imaging individual particles in the suspended state and even after binding to the target (8). Submicron gas bubbles possess much worse stability and circulation time; they are not as echogenic as larger bubbles. Therefore, preferred contrast particle size is 2-4 um (larger microbubbles may lodge in the capillaries, e.g., in the lungs). It means Amyloid in the Brain Continued on page 2. See Ultrasound Contrast Agents. PET Drugs and Part 212 Requirements T PET drug he FDA, taking into consideration the unique nature of PET drugs and production, published the final rule, 21 CFR Part 212 “Current Good Manufactur ing Practice (CGMP) for PET drugs” on December 10, 2009 (Federal Register/Vol.74/ December 10, 2009, p.65409). Part 212 is the rule (or regulation) and contains binding guidance requirements for the CGMP for PET drugs and is enforceable in the courts. The “PET drugs…CGMP” published at the same time as Part 212 describes FDA’s current thinking on specific approaches to comply with Part 212 requirements (Federal Register/ Vol.74/December 10, 2009, p.65538). Part 212 requires that producers of PET drugs for clinical use must be compliant with the rule by December 12, 2011––and that is only Continued on page 5. See PET Drugs and Part 212. in this issue Images of Interest 3 Tech Sector 4 YI Contribution 5 Donor Corner 6 MI Calendar 8 Ultrasound Contrast Agents. Continued from page 1. 2011 Molecular Imaging Meetings Multimodality Molecular Imaging of Prostate Cancer Friday, January 21, 2011 Palm Springs, California Part of the SNM 2011 Mid-Winter Meetings www.snm.org/prostate2011 Clinical Trials Network Workshop January 20–21, 2011 Palm Springs, California www.snm.org/ctn2011 Breast Cancer Imaging: State of the Art 2011 Diagnosis, Therapy and Beyond April 21-22, 2011 Bethesda, Maryland 2 The Natcher Center National Institutes of Health www.snm.org/breast2011 Lost and Found in Translation: Translating Your Optical and Radiopharmaceutical Agents into the Clinic, a Categorical Seminar June 4, 2011 San Antonio, Texas SNM Annual Meeting www.snm.org/am m i images of interest Ultrasound Contrast Agents. Continued from page 1. that successful molecular imaging with current generation of microbubble contrast agents is possible only for intravascular markers, and ultrasound contrast detection of a specific cellular marker is not feasible if that marker is not exposed to the bloodstream and is located at the interstitial space or inside the target cell. Design of Microbubbles for Molecular Imaging Over the past 15 years, dozens of papers describing molecular imaging with ultrasound contrast have appeared, presenting targeting to a variety of the disease marker molecules. General design of the particle has not changed significantly since its first presentation (9). Targeting ligand is attached to the microbubble shell-forming material, then microbubbles are generated from insoluble gas during high-shear mixing, e.g., with a probe-type sonicator. During the preparation procedure, microbubbles are immediately covered with the shell. After removal of excess ligand by centrifugal flotation, microbubble targeting is either tested in vitro or injected intravenously in the experimental animals with the appropriate disease models. Most successful and popular targeted microbubble shell design is based on a lipid monolayer shell decorated with a grafted brush of the water-soluble polyethylene glycol. The thickness of the lipid monolayer is ~2 nm. This thin shell does not interfere significantly with microbubble expansion and contraction in the ultrasound field, providing good contrast echogenicity without the need to destroy the particles by cracking the shell with high-power ultrasound. This shell does not serve as a significant barrier for gas diffusion in and out of the bubble. PEG chains extend from the microbubble surface into the surrounding aqueous environment by ~10-30 nm, which is not very significant when compared with a 2-3 um particle diameter (10). Targeting ligand is usually attached to the exterior of the PEG brush in the same extended “fishing line” manner as it was earlier proposed for liposomes (11). This ligand coupling technique facilitates ligand-receptor interaction and improves microparticle targeting in a flow-through scenario (12). Peptides/mimetics, carbohydrates, glycosulfopeptides, small and large proteins (such as antibodies) were successfully tested as ligands for ultrasound molecular imaging. Most of such tests required biotinylated ligand that would attach to the bubble via a streptavidin spacer (13); many biotinylated ligands are available commercially or can be prepared easily. The advantage of biotin-streptavidin ligand linking technique is in its simplicity; bubbles can be easily centrifuged to remove excess of free ligand. This approach is especially useful if the ligand is a large protein that could become denatured and inactivated during microbubble preparation by sonication as described in the previous paragraph. However, there is a very significant disadvantage. Streptavidin, as a foreign protein, will not be approved for clinical application in human setting. Therefore, chemical coupling between ligand and shell has to take place, either before (as described above) or after bubble preparation. The choice of ligands for microbubble targeting may be determined not just by the specificity and affinity of ligand-receptor interaction for the respective molecular markers (thermodynamics), but also by how fast the ligand-receptor interaction takes place (kinetics). Antibodies are usually selected via ELISA, by the value of equilibrium affinity, often described as equilibrium dissociation constant, Kd; however, the act of interaction of ligand-microbubble with the receptor on the vessel wall is a rather timeconstrained event, and if the kinetics of association between the ligand and receptor is slow, the microbubble would be transported away from the target area and would not attach to the intended target. Therefore, the choice of fast-binding ligands, such as glycosulfopeptide portion of the natural molecule P-Selectin Glycoprotein Ligand 1 (PSGL-1, (14)) or even simpler molecules such as sialyl Lewis X, (15) could be considContinued on page 3. See Ultrasound Contrast Agents. www.molecularimagingcenter.org/ mi Molecular Ultrasound Imaging of Tumor Angiogenesis Visistar-Integrin microbubbles (cRGD peptide) Visistar-Integrin Control microbubbles (cRAD peptide) 8 min after intravenous injection of 50 million microbubbles. Sequoia 512 imaging system with 15L8 probe, operated in CPS mode Ultrasound molecular imaging of tumor angiogenesis in an orthotopic mouse model of breast cancer (Met-1 cells implanted in mammary fat pad). Microbubbles bearing a cyclic RGD peptide ligand (Visistar-Integrin, directed at avb3 integrin on tumor vascular endothelium) or a control ligand (cyclic RAD peptide) covalently conjugated to the bubble shell were administered intravenously and allowed to circulate and clear from the bloodstream over eight minutes. Targeted microbubbles accumulated within the tumor. Control microbubbles exhibited negligible accumulation. Dotted line delineates tumor borders, as determined by B-mode ultrasound. Images courtesy of Xiaowen Hu and Katherine Ferrara (University of California, Davis); Visistar-Integrin microbubbles provided by Joshua Rychak (Targeson, San Diego). Ultrasound Contrast Agents. Continued from page 2. ered. Interestingly, the latter has equilibrium Kd ~ 1mM for P- or E-selectin. Such low affinity is not useful for targeting of small molecules. However, successful particle targeting is possible via a combination of rapid association between the ligand and receptor, and cooperative multipoint interaction between large number of ligand and receptor molecules. Placing over a million small ligand molecules per single microbubble is feasible. Only ~105 (or less) antibody molecules attached per microbubbles is typically reported (13). Using full IgG molecule (MW=150,000) for immobilization on the microbubble surface may not be the best strategy as compared with the use of smaller ligands: larger molecules carry much more than just the target binding sequence. Fc fragment of the antibody may be quite immunogenic, so the use of humanized (or fully human) antibodies is required. Furthermore, Fc receptors on phagocytic cells (e.g., in the liver) may alter microbubble biodistribution in an undesirable way. Overall, the use of smaller molecules as ligands for molecular ultrasound imaging should be preferred. In Vivo Molecular Imaging with Microbubble Contrast Agents There are many useful intravascular molecular targets that mark disease tissue location; most of them are affiliated, directly or indirectly, with endothelial cells, and constitute markers of inflammation (such as ICAM-1 (16), VCAM-1 (17), MAdCAM-1 (18), P- or E-selectin (13)) or angiogenesis (VERFR2 (19), αvβ3 (20)). Blood clot markers, such as platelet GPIIbIIIa (21) and P-selectin (22) and activated form of endothelial von Willebrand Factor (23) can also serve as useful targets of disease. A wide array of molecular imaging ultrasound contrast studies have been performed to date in animal models. Imaging procedure is quite straightforward, but somewhat different when compared with other molecular imaging modalities. Targeted microbubble construct aqueous dispersion (or control non-targeted preparation) is injected intravenously as a bolus, and low-power contrast ultrasound imaging of the region of interest is performed immediately. Contrast inflow imaging provides real-time information of the blood flow patterns in the tissue of interest, and may be useful for immediate understanding of the target tissue physiology. Several minutes later, imaging of microbubbles that have accumulated in the tissue can be performed. By that time, repeated circulation of the injected microbubbles through the body vasculature results in the selective binding of a fraction of the injected bubbles to the target, e.g., disease tissue. Continued on page 7. See Ultrasound Contrast Agents. 3 Ultrasound Contrast Agents. Continued from page 1. 2011 Molecular Imaging Meetings Multimodality Molecular Imaging of Prostate Cancer Friday, January 21, 2011 Palm Springs, California Part of the SNM 2011 Mid-Winter Meetings www.snm.org/prostate2011 Clinical Trials Network Workshop January 20–21, 2011 Palm Springs, California www.snm.org/ctn2011 Breast Cancer Imaging: State of the Art 2011 Diagnosis, Therapy and Beyond April 21-22, 2011 Bethesda, Maryland 2 The Natcher Center National Institutes of Health www.snm.org/breast2011 Lost and Found in Translation: Translating Your Optical and Radiopharmaceutical Agents into the Clinic, a Categorical Seminar June 4, 2011 San Antonio, Texas SNM Annual Meeting www.snm.org/am m i images of interest Ultrasound Contrast Agents. Continued from page 1. that successful molecular imaging with current generation of microbubble contrast agents is possible only for intravascular markers, and ultrasound contrast detection of a specific cellular marker is not feasible if that marker is not exposed to the bloodstream and is located at the interstitial space or inside the target cell. Design of Microbubbles for Molecular Imaging Over the past 15 years, dozens of papers describing molecular imaging with ultrasound contrast have appeared, presenting targeting to a variety of the disease marker molecules. General design of the particle has not changed significantly since its first presentation (9). Targeting ligand is attached to the microbubble shell-forming material, then microbubbles are generated from insoluble gas during high-shear mixing, e.g., with a probe-type sonicator. During the preparation procedure, microbubbles are immediately covered with the shell. After removal of excess ligand by centrifugal flotation, microbubble targeting is either tested in vitro or injected intravenously in the experimental animals with the appropriate disease models. Most successful and popular targeted microbubble shell design is based on a lipid monolayer shell decorated with a grafted brush of the water-soluble polyethylene glycol. The thickness of the lipid monolayer is ~2 nm. This thin shell does not interfere significantly with microbubble expansion and contraction in the ultrasound field, providing good contrast echogenicity without the need to destroy the particles by cracking the shell with high-power ultrasound. This shell does not serve as a significant barrier for gas diffusion in and out of the bubble. PEG chains extend from the microbubble surface into the surrounding aqueous environment by ~10-30 nm, which is not very significant when compared with a 2-3 um particle diameter (10). Targeting ligand is usually attached to the exterior of the PEG brush in the same extended “fishing line” manner as it was earlier proposed for liposomes (11). This ligand coupling technique facilitates ligand-receptor interaction and improves microparticle targeting in a flow-through scenario (12). Peptides/mimetics, carbohydrates, glycosulfopeptides, small and large proteins (such as antibodies) were successfully tested as ligands for ultrasound molecular imaging. Most of such tests required biotinylated ligand that would attach to the bubble via a streptavidin spacer (13); many biotinylated ligands are available commercially or can be prepared easily. The advantage of biotin-streptavidin ligand linking technique is in its simplicity; bubbles can be easily centrifuged to remove excess of free ligand. This approach is especially useful if the ligand is a large protein that could become denatured and inactivated during microbubble preparation by sonication as described in the previous paragraph. However, there is a very significant disadvantage. Streptavidin, as a foreign protein, will not be approved for clinical application in human setting. Therefore, chemical coupling between ligand and shell has to take place, either before (as described above) or after bubble preparation. The choice of ligands for microbubble targeting may be determined not just by the specificity and affinity of ligand-receptor interaction for the respective molecular markers (thermodynamics), but also by how fast the ligand-receptor interaction takes place (kinetics). Antibodies are usually selected via ELISA, by the value of equilibrium affinity, often described as equilibrium dissociation constant, Kd; however, the act of interaction of ligand-microbubble with the receptor on the vessel wall is a rather timeconstrained event, and if the kinetics of association between the ligand and receptor is slow, the microbubble would be transported away from the target area and would not attach to the intended target. Therefore, the choice of fast-binding ligands, such as glycosulfopeptide portion of the natural molecule P-Selectin Glycoprotein Ligand 1 (PSGL-1, (14)) or even simpler molecules such as sialyl Lewis X, (15) could be considContinued on page 3. See Ultrasound Contrast Agents. www.molecularimagingcenter.org/ mi Molecular Ultrasound Imaging of Tumor Angiogenesis Visistar-Integrin microbubbles (cRGD peptide) Visistar-Integrin Control microbubbles (cRAD peptide) 8 min after intravenous injection of 50 million microbubbles. Sequoia 512 imaging system with 15L8 probe, operated in CPS mode Ultrasound molecular imaging of tumor angiogenesis in an orthotopic mouse model of breast cancer (Met-1 cells implanted in mammary fat pad). Microbubbles bearing a cyclic RGD peptide ligand (Visistar-Integrin, directed at avb3 integrin on tumor vascular endothelium) or a control ligand (cyclic RAD peptide) covalently conjugated to the bubble shell were administered intravenously and allowed to circulate and clear from the bloodstream over eight minutes. Targeted microbubbles accumulated within the tumor. Control microbubbles exhibited negligible accumulation. Dotted line delineates tumor borders, as determined by B-mode ultrasound. Images courtesy of Xiaowen Hu and Katherine Ferrara (University of California, Davis); Visistar-Integrin microbubbles provided by Joshua Rychak (Targeson, San Diego). Ultrasound Contrast Agents. Continued from page 2. ered. Interestingly, the latter has equilibrium Kd ~ 1mM for P- or E-selectin. Such low affinity is not useful for targeting of small molecules. However, successful particle targeting is possible via a combination of rapid association between the ligand and receptor, and cooperative multipoint interaction between large number of ligand and receptor molecules. Placing over a million small ligand molecules per single microbubble is feasible. Only ~105 (or less) antibody molecules attached per microbubbles is typically reported (13). Using full IgG molecule (MW=150,000) for immobilization on the microbubble surface may not be the best strategy as compared with the use of smaller ligands: larger molecules carry much more than just the target binding sequence. Fc fragment of the antibody may be quite immunogenic, so the use of humanized (or fully human) antibodies is required. Furthermore, Fc receptors on phagocytic cells (e.g., in the liver) may alter microbubble biodistribution in an undesirable way. Overall, the use of smaller molecules as ligands for molecular ultrasound imaging should be preferred. In Vivo Molecular Imaging with Microbubble Contrast Agents There are many useful intravascular molecular targets that mark disease tissue location; most of them are affiliated, directly or indirectly, with endothelial cells, and constitute markers of inflammation (such as ICAM-1 (16), VCAM-1 (17), MAdCAM-1 (18), P- or E-selectin (13)) or angiogenesis (VERFR2 (19), αvβ3 (20)). Blood clot markers, such as platelet GPIIbIIIa (21) and P-selectin (22) and activated form of endothelial von Willebrand Factor (23) can also serve as useful targets of disease. A wide array of molecular imaging ultrasound contrast studies have been performed to date in animal models. Imaging procedure is quite straightforward, but somewhat different when compared with other molecular imaging modalities. Targeted microbubble construct aqueous dispersion (or control non-targeted preparation) is injected intravenously as a bolus, and low-power contrast ultrasound imaging of the region of interest is performed immediately. Contrast inflow imaging provides real-time information of the blood flow patterns in the tissue of interest, and may be useful for immediate understanding of the target tissue physiology. Several minutes later, imaging of microbubbles that have accumulated in the tissue can be performed. By that time, repeated circulation of the injected microbubbles through the body vasculature results in the selective binding of a fraction of the injected bubbles to the target, e.g., disease tissue. Continued on page 7. See Ultrasound Contrast Agents. 3 SNM is now accepting abstracts for the 2011 Annual Meeting, June 4-8 in San Antonio, TX. This premier event offers physicians, scientists, technologists, lab professionals, and educators/course directors in the field of nuclear medicine and molecular imaging the ideal platform to present scientific research to an audience of medical imaging professionals from around the world. call Abstracts Abstract Submission Deadline: JAnuAry 7 2011 for DONOR CORNER MI Innovations Increase Efficiency and Reduce Exam Times without Compromise 6 M olecular imaging has the potential to transform health care by shifting the focus from treating disease to enabling early health. At RSNA 2010, GE Healthcare demonstrated several innovative molecular imaging technologies designed to increase workflow efficiency and overall image quality, while reducing exam times and improving dose management. By combining the power of anatomical and functional scanning with biological tracers, GE is helping health care providers to detect and diagnose disease earlier, and to evaluate treatment efficacy more quickly. Molecular imaging also directly impacts patient care by allowing physicians to tailor specific treatments to individual patients, which in turn will mean that health care dollars are more efficiently spent to save lives. With tri-modality imaging, researchers and clinicians have the potential to improve small lesion detection, image quality and therapy response monitoring to understand disease from the beginning. It is important to demonstrate industry commitment to improving the patient experience while maintaining clinical excellence and quality. By applying innovation, we can significantly shorten traditional exam times and reduce dose to improve the patient experience without compromising a clinician or researcher’s ability to understand and treat disease effectively. Terri Bresenham Vice-President of Molecular Imaging at GE Healthcare www.molecularimagingcenter.org/ mi 2011 Annual Meeting San Antonio, TX June 4-8, 2011 SNM 2011 Mid-Winter Meetings Offer Comprehensive Prostate Cancer Symposium SNM’s Center for Molecular Imaging Innovation and Translation (CMIIT) is hosting the Multimodality Molecular Imaging of Prostate Cancer Symposium on Jan. 21, 2011. This one-day symposium brings together individuals from multiple clinical and scientific disciplines to provide an up-to-date survey of best practices for the diagnosis and treatment of patients with prostate cancer. The symposium will address the need for synergism between diagnostic radiology, nuclear medicine and the new molecular imaging modalities. Lectures will emphasize the role of imaging in enabling better treatment selection and evaluation and, importantly, the ideal approach to assessing response to treatment. Ultrasound Contrast Agents. Continued from page 3. The majority of contrast agent is not likely to adhere to the molecular marker of disease and is recirculating with the blood flow. Microbubble shell is too thin to be a good barrier for air diffusion into the bubble and fluorocarbon diffusion out of the bubble. As microbubble contrast passes through the lungs, gas exchange with the surrounding medium takes place; most of the fluorocarbon gas is exchanged out of the bubbles and exhaled within minutes of intravenous administration. Residual air in the bubbles does not support good stability in vivo, it diffuses out and shell collapses, making the particle non-echogenic. Targeted bubbles, adhered e.g., to tumor vasculature, are not exposed to fast flow convection conditions that support rapid gas exchange during circulation, so we can hypothesize that loss of gas from targeted bubbles would be slower. This process can contribute to the improvement of signalto-noise (e.g., target-to-blood) localization ratio. So at 5-15 minutes after microbubble administration, most of the circulating bubbles have cleared from the bloodstream, and imaging of adhered bubble can be performed. Modern contrast modes (such as Contrast Pulse Sequencing or Pulse Inversion Amplitude Modulation) implemented on many ultrasound imaging systems allow to suppress the signal from the tissue itself, and observe microbubbles with excellent detection sensitivity in real time at low power without contrast destruction (ultrasound Mechanical Index <0.2). After observing the targeted bubble in the particular imaging plane(s), ultrasound power can be increased, and adhered bubbles destroyed. Reduction of the acoustic backscatter signal after destructive pulse can serve as an additional proof of microbubble targeting; within seconds after reduction of Mechanical Index, we can observe residual circulating bubbles still present in the bloodstream. Nearly all of the molecular ultrasound imaging studies described in the literature so far have been performed in rodent animal models. Publications of molecular ultrasound imaging studies on larger animals are quite rare. There is one exception––a clinically approved agent that is routinely used for Kupffer cell targeting, Sonazoid (perflubutane microbubbles). It is approved for targeted ultrasound contrast in the liver radiology setting in Japan. It is estimated that several hundred thousand patients have received this contrast agent since its approval. Sonazoid accumulation in normal liver parenchyma is achieved via phosphatidylserine targeting: Sonazoid microbubble consists of phosphatidylserine shell and perfluorobutane gas. As phosphatidylserine is the natural marker of apoptosis, its presence on the outer surface of a particle or a cell makes that surface an immediate target for phagocytic uptake (24) (25, 26). In the normal liver tissue but not in the lesion foci, Kupffer cells are present and can capture circulating microbubbles and allow better disease characterization by “negative” target enhancement, as compared with unenhanced ultrasound or dynamic CT (27). This “late-phase” ultrasound imaging is performed to detect bubbles that have targeted to the normal liver tissue of interest following the clearance of circulating bubbles from the bloodstream, several minutes after bolus intravenous administration. As phosphatidylserine-targeted microbubbles are taken up by any phagocytic cells, they can be applied not only for liver radiology, but also for imaging of adherent neutrophils in the acute inflammation (28) or ischemia/reperfusion injury scenarios (29). Cell Labeling for Ultrasound Contrast Imaging As described in the previous paragraph, in vivo cell-specific labeling is already becoming a useful clinical tool in liver radiology studies. It serves as proof that ex vivo cell labeling with microbubble agents can also be performed, e.g., for stem cell or dendritic cell therapy research, as is now popular for optical, MRI and SPECT imaging modalities. Several groups by now have presented ultrasound contrast materials such as microbubbles and liquid fluorocarbon nanoparticle emulsions (30) for contrast labeling of cells for ultrasound contrast imaging. One interesting example of in vivo selective cell labeling is provided for circulating cells that are tagged with ligand-carrying microbubbles after intravenous administration (31). The ability to detect microbubbles by ultrasound even after their uptake in the cell has been proven experimentally a decade ago (32); we can expect that after intracellular uptake, microbubbles will not lose their gas core as rapidly as free circulating or even target-adherent bubbles; anecdotal evidence suggests that echogenicity of microbubbles in the liver have significant longevity, perhaps due to intracellular uptake. Currently, this area is rapidly developing, with the general goal of preparing labeled cell samples to be monitored by ultrasound imaging for an extended period of time (days). Conclusion In conclusion, molecular/cellular imaging with ultrasound contrast agents represents a rapidly developing area of research. A combination of equipment portability, low cost and excellent contrast detection sensitivity by ultrasound imaging, in concert with the ability to detect molecular markers of disease in real time, will very likely lead to the development of molecular imaging contrast agents for widespread clinical application for diagnostic imaging and image-guided therapy. A complete list of references for this article can be found at http://www.molecularimagingcenter.org/docs/Gateway_Lead_ Article_US_Contrast-Klibanov.pdf Alexander (Sasha) L. Klibanov, PhD Associate Professor, Division of Cardiovascular Medicine and Department of Biomedical Engineering, University of Virginia 7